


Abstract
Aim: To explore whether the size and characteristics of the largest regional lymph node in patients with rectal cancer, based on magnetic resonance imaging (MRI), following neoadjuvant therapy and before surgery, is able to identify patients at high risk of developing metachronous metastases. Patients and Methods: A retrospective case–control study with data from the Swedish Colo-Rectal Cancer Registry. Forty patients were identified with metachronous metastases (M+), and 40 patients without metastases (M0) were matched as controls. Results: Patients with M+ disease were more likely to have a regional lymph node measuring ≥5 mm than patients with M0. (87% vs. 65%, p=0.02). There was also a significant difference between the groups regarding the presence of an irregular border of the largest lymph node (68% vs. 40%, p=0.01). Conclusion: Lymph nodes measuring ≥5 mm with/without displaying irregular borders at MRI performed after neoadjuvant therapy emerged as risk factors for metachronous metastases in patients with rectal cancer. Intensified follow-up programmes may be indicated in these patients.
Rectal cancer is a global health problem, each year affecting 700,000 new individuals worldwide (1). In Sweden, a total of 2,000 patients are diagnosed with rectal cancer annually; morbidity and mortality remain high, with a 5-year relative survival of 66% (2).
Approximately 20-30% of all patients with rectal cancer will, at some point, be diagnosed with metastases (3-5) in the liver, lungs or elsewhere. Fifty percent of these are diagnosed as synchronous metastases, i.e. simultaneous with the diagnosis of the primary rectal tumour (6). In the other half, metastases are metachronous; the metastases develop later, i.e. during follow-up of the primary treatment. Despite improved therapeutic options with combination chemotherapy, stereotactic radiotherapy, surgical resections and locally ablative approaches, a significant proportion of these patients will die due to their disease. In Sweden, the relative 5-year survival in patients with stage IV rectal cancer (i.e. metastatic disease) is 20% (6). According to the Swedish Registry of Liver, Bile duct and Gallbladder Cancer (Sweliv), relative 5-year survival in patients with colorectal liver metastasis undergoing resection or ablation is 51% (7). This indicates that active follow-up and prompt initiation of treatment upon detection of metastases is relevant and may lead to long-term remission or even cure. The risk of developing metastases is proportional to the primary cancer stage. In rectal cancer, this is most evident for liver metastases (5).
In order to identify patients with recurrent or metastatic disease as early as possible, there is a Swedish national standardised follow-up programme after rectal cancer surgery. Several attempts have been made to find evidence of improved survival with more intense follow-up programmes for colorectal cancer (8, 9). The COLOFOL trial (8) did not find a significant reduction of 5-year mortality when comparing high-frequency follow-up to low-frequency. A Cochrane review from 2016 concluded that more patients in a high-frequency follow-up were treated with surgery (with curative intent) (10). This might indicate that optimal follow-up programmes need to be more individualised than today. Preferably, such tailored follow-up strategies should use simple and easily available tools for prognostic risk scoring. The vast majority of patients with rectal cancer will undergo MRI for tumour staging and evaluation of neoadjuvant therapy, and a natural starting point would therefore be the identification of early MRI radiological warning signs that indicate a higher risk of metachronous metastasis and that a more intense follow-up might be required.
The importance of MRI in staging rectal cancer is widely recognised, as is the use of MRI for assessment of tumour response after neoadjuvant treatment. Neoadjuvant treatment in rectal cancer consists of radiation therapy (RT) with or without chemotherapy (11). In lymph node staging (N-stage), size, signal intensity and border contours are different criteria for indicating positivity (12-15). Current European guidelines for restaging, updated in 2018, consider all nodes <5 mm to be benign, and ≥5 mm to be malignant (15).
Due to the effect of RT on lymph nodes, nodal status following neoadjuvant therapy is difficult to interpret (16). Since RT eradicates both benign and malignant lymph nodes (17), there are fewer nodes to evaluate post RT. Size does more accurately predict positive lymph nodes after RT compared to before it (18, 19). This might possibly make interpretation easier for a non-expert radiologist to evaluate the lymph node status after RT. The size of the largest lymph node might be a criterion for use in a clinical setting.
