


Abstract
Background/Aim: To develop a nomogram for predicting the pathological tumor response to preoperative chemoradiotherapy (CRT) for locally advanced rectal cancer based on pre-treatment magnetic resonance imaging (MRI) and blood test characteristics. Patients and Methods: This retrospective study included 514 patients who underwent MRI and received preoperative CRT followed by surgical resection. Pathological tumor response was assessed as good [Dworak tumor regression grade (TRG) 3 or 4] or poor (TRG 0-2). A nomogram for good response was developed using stepwise logistic regression analysis. Results: A nomogram based on longitudinal tumor diameter, extramural tumor invasion depth, carcinoembryonic antigen and hemoglobin levels, age, and interval between CRT and surgery gave an area under the receiver operating characteristic curve for a good response of 0.721 (95%CI=0.676-0.768). Conclusion: Our nomogram based on pre-treatment clinical characteristics can predict the tumor response to CRT, which may help identify patients who can benefit most from CRT.
The current standard treatment for locally advanced rectal cancer is preoperative chemoradiotherapy (CRT) followed by surgical resection. The tumor response to CRT varies considerably among patients. Those with a good response to CRT can be expected to experience good oncological outcomes (1-3) and may demonstrate the potential for organ-preserving approaches such as local excision or watch-and-wait, thereby avoiding the risk of surgical complications and the need for a stoma (4). Conversely, a considerable number of patients do not show significant regression of the tumor with CRT. Although preoperative CRT has been shown to allow sphincter preservation and reduce the risk of local recurrence and cancer-specific mortality (5-7), it is associated with an increase in mortality from other causes, such as vascular or infectious (6), and no benefit to overall survival exists (7). Furthermore, radiotherapy in the pelvic region is associated with a higher prevalence of sexual dysfunction (8), fecal incontinence, and urinary incontinence (9-11).
Therefore, the ability to predict accurately the pathological tumor response to CRT would be beneficial. This would allow potential non-responders to be exempted from unnecessary exposure to ineffective yet harmful CRT. It would also allow physicians to make better informed and more prudent decisions about organ-preserving approaches for the patients expected to respond well after CRT. Despite extensive research, identifying a reliable predictive marker because of the complex mechanisms involved in the resistance to CRT remains difficult (12, 13). Molecular biomarkers may demonstrate the potential to provide an early prediction of the response to CRT, but none are currently available for clinical use. Pre-treatment clinical characteristics could potentially form the basis for a cost-effective prediction model for tumor response to CRT with wide applicability. However, studies investigating this approach reported that clinical characteristics were not good predictors of tumor response as expected (14, 15).
To address these issues, the aim of this study was to develop a nomogram for predicting the patient-specific probability of a good response to CRT. The nomogram integrates pre-treatment clinical characteristics, such as MRI findings and blood test results.
Patients and Methods
Patients. The Institutional Review Board of Seoul National University Bundang Hospital approved this study (IRB no. B-1906-546-101). The requirement for informed consent was waived because of the retrospective nature of the study. This study retrospectively analyzed data from 514 patients with pathologically confirmed primary middle or low rectal cancer (stage II and III), who received preoperative CRT followed by curative intent surgical resection at our hospital between January 2004 and May 2019.
Treatments. All but 20 of the patients were treated with radiotherapy (three-dimensional, n=398; two-dimensional, n=96) at a dose of 45 Gy to the whole pelvis, followed by a primary tumor boost of 5.4 Gy within 5.5 weeks. The other patients (n=20) were treated with simultaneous integrated boost intensity-modulated radiation therapy (SIB-IMRT) at a dose in the range of 50-54.6 Gy in 25 or 26 fractions. All but six of the patients were treated with fluoropyrimidine-based chemotherapy, either as an intravenous bolus of 5-fluorouracil/leucovorin (400/20 mg/m2 daily injection for three days in weeks 1 and 5) or as capecitabine (825 mg/m2 twice daily throughout the radiation period). The other six patients received a combination regimen, including cetuximab, irinotecan, and capecitabine. After completing the CRT, 15 patients received a local transanal excision, and the other patients received total mesorectal excision.
