


Abstract
Background/Aim: We performed a phase II study of triple-drug combination chemoradiotherapy (DCF-R therapy), in which docetaxel was added to the standard chemoradiotherapy (cisplatin [CDDP]/5-fluorouracil [5-FU]) for unresectable advanced esophageal cancer. Patients and Methods: Sixty-one patients with unresectable advanced esophageal cancer underwent the following DCF-R therapy: intravenous infusion of l60 mg/m2 docetaxel and 60 mg/m2 of CDDP (day 1), and 600 mg/m2 of 5-FU (days 1-5); 2 courses administered within a 4-week interval. Radiotherapy comprised 60 Gy in total. Results: Response rates were 85.2% for the main lesion, 80.7% for metastasized lymph nodes, and 67.6% for distant organ metastases. Common adverse effects were leukopenia, anemia, and nausea, in 98.4%, 62.3%, and 60.7% of patients, respectively. Treatment completion rate was 90.2% and no treatment-associated deaths occurred. Median survival time was 406 days and 1-, 2-, and 5-year survival rates were 58.6%, 39.1%, and 22.8%, respectively. Conclusion: DCF-R therapy for unresectable advanced esophageal cancer demonstrated a high antitumor effect with sufficient safety.
Treatment outcomes of esophageal cancer have improved due to advances in diagnostic techniques, such as chromoendoscopy and magnifying endoscopy, in surgical devices and techniques, including thoracoscopy and surgical robots, and in perioperative management techniques. However, treatment outcome remains poor in patients with metastases, and especially in those with unresectable metastatic lesions. We have performed triple-drug combination chemotherapy (DCF therapy) adding docetaxel (DTX) to the conventional combination of cisplatin (CDDP)+5-fluorouracil (5-FU) for unresectable esophageal cancer, since 2003 (1). The response rate of metastasized lymph nodes and distant metastatic lesions to DCF therapy exceeded 70%, the treatment outcome greatly surpassed that of the conventional 2-drug combination therapy using CDDP and 5-FU, and safety was also confirmed. A strong antitumor effect on the main lesion was also observed, but the complete response (CR) rate was equivalent to or did not reach that of chemoradiotherapy in which radiation was added to the 2 drugs (2, 3), and early tumor regrowth occurred in a considerable number of patients despite the effectiveness of therapy. Aiming at acquiring a higher therapeutic effect, we planned chemoradiotherapy in which radiation therapy with superior local tumor was added to the triple-drug combination chemotherapy using CDDP, 5-FU, and DTX, and performed a phase I study in 2007 to 2008 (4), in which tolerability was investigated based on the occurrence of adverse events as an index, and determined a recommended dose. In the present study, based on the results of the phase I study, we performed a phase II study and investigated the efficacy and safety of our chemoradiotherapy regimen.
Patients and Methods
Patients. Of the patients with untreated unresectable esophageal cancer accompanied by the invasion of other organs (T4b) or distant metastasis (M1) (7th edition of the Union for International Cancer Control classification) (5) who were admitted to our Department between January 2009 and December 2017, 61 patients who met the following criteria were included in the study: 1) pathological diagnosis was esophageal squamous cell carcinoma, 2) the presence of an evaluable lesion, 3) aged between 20 and 80 years old, 4) performance status (PS) (Eastern Cooperative Oncology Group classification) of 0-1, 5) retention of major organ functions. Furtheremore should have met the following laboratory test values: 1) neutrophils >2,000/mm3, 2) white blood cells >4,000/mm3, 3) hemoglobin >9.0 g/dl, 4) platelets >10×104/mm3, 5) total bilirubin level within the normal range, 6) glutamic oxaloacetic transaminase, glutamic pyruvic transaminase: 1.5 times or lower than the normal values, 7) alkaline phosphatase: 2.5 times or lower than the normal value, 8) serum creatinine: 1.5 times or lower than the normal value, and 9) provided consent.

Treatment schedule.