In a previous study by our group, we reported that the average size of the largest lymph node on evaluating MRI was significantly larger in the group with nodal metastases (N+) than in that without (N0) (20). Other studies have made node-per-node-analyses in order to find lymph nodes with metastasis (12, 21).
To explore the importance and reliability of a standardised lymph node predictive model based on the preoperative MRI, a retrospective case–control study was designed. Patients with rectal cancer and evidence of metachronous metastasis during follow-up were compared with matched controls who had similar baseline characteristics but who did not develop metachronous metastases. The main hypothesis was that if the largest lymph node after neoadjuvant treatment was ≥5 mm, or had other morphological characteristics signifying involvement of cancer, it would indicate a higher risk for development of metachronous metastasis.
Patients and Methods
According to Swedish national guidelines (22), all patients with rectal cancer should be assessed at multidisciplinary team conferences (MDT). An MRI is performed before the MDT in order to stage the rectal tumour. The most advanced rectal tumours are treated with preoperative RT or chemo-radiotherapy (CRT). Short-course RT, 5×5 Gy, is directly followed by surgery or with a 6-14-week delay before surgery. Long-course RT, 2×25 or 1.8×28 Gy, is also followed by a waiting period before surgery, to allow for RT-induced down-staging of primary tumour and regional lymph nodes. Short-course RT with delay gives biological effect and oncological results equal to those of long-course RT with delay (23, 24), and can be regarded as comparable therapies. When RT is followed by a delay, it is common practice to perform an MRI after 6 weeks, ahead of surgery, in order to rule out progression. Thus, two MRI examinations are performed before surgery.
Baseline characteristics of patients with rectal cancer with (M+) or without (M0) metachronous metastasis. Clinical lymph node stage (cN) was analysed using Fisher's exact test.
Radiotherapy (RT), and neoadjuvant and adjuvant treatment.
The inclusion criteria for this study were patients with rectal cancer, without synchronous metastases (cM0), who had undergone elective radical surgery (R0) during 2008-2015, in the south east region of Sweden covering three centres (Jönköping, Kalmar and Östergötland) and a total population of 1.1 million (2019) (25). All participants were evaluated with preoperative MRI, received neoadjuvant (C)RT with radical surgery delayed more than 6 weeks, and subsequently developed one or more metachronous metastases.