Pathological examination. Dedicated gastrointestinal pathologists graded the surgical specimens using Dworak's tumor regression grading (TRG) system, as follows (3): TRG 0, no regression; TRG 1, dominant tumor cell mass with obvious fibrosis; TRG 2, dominant fibrotic changes with few tumor cells or groups; TRG 3, very few (difficult to find microscopically) tumor cells in fibrotic tissue, with or without mucous substance; and TRG 4, no tumor cells, only fibrotic mass. The patients were categorized according to the response to CRT as having either a good response (TRG 3 or 4) or a poor response (TRG 0, 1, or 2).
Statistical analysis. Univariate analyses using Student's t-test or the chi-square test were used to identify clinical variables associated with the tumor response to CRT. A receiver operating characteristic curve (ROC) analysis was performed for each of the continuous variables predicting tumor response to determine the cut-off point indicative of a good response (16). The multivariate analysis used a logistic regression model, applying backward stepwise selection by using the likelihood ratio test. Regression coefficients were applied to develop the nomogram, and the area under the ROC curve (AUC) for the nomogram was used to quantify its predictive accuracy (17). The statistical analyses were performed using R software (version 3.5.3; R Foundation for Statistical Computing, Vienna, Austria).
Patient characteristics.
Univariate and multivariate analysis for pathologic good response.
Results
The baseline characteristics of the 514 patients are summarized in Table I. The median age was 61 years (range=28.2-88 years), and the median tumor distance from the anal verge was 5 cm (range=0-10 cm). At the initial evaluation, most of the tumors were stage III (88.7%) and moderately differentiated (79.0%).
Of the 514 patients, 184 (35.8%) showed a good response and 330 (64.2%) a poor response. There were no significant differences between the good and poor response groups in age, sex, distance from the anal verge to the lower pole of the tumor, histological differentiation on biopsy, or clinical TNM stage. Factors associated with a good response to preoperative CRT included low clinical T and N stages, small diameters of the primary tumor and metastatic lymph nodes, a shallow extramural tumor depth in the pre-treatment MR images, low pre-treatment levels of hemoglobin (Hb) and carcinoembryonic antigen (CEA), and a long interval (≥ 6 weeks) between radiotherapy and surgery. The good response group was more likely to have undergone transanal excision and less likely to have undergone abdominoperineal resection.
Table II summarizes the results of the univariate and multivariate logistic regression analyses. After stepwise selection, the following variables were included as predictors of a good response, with cut-off values established from the ROC analyses: longitudinal tumor diameter [odds ratio (OR)=0.79; p=0.016], shallow extramural tumor depth (≤ 3 mm; OR=1.81; p=0.006), age >45 years (OR=2.85; p=0.015), high pre-treatment level of Hb (≥15 g/dl; OR=1.98; p=0.006), long interval between CRT and surgery (≥ 6 weeks; OR=2.65; p=0.043), and low pre-treatment level of CEA (1 ng/ml < CEA ≤3 ng/ml; OR=1.83; p=0.015; CEA ≤ 1 ng/ml; OR=4.02; p<0.001). The nomogram developed from this model is shown in Figure 1. A ROC analysis of the model's ability to predict a good response resulted in an AUC of 0.721 (95% confidence interval=0.676-0.768) (Figure 2A). Internal validation of the nomogram was performed using 200 bootstrap resamples, demonstrating satisfactory predictive ability (Figure 2B).
Discussion
This single-institution retrospective study evaluated clinical variables as predictors of a good tumor response after preoperative CRT for locally advanced rectal cancer. Pre-treatment CEA and Hb levels, longitudinal tumor diameter, extramural tumor depth, age, and the CRT-to-surgery interval were independent predictors of a good response. We used these predictors to develop a nomogram, which demonstrated an AUC of 0.721 for the prediction of a good pathological response to CRT. To the best of our knowledge, there has been no study predicting tumor response based on pathologic complete response (pCR) and near-complete response (nearCR) patients. The prognostic significance of nearCR is inconsistent across studies (18-21). In particular, researchers reported that patients with rectal cancer with nearCR and a pathological lymph node status (ypN+) experienced poor outcomes (21), whereas other studies suggested that patients with nearCR experience favorable oncological outcomes comparable to those with pCR (3, 22-26). For this reason, we did not differentiate between pCR and nearCR in the present study.