Patients were excluded if they had any of the following conditions: a history of serious allergic reaction to these chemotherapeutic agents; severe general medical conditions that may prevent scheduled chemoradiotherapy; pregnancy, possible pregnancy, or breastfeeding; active febrile infections; any other conditions for which the attending physician judged that the patient was ineligible.
The study was approved by the Ethics Committee of Tokyo Medical University. All patients provided written informed consent.
Pretreatment evaluation. Before treatment, patients were evaluated by their medical history, physical examination, blood count, blood biochemistry, tumor markers, electrocardiography, chest radiography, barium esophagography, esophagoscopy, and contrast-enhanced computed tomography (CT) scan of the neck, thorax, and abdomen. Ultrasonography of the neck or abdomen, bronchoscopy, bone scintigraphy, and endoscopic ultrasonography were optionally performed according to the tumor status. The clinical staging of the tumors was defined according to the TNM classification for malignant tumors (7th edition) staging system.
Treatment plan. The treatment schedule is shown in Figure 1.
Chemotherapy with DTX, CDDP, and 5-FU. DTX was administered intravenously for 1 hour and CDDP was administered for 2 hours after the completion of the DTX infusion on day 1. On days 1 to 5, 5-FU was administered as a protracted intravenous infusion. Two cycles of chemotherapy were administered every 4 weeks. Doses were set to those determined by the phase I study, i.e., DTX, 60 mg/m2 (day 1); CDDP, 60 mg/m2 (day 1); 5-FU, 600 mg/m2 (days 1-5). The discontinuation criteria of chemotherapy were as follows: 1) development of a severe adverse effect, 2) clear progression of the disease, and 3) other conditions judged to make continuation of chemotherapy difficult.
Radiotherapy. Treatment planning consisted of a CT scan of the esophagus of 0.5-cm thick slices. Gross tumor volume (GTV) 1 and GTV 2 were defined as that of the primary tumor, and of the lymph nodes with a maximum diameter of 1.5 cm or more in the cervix, mediastinum, and abdomen, respectively. The clinical target volume (CTV) was determined as GTV 1 with a 3-cm expansion superiorly and inferiorly along the length of the esophagus and a 1.0 to 1.5-cm radial expansion plus GTV 2 with a 1.5-cm radial expansion in all directions. The planned treatment volume (PTV) was established by adding a 0.5 to 1.0-cm margin to the CTV. Patients were treated daily 5 times per week. The PTV was irradiated using a parallel opposed field of up to 40 Gy administered in 20 sessions. Then, the PTV was irradiated with a total dose of 60 Gy administered in 30 sessions, using 2 or 3 ports to avoid the spinal cord. Radiotherapy was suspended if the patient developed grade 3 or 4 leukocytopenia.
Response evaluation and monitoring. Four weeks after the completion of the treatment, the clinical response of each patient was assessed by esophagoscopy and CT scans. The responses at the primary site were evaluated by esophagoscopy according to the response evaluation criteria of the Japanese Esophageal Society. Briefly, a CR was defined as complete tumor disappearance and absence of viable cells in biopsy samples. An incomplete response/stable disease (SD) was defined as incomplete tumor disappearance without tumor progression. A partial response (PR) referred to a 50% or more decrease in the tumor, SD was defined as less than a 50% decrease or less than a 25% increase in the tumor, and progressive disease (PD) was defined as a 25% or more increase in the primary tumor. The responses of the metastatic lesions were evaluated according to the Response Evaluation Criteria in Solid Tumors. Adverse reactions were evaluated by the National Cancer Institute Common Toxicity Criteria (version 4.0) (6).
After evaluation of the clinical response, the patients were subsequently evaluated every 3 months for the first 2 years and every 6 months for the next 3 years. This evaluation included a physical examination, full blood analysis, CT scan, and esophagoscopy. Late radiation toxicities were assessed using the US Radiation Therapy Oncology Group (RTOG)/European Organisation for Research and Treatment of Cancer late radiation morbidity scoring scheme.