Metachronous metastases were defined as one or more metastases found after rectal surgery in patients who were staged as M0 at MDT. Metastases were defined as metastases in the liver, lungs or another organ. The medical records were reviewed after a minimum follow-up period of 2 years from surgery. Some patients had died by the time medical records were reviewed; these patients were also included in the study.
In order to compare this group of metastasis-afflicted patients, an equally large number of metastasis-free patients meeting the inclusion criteria were identified and included. This control group was matched to the study group by gender, county of residence, year of surgery, age at diagnosis, type of RT, neoadjuvant chemotherapy, T-stage and adjuvant chemotherapy (Tables I and II). Node-per-node analyses were not made, since the objective was to study MRI in a clinical setting.

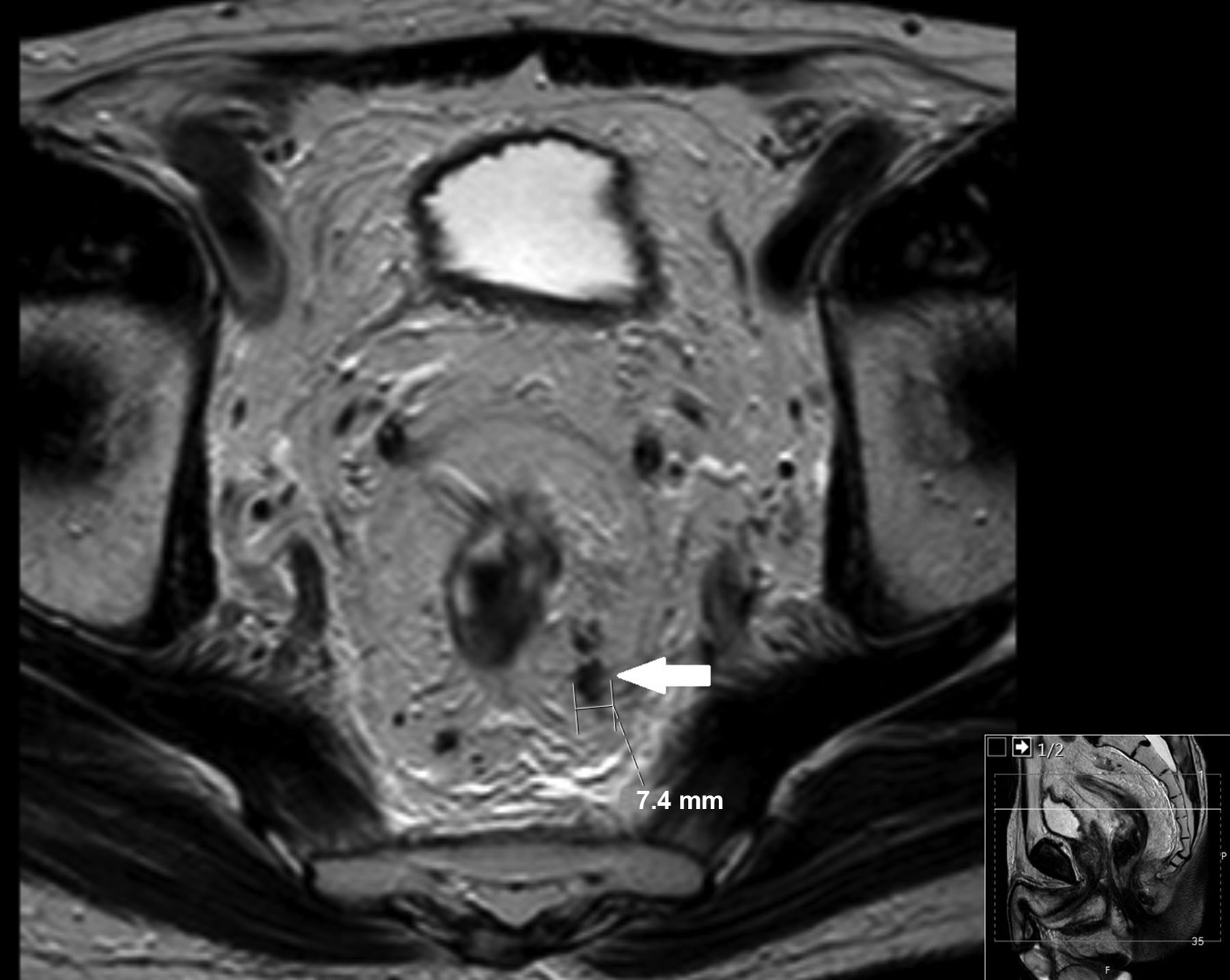
Magnetic resonance imaging showing the irregular border of the largest lymph node.
Patients. The patients were identified from the Swedish Colo-Rectal Cancer Registry (SCRCR). Sweden is unique in that all Swedish citizens since 1947 have a personal identity number (26). Since 1995, all patients with rectal cancer have been recorded in the SCRCR (27).
To ensure that no metastases were missed in the SCRCR, data from Sweliv and the Swedish Registry of Thoracic Surgery (ThoR) were also collected. These patients were compared to SCRCR and if uncertainties were detected, these were resolved by a manual review of the primary medical record. No additional patients were found in these two registries. All data collection was made in 2017 and 2018, and the medical records were examined in May 2018.
MRI interpretation and analyses. The MR images were collected from different Radiology Departments. The MR images were assessed by one radiologist (M.W.) with 5 years of experience in reading pelvic MRI and was aware of the inclusion criteria but blinded to the information on metastasis, as well as the surgical and pathological findings. The interpreter had no access to the primary report of the MRI examinations. Analysis was performed using a Sectra Workstation IDS7 with diagnostic monitors.
The field strength of all examinations was 1.5 Tesla. The examination protocol varied as the examinations were carried out at different locations. The assessment was performed on axial, sagittal and oblique T2-weighted sequences in at least two planes as well as T1-weighted images. Eighty-seven percent of the examinations included a thin-slice sequence with 3 mm slice thickness. Thirteen percent of the examinations had a slice thickness of 5 mm. The T1-weighted images were mainly used for the assessment of lymph nodes. Diffusion-weighted images were not assessed as these were not available for all patients.