Nomogram for predicting the probability of pathologic good response.
Numerous studies investigated the association between clinical variables and pathological tumor response in locally advanced rectal cancer. Factors reported to be associated with the increased likelihood of pCR included low CEA (pre/post CRT) (14, 27-29), small tumor size (pre/post CRT) (30, 31), low T/N stage (32), tumor movability (30), low histologic grade (32), small circumferential tumor extent (15), high Hb levels (14), and a low neutrophil-to-lymphocyte ratio (33). In the present study, low pre-treatment CEA, high pre-treatment Hb, small tumor size (based on the longitudinal tumor diameter), shallow extramural tumor depth, and age >45 years were independent predictors of a good response. All these factors apart from age have previously been identified as predictors of pCR. Intriguingly, patients younger than 45 years were associated with a lower probability of a good response in the present study. As far as we know, no previous report addressed the association between age and pathological response, although Jwa et al. reported that young age was a predictor for post-CRT lymph node metastasis (34). Our finding might be explained by younger patients exhibiting poorer tumor biology, but the possibility of selection bias cannot be ruled out, and further study is needed to confirm this finding.
Several treatment-related factors associated with the pathological response to CRT are modifiable. The optimal timing for surgery after CRT has been investigated in several studies (35, 36); however, the only prospective randomized trial to address this is the Lyon R90-01 study (37), which reported a higher pCR rate with a long interval between CRT and surgery (6-8 weeks) compared to a short interval (2 weeks). Although the ideal interval between CRT and surgery has not yet been established, the findings of the previous studies, including a meta-analysis, suggest that increasing the treatment interval to more than 8 weeks may improve pCR rates (35, 38). In the present study, a CRT-to-surgery interval of more than 6 weeks was associated with a better pathological response (pCR or nearCR), but no significant difference existed if this was increased to more than 8 weeks. This discrepancy with previous studies might be due to differences in the study subjects; unlike the previous studies, our analysis included patients with both pCR and nearCR, not pCR alone. We interpret the difference with the previous studies as follows: the patients who achieve nearCR within 6-8 weeks may reach pCR after 8 weeks, whereas the patients who do not show nearCR within 6-8 weeks are unlikely to achieve a good response even if surgery is deferred by more than 8 weeks.