Statistical analysis. Actual survival rates were calculated by the Kaplan-Meier method.
Results
Patient characteristics. Table I shows the characteristics of the patients. Factors indicating unresectability were tumor stage T4 in 51 patients, and tumor stage M1 in 34 patients (Table I). Table II lists the details of the stage T4 and M1 organs. In patients with stage T4 tumors, both bronchi and large vessels were infiltrated, and in patients with M1 tumors, distant lymph nodes metastasis (M1Lym) and metastasis to the lung were found in 4 patients, M1Lym and metastasis to the liver in 1 patient, and lung and liver metastases in 4 patients (Table II).
Clinical efficacy (effective rate). The clinical effect on the primary lesion was CR in 29 (47.5%), PR in 23 (37.7%), SD in 2 (3.3%), and PD in 7 patients (11.3%), and the response rate was 85.2%. The clinical effect on metastasized lymph nodes was CR in 18 (31.6%), PR in 28 (49.1%), SD in 2 (3.5%), and PD in 9 patients (15.8%), and the response rate was 80.7% The judgment of the clinical effect on metastatic lesions in distant organs was CR in 10 (29.4%), PR in 13 (38.2%), SD in 1 (2.9%), and PD in 10 patients (29.4%), and the response rate was 67.6%. The overall response rate was 75.4% (Table III).
Adverse reactions. Regarding grade 1 or severer adverse effects, based on the National Cancer Institute Common Toxicity Criteria, included hematotoxicity: leukopenia in 60 (98.4%), anemia in 38 (62.3%), and thrombocytopenia in 14 patients (23.0%). As non-hematotoxicity, the following adverse reactions were observed: nausea in 37 (60.7%), hair loss in 33 (54.1%), stomatitis in 22 (36.1%), esophagitis in 18 (29.5%), diarrhea in 17 (27.9%), hyponatremia in 10 (16.4%), impairment of renal function in 6 (9.8%), hypokalemia in 5 (8.2%), impairment of liver function in 4 (6.6%), anorexia in 2 (3.3%), hypercalcemia in 1 (1.6%), and dermatitis in 1 patient (1.6%) (Table IV). The treatment completion rate was 90.2%.
Treatment after DCF-R therapy. Treatment after DCF-R therapy was surgery in 3 patients (esophagectomy via right thoracotomy in 2 and transhiatal esophagectomy in 1), chemotherapy in 39 (DCF therapy in 30 and CDGP/PTX therapy in 9), esophageal stent insertion in 6, and no treatment was performed in 13 patients.
Prognosis. The median survival time was 406 days and the 1-year, 2-year, and 5-year survival rates were 58.6%, 39.1%, and 22.8%, respectively. The cause of death was primary or other diseases and no treatment-associated deaths occurred (Figure 2).
Patient characteristics.
Cancer invasion and distant metastasis to other organs.
Discussion
To date, esophageal cancer has been treated with surgery, radiotherapy, chemotherapy, as well as a combination of these (7). With the recent progression in diagnostic technology, the diagnosis of esophageal cancer in its early stages has increased, and endoscopic treatment is now actively performed (8). However, there is still a considerable number of patients that show invasion of the great vessels and airway system or metastasis to other organs and distant lymph nodes at the time of diagnosis, who are judged as advanced cases and are excluded from surgical indication (9). For these cases of highly advanced esophageal cancer, a randomized controlled study (RTOG8501) was performed by the RTOG and it was clarified that chemoradiotherapy significantly increased the survival rate compared with that of patients treated with irradiation therapy alone (10-12). Based on these results, chemoradiotherapy is presently regarded as the standard treatment for unresectable advanced esophageal cancer, also in Japan. Ohtsu et al. (2) have performed a phase II study of CDDP+5FU combination chemoradiotherapy for T4/M1Lym esophageal cancer and reported that the CR rate was 33%, the median survival time was 9 months, and the 2-year survival rate was 34%. Ishida et al. (3) have also performed a multicenter phase II study of CDDP+5FU combination chemoradiotherapy for T4/M1Lym esophageal cancer and reported that the CR rate was 15%, the median survival time was 10 months, and the 2-year survival rate was 31.5%, showing almost the same results even in a multicenter study.
Summary of radiological evaluation.
Adverse reactions.
Several studies on chemotherapy regimens other than CDDP+5FU for curative chemoradiotherapy of unresectable esophageal cancer have been reported. Hejna et al. (13) treated 30 patients with unresectable esophageal cancer with CDDP+etoposide+radiation (RT), and reported that the response rate was 40% (CR: 10%; PR: 30%). Regarding adverse effects of grade 3 or higher, neutropenia was noted in 57%, leukopenia in 43%, thrombocytopenia in 37%, anemia in 17%, and esophagitis, hair loss, and infection in 10%; and regarding outcomes, the median survival time was 9.2 months, and the 1-year survival rate was 3.3%. Iwase et al. (14) treated 31 and 24 patients with stage III and IV advanced esophageal cancer, respectively, with uracil+tegafur+CDDP+RT and the response rate was 71% (CR: 20%; PR: 51%), grade 3 or severer adverse effects were leukopenia in 78%, thrombocytopenia in 20%, anemia in 9%, and nausea in 9%. Regarding the outcome, the 2-year and 5-year survival rates of stage III patients were 25% and 4%, respectively, and those of stage VI patients were 7% and 0%, respectively. In addition, Kato et al. (15) treated 25 patients with unresectable esophageal cancer with nedaplatin+5-FU+RT in, and the response rate was 77%; grade 3 or severer adverse effects were leukopenia noted in 20.5%, thrombocytopenia in 15.4%, and anemia in 7.7%, and the 1-year and 2-year survival rates were 30.7% and 10.2%, respectively. Cho et al. (16) treated 30 patients with unresectable esophageal cancer with tegafur/gimeracil/oteracil (S-1)+CDDP+RT, and the response rate was 74.1% (CR=18.5%, PR=55.6%), grade 3 or severer adverse effects were leukopenia in 19% and neutropenia in 15%, the median survival time was 11.6 months, and the 1-year and 3-year survival rates were 40.9% and 0%, respectively. Chemoradiotherapy using these various regimens has been reported, but none of the regimens resulted in satisfactory treatment outcomes. Thus, improvement in treatment outcomes is anticipated via the development of a new regimens of chemoradiotherapy for unresectable advanced esophageal cancer.
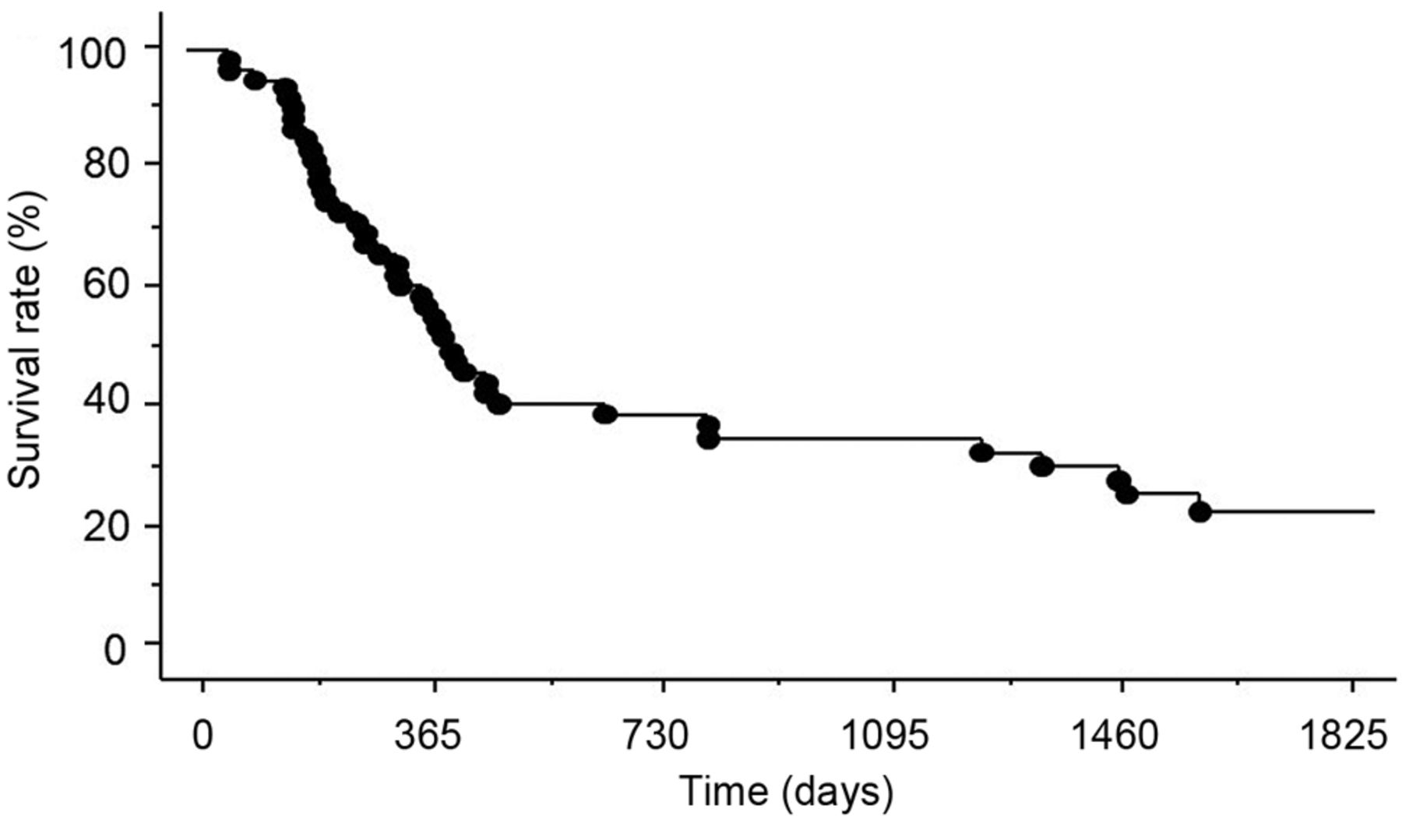
Actual survival curve of DCF-R therapy. The median survival time was 406 days. The 1-year, 2-year and 5-year survival rates were 58.6, 39.1, and 22.8%, respectively.
DTX has less cross resistance to chemotherapy using CDDP and 5-FU because it has a different action mechanism from those of previous anticancer drugs (17). Its antitumor effect is considered to be independent from p53, although esophageal cancers with the p53 gene mutation occur at a high frequency. Furthermore, an in vitro study reported that the antitumor effect of DTX on a human esophageal cancer cell line was stronger than that of paclitaxel, which is also a taxane anticancer drug (18). Focusing on these findings, we performed a phase II study of chemotherapy alone for highly advanced esophageal cancer from 2003, in which DTX was added to the conventional combination of CDDP and 5FU. Regarding the therapeutic effect, the response rates against lymph node and distant organ metastases exceeded those acquired by conventional CDDP+5FU chemotherapy. An excellent antitumor effect on the main lesion was also observed, but tumor regrowth occurred early in a considerable number of patients. Thus, aiming at acquiring a higher therapeutic effect, we planned chemoradiotherapy in which irradiation therapy with superior local tumor control was added to the triple-drug combination chemotherapy of DTX, CDDP, and 5FU and initiated a phase I study in 2007. No treatment-associated deaths occurred and the treatment completion rate was 100%, confirming favorable tolerability of this regimen. In addition, the response rate was 73% (CR=26.7%; PR=46.3%), showing that the therapeutic effect was favorable. The recommended doses determined in the phase II study were 60 mg/m2 DTX, 60 mg/m2 CDDP, and 600 mg/m2 5FU. Based on these findings, we initiated the present phase II study in January 2009 and investigated the safety and efficacy of this new regimen.
Few studies on chemoradiotherapy for unresectable esophageal cancer using a regimen similar to ours have been reported. Okamoto et al. (19) performed DCF-R for cervical esophageal cancer and reported that the response rate was 91.0%, grade 3 or severer adverse effects were leukopenia in 91%, neutropenia in 91%, sore throat in 55%, and febrile neutropenia in 45%, and the 2-year survival rate was 72%. Higuchi et al. (20) administered DCF-R in T4 patients and M1Lym patients and reported that the response rate was 52.4%, grade 3 or severer adverse effects were leukopenia in 71.4%, neutropenia in 57.2%, febrile neutropenia in 38.1%, anemia in 16.7%, loss of appetite in 31.0%, and esophagitis in 28.6%, and the 1-year and 3-year survival rates were 66.1 and 43.9%, respectively. They investigated the dose of irradiation exposure at the same time and reported that the incidence of loss of appetite and esophagitis tended to be decreased by reducing the total dose from 61.2 to 50.4 Gy, and no pericarditis or esophageal fistula developed as late complications. Therefore, favorable outcomes of DCF-R compared with the outcomes of chemoradiotherapy using other regimens have been reported. In our phase II study, the response rates of the main lesion, metastasized lymph nodes, and distant organ metastases were 85.2%, 80.7%, and 67.6%, respectively, which were favorable. The adverse effects were leukopenia noted in 98.4%, anemia in 62.3%, and nausea in 60.7%, showing that the incidence of leukopenia was high. However, the treatment completion rate was 90.2% and no treatment-associated deaths occurred. The median survival time was 406 days and the 1-year and 5-year survival rates were 58.6% and 22.8%, respectively, showing that the outcome was favorable. Of the 15 patients who clinically achieved a CR, 8 patients survived for 5 years or longer or were still alive. In 3 patients, the lesion became resectable after DCF-R treatment and surgery was performed. Two of the patients achieved a long-term survival of 5 years or longer, showing that complete cure of unresectable advanced esophageal cancer is possible.
Our results demonstrated that chemoradiotherapy with DTX, CDDP, and 5FU can be safely administered and the therapeutic effect is favorable. Although patient accumulation and long-term observation are necessary in the future, this regimen may be promising for patients with unresectable esophageal cancer.
Acknowledgements
The Authors are indebted to Instructor Helena Popiel of the Department of International Medical Communications of Tokyo Medical University for the review of this manuscript.
Footnotes
Authors' Contributions
K. Takahashi wrote the manuscript. Y. Osaka conceived the idea and study design and edited the manuscript. Y. Ota, T. Watanabe, K. Iwasaki, and S. Tachibana provided medical care to the patient during his hospital stay. Y. Nagakawa, K Katsumata, A Tsuchida read and approved the final manuscript. All Authors provided critical feedback and contributed to the research and analysis, and proofread the final manuscript.
Conflicts of Interest
The Authors declare no conflicts of interest associated with this manuscript.
- Received February 16, 2020.
- Revision received March 27, 2020.
- Accepted April 3, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Concurrent Chemoradiotherapy With Docetaxel, Cisplatin, and 5-Fluorouracil (DCF-RT) for Patients With Potentially Resectable Esophageal Cancer
- Sleep Problems Prior to Radio-chemotherapy in Patients With Locally Advanced Cancer of the Esophagus or the Esophagogastric Junction
- Concurrent Chemoradiotherapy With Docetaxel, Cisplatin, and 5-Fluorouracil (DCF-RT) vs. Cisplatin and 5-Fluorouracil (CF-RT) for Patients With Unresectable Locally Advanced Esophageal Cancer in a Real-world Clinical Setting