The following parameters were evaluated (28) for this study: Tumour stage (T- stage), number of lymph nodes (total number of lymph nodes, both potentially benign and malignant were recorded), short axis diameter of the largest lymph node (mm), borders of the largest lymph node (regular/irregular), and signal characteristics of the largest lymph node (regular/irregular) (Figure 1).
Statistical analysis. Baseline characteristics are presented as the median and range when not otherwise stated, using independent median sample test; when presented as the mean, the standard deviation is also presented. Parametric data were analysed using Student's t-test and non-parametric data were analysed using Pearson's chi-squared test. A p-value of less than 0.05 was considered significant. The analyses were made using SPSS©, version 25 (IBM, Armonk, NY, USA).
Ethics. This study was approved by the Regional Ethics Committee at Linköping University (Dnr 2017/425-31) and conducted according to national/European regulations and the Helsinki declaration. Informed consent was not necessary given the retrospective non-interventional nature of the study.
Results
The initial cohort consisted of 703 patients who were identified in the SCRCR and diagnosed with rectal cancer between January 2008 and December 2015. Of these, a total of 138 (19.6%) patients were found to have been diagnosed with metachronous metastases, of whom 40 had been examined with a preoperative MRI. The number of individuals eligible for inclusion in the study was therefore 40 patients, and thus 40 patients were also allocated to the control group (Table I).
The sparse use of MRI was partly due to the fact that a majority of these patients had received short-course RT without delay to surgery (which does not justify a second MRI preoperatively), and partly because some centres had yet to implement the MRI procedure as standard practice in their clinical settings at the time of data entry.
The median follow-up time between primary surgery and medical record review was 53 (range=29-117) months. The attrition rate was 45%, due to death of included patients.
Demographics. The median number of positive lymph nodes was significantly higher in patients with metachronous metastases compared to those without [2 (range=0-19) vs. 0 (range=0-7), p<0.001]. There was no significant difference between the groups regarding classification of mucinous tumours at histopathological assessment (six in the M+ group and eight in the M0 group, p=0.73). Distant metastatic sites were identified as the liver in 14, lungs in 20 and other (e.g. peritoneum and brain) in 11.
Median survival from primary surgery to death/date of medical record review was 28 (range=2-98) months in the M+ group and 53 (range=3-117) months in the M0 group (p<0.0001).
The median metastasis-free interval (from date of surgery to detection of metachronous metastasis) was 8 (range=1-31) months. Fourteen (35%) patients with metachronous metastases were treated with surgery (with curative intent), the remainder were treated with best supportive care, with or without palliative oncological therapies. Median survival from diagnosis of metastasis was 17 (range=1-61) months.
Magnetic resonance imaging interpretation after neaoadjuvant radiotherapy. Clinical stage of tumour after neoadjuvant treatment (yT) was analysed using Fisher's exact test.
MRI interpretation: Size of the largest lymph node. There were no significant differences between the M+ and M0 groups regarding the size of the largest lymph node (median 6 mm and 5 mm, respectively, p=0.35) or T-stage on evaluation of the MRI after neoadjuvant radiotherapy (Tables III and IV). However, there was a significant difference between the two groups regarding the number of patients with the largest lymph node ≥5 mm (n=34, 87% vs. n=26, 65%, p=0.02).
Lymph nodes larger than 8 mm were found only in patients with positive nodes on the histopathological assessment (n=13).
Morphology of the largest lymph node. Irregular borders of the largest lymph node were significantly more frequent in the M+ group [27 (68%)] compared with the M0 group [16 (40%) (p=0.01) (Table IV).
Morphology of the largest lymph node compared to histopathological assessment. When comparing the histopathological lymph node assessment (ypN) with the MRI-assessment (ycN), there was a significant difference in the presence of irregular borders on MRI: With 25/38 (66%) in the ypN+ group and 18/42 (43%) in the ypN0 group (p=0.04). The frequency of heterogeneous signal was also significantly higher in the ypN+ group at 27/38 (71%) than in the ypN0 group [19/42 (45%)] (p=0.02).