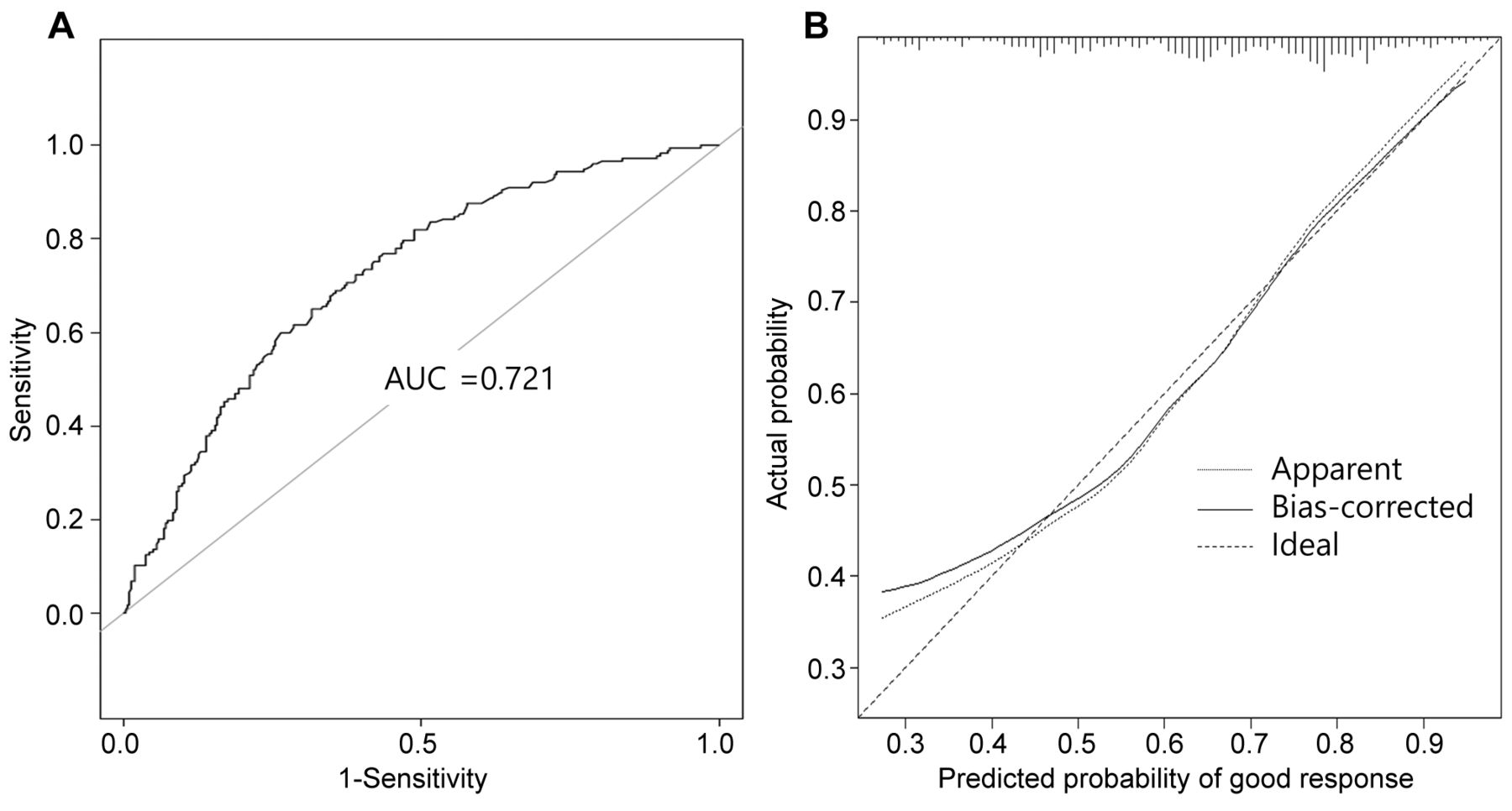
Analysis of the model's discrimination and calibration. (A) Receiver operating characteristic curve for pathologic good response model. (B) Calibration plot for pathologic good response nomogram.
A few studies investigated treatment intensification to allow more patients to achieve a pCR with acceptable toxicity (39-41). Burbach et al. reported in their meta-analysis that dose escalation above 60 Gy resulted in high pCR rates with acceptable early toxicity (42). The German CAO/ARO/AIO-04 randomized trial reported that adding oxaliplatin to fluorouracil-based CRT was well tolerated and increased pCR rates (43, 44). In our study, more than 95% of the patients received standard CRT; therefore, we were unable to investigate the association between pathological response and treatment strategy, such as radiation dose or type of chemotherapy.
In this study, we developed a nomogram to predict a good pathological response after CRT for patients with locally advanced rectal cancer. However, the nomogram requires further validation with an external cohort, and this study exhibited several limitations. First, there were the inherent limitations of a retrospective study, including the inevitable selection bias. Second, the prediction model predicts a good pathological response but not the lymph node status or long-term clinical outcomes. The TRG system does not provide information regarding nodal status, so our model should be interpreted and applied with caution. Nevertheless, our model demonstrates the potential to assist with patient selection, consultations, and the choice of treatment strategy for patients with locally advanced rectal cancer.
Acknowledgements
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (Grant number: NRF-2017R1D1A1B03033892).
Footnotes
↵* These Authors contributed equally to this work.
Authors' Contributions
JSK contributed to conception and design of the study. BHK, CS, and JSK contributed to analysis and interpretation of data, and drafting of the manuscript. All Authors participated in clinical data acquisition. All Authors read and approved the final manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors declare that they have no competing interests regarding this study.
- Received February 29, 2020.
- Revision received March 11, 2020.
- Accepted March 12, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}