


Abstract
Background/Aim: Patients requiring re-irradiation for recurrent glioblastoma multiforme (GBM) may benefit from individualized therapy. This study aimed to identify predictors of survival and contribute to treatment personalization. Patients and Methods: In 28 patients with recurrent GBM, nine factors were analyzed for associations with survival: Main location and type of recurrence, Karnofsky performance score (KPS), age, gender, interval between primary radiotherapy and recurrence, gross total resection (GTR), equivalent dose in 2-Gy fractions (EQD2) of re-irradiation and cumulative EQD2 of primary and re-irradiation. Results: On univariate analyses, GTR (p=0.047), EQD2 ≥30 Gy (p=0.029) and cumulative EQD2 ≥90 Gy (p=0.023) were significantly associated with better survival; frontal location (p=0.119) and KPS 80-100% (p=0.067) showed trends. In multivariate analyses, frontal location (p=0.032) and cumulative EQD2 ≥90 Gy (p=0.038) were significant; KPS 80-100% (p=0.110) and EQD2 ≥30 Gy (p=0.083) showed trends. Conclusion: Predictors of survival after re-irradiation for recurrent GBM were identified that can help when designing personalized treatments. Use of irradiation with EQD2 ≥30 Gy appeared superior to lower doses.
Of all primary brain tumors in adults, glioblastoma multiforme (GBM) is the most common, with an incidence of approximately three patients per 100,000 inhabitants worldwide (1, 2). The prognoses of most patients with GBM are poor (3). In a randomized trial investigating a tri-modality treatment approach including maximum possible resection of the GBM followed by radio-chemotherapy over 6 weeks with concurrent temozolomide and additional cycles of temozolomide, median survival and 5-year survival were less than 15 months and less than 10%, respectively (4, 5). Moreover, the median time to progression of GBM was only 6.9 months (4). The majority of recurrences of GBM occur in previously irradiated areas of the brain (in-field recurrences) and many patients receive a second course of radiotherapy (re-irradiation) (2).
The prognoses of patients re-irradiated for recurrent GBM are often poor, and treatment is palliative. In a systematic review and meta-analysis, the 1-year survival rate was only 36% after re-irradiation (2). However, selected patients may benefit from more aggressive treatment programs including resection of the recurrent GBM and systemic treatment (6-11). Thus, patients with recurrent GBM would likely benefit from individualized treatment taking into account various factors associated with the patient’s survival prognosis in order to avoid too aggressive treatment for those with a very short expected survival and a too limited one for longer-term survivors. In general, patients with an estimated short survival time should receive a short and minimally burdensome treatment such as short-course radiotherapy (12), whereas patients with more favorable prognoses could be candidates for a more aggressive approach including reresection and administration of systemic therapies (6-11).
The present study aimed to identify predictors of survival in a cohort of patients receiving re-irradiation for recurrent GBM and contribute to treatment personalization for this particular group of patients. Moreover, it aimed to contribute to the definition of the optimal dose of re-irradiation
Patients and Methods
Twenty-six patients irradiated for recurrent GBM (re-irradiation) between 2005 and 2018 were included in this retrospective study, which was approved by the local Ethics Committee (University of Lübeck, reference number 15-355A). Total doses ranged between 15.0 and 60.0 Gy (median=30.0 Gy). Doses per fraction were 1.2-1.5 Gy (twice daily) or 1.8-7.0 Gy (once daily). Radiation techniques included volumetric-modulated arc therapy in 12, fractionated stereotactic radiotherapy in 10 and 3D-conformal radiotherapy in 6 patients. All patients received additional systemic treatment prior to, during and/or following re-irradiation with temozolomide alone in 16, temozolomide and procarbazine/lomustine (PC) or carmustine in six, temozolomide and bevacizumab in two, procarbazine/lomustine alone in two, bevacizumab alone in one and procarbazine/lomustine PC plus bevacizumab in one patient. Resection of recurrent GBM was performed in eight patients (28.6%); in six of these, gross total resection (GTR) was achieved.
Nine potential prognostic factors were analyzed with respect to survival. These factors were: i) Main site of the recurrent GBM (frontal vs. temporal vs. parietal and/or occipital vs. central), ii) type of recurrence (in-field only vs. out-field with/without in-field), iii) Karnofsky performance score (KPS) at the time of re-irradiation (50-70% vs. 80-100%, median=70%), iv) gender, v) age at reirradiation (≤60 vs. >60 years, median=60 years), vi) interval between end of primary radiotherapy of GBM and recurrence (≤12 vs. >12 months, median interval=12 months), vii) GTR of recurrent GBM (no vs. yes), viii) equivalent dose in 2-Gy fractions (EQD2) of re-irradiation (<30 Gy vs. ≥30 Gy), ix) and cumulative EQD2 of the primary radiotherapy and re-irradiation (<90 Gy vs. ≥90 Gy) (13, 14). Distributions of the factors are summarized in Table I.
Characteristics included in the analyses of survival after a second course of radiotherapy (RT) for recurrent glioblastoma (reirradiation).
Survival was calculated from the first day of re-irradiation. Univariate analyses were performed applying the Kaplan–Meier method and the Wilcoxon test. p-Values less than 0.05 were regarded as significant, and p-values <0.12 as indicating a trend. The significant factors were subsequently included in a multivariate analysis (Cox regression model).
Results