Discussion
This study was conducted to explore the prognostic impact of lymph node characteristics on the preoperative MRI evaluation in patients with rectal cancer who had received neoadjuvant RT. Nodal status post neoadjuvant treatment was based on interpretation of the size, border characteristics and signal intensity of the largest lymph node. Our main finding was a positive association between the size of the largest lymph node (≥5 mm as measured on preoperative MRI) and the risk of developing metachronous metastases (p=0.02). Similarly, irregular border features of the largest lymph node were more common in the metastases group in this patient cohort (p=0.01). These results suggest the need for further studies focusing on standardised evaluation of the largest lymph node on the preoperative MRI as a tool for risk stratification and personalised follow-up schedules.
Characteristics of the largest lymph node (LLN) after neoadjuvant radiotherapy.
In a previous study by our group, the size of the largest lymph node after neoadjuvant treatment was found to indicate nodal positivity (20). In that study, lymph nodes of 8 mm or more in diameter were similarly correlated with ypN+. This confirmed, in accordance with other studies, that size is a key factor when interpreting MRI post RT in patients with rectal cancer (15, 18, 19).
As several studies have indicated, the MRI characteristics of lymph nodes in rectal cancer is also important for predicting nodal involvement (12, 13). This study supports these findings, since there were significant differences when comparing nodal status on histopathological assessment with characteristics of the largest lymph node on MRI.
Although the evidence is conflicting (8-10), the rationale for follow-up programmes is that early (rather than late) detection of metachronous metastases will lead to better treatment options due to less extensive disease, and therefore an enhanced likelihood for successful treatments and improved survival. As only a small proportion of patients will develop metachronous metastases, identifying risk factors would be of great value in order to find high-risk patients, and develop individualised follow-up programmes for them. In addition, other patients with very low risk of metastatic disease could be excluded from intense follow-up; economical costs as well as patient inconvenience and psychological stress associated with the follow-up schedule would therefore also be avoided. There are still questions regarding the optimal follow-up regime (8, 9), as several large multi-centre studies did not show any survival benefits between different follow-up-regimes (8-10). Case mix may hide any benefit of more intense follow-up in a sub-group of patients.
Apart from standardised and correct staging of the primary tumour, which has been recognised as a key prognostic parameter (4), the present results suggest that the size and characteristics of the largest lymph node on post neoadjuvant MRI might be a predictor for subsequent development of metachronous metastases, and a potential tool for future decisions regarding individualised follow-up.
The present study has some limitations. While the original cohort of patients was large at 703, of which 138 were diagnosed with metachronous metastases during follow-up, a large proportion of these, 98 in fact, could not be included in the study. The reason for this is partly because the majority of the patients were treated with short-course RT without delay to surgery but also due to the absence of a preoperative MRI. The most likely explanation for absence of MRI after RT with delay was the delayed implementation of MRI in the post neoadjuvant/preoperative setting at many centres, a procedure that is now considered a standard of care (22). In effect, there were only 40 cases available for analysis, and groupwise or further multivariable statistics were not feasible. The matched case–control design, with minimal variation in other known prognostic parameters obscuring the factors of interest, was therefore considered the most sensible way to address the main hypothesis. There was a high attrition rate in median follow-up, due to high rate of death, these were thus censored. They were, however, included in the study. Due to the limitations mentioned, the results obtained should be interpreted with care. Nevertheless, the present findings encourage larger retrospective and prospective observational studies where the prognostic impact of standardised post neoadjuvant/preoperative MRI is further evaluated. The main strength of the present study was the population-based real-world approach and, given the Swedish public healthcare system that offers equal treatment and follow-up programmes to all citizens, this minimises the risk for bias based on socioeconomic factors and varying accessibility to healthcare providers.
In conclusion, this study indicates that both irregular lymph node border and largest lymph node size ≥5 mm, as measured on MRI post neoadjuvant treatment and before surgical resection, may be predictors for metachronous metastatic disease in rectal cancer. Further studies are needed to elucidate whether intensified follow-up programmes are beneficial or not in this group of patients.
Footnotes
Authors' Contributions
All Authors of this research article directly participated in the planning, execution, or analysis of this study. All Authors read and approved the final version submitted.
This article is freely accessible online.
Conflicts of Interest
None of the Authors have any conflicts of interest to report.
- Received March 8, 2020.
- Revision received April 9, 2020.
- Accepted April 13, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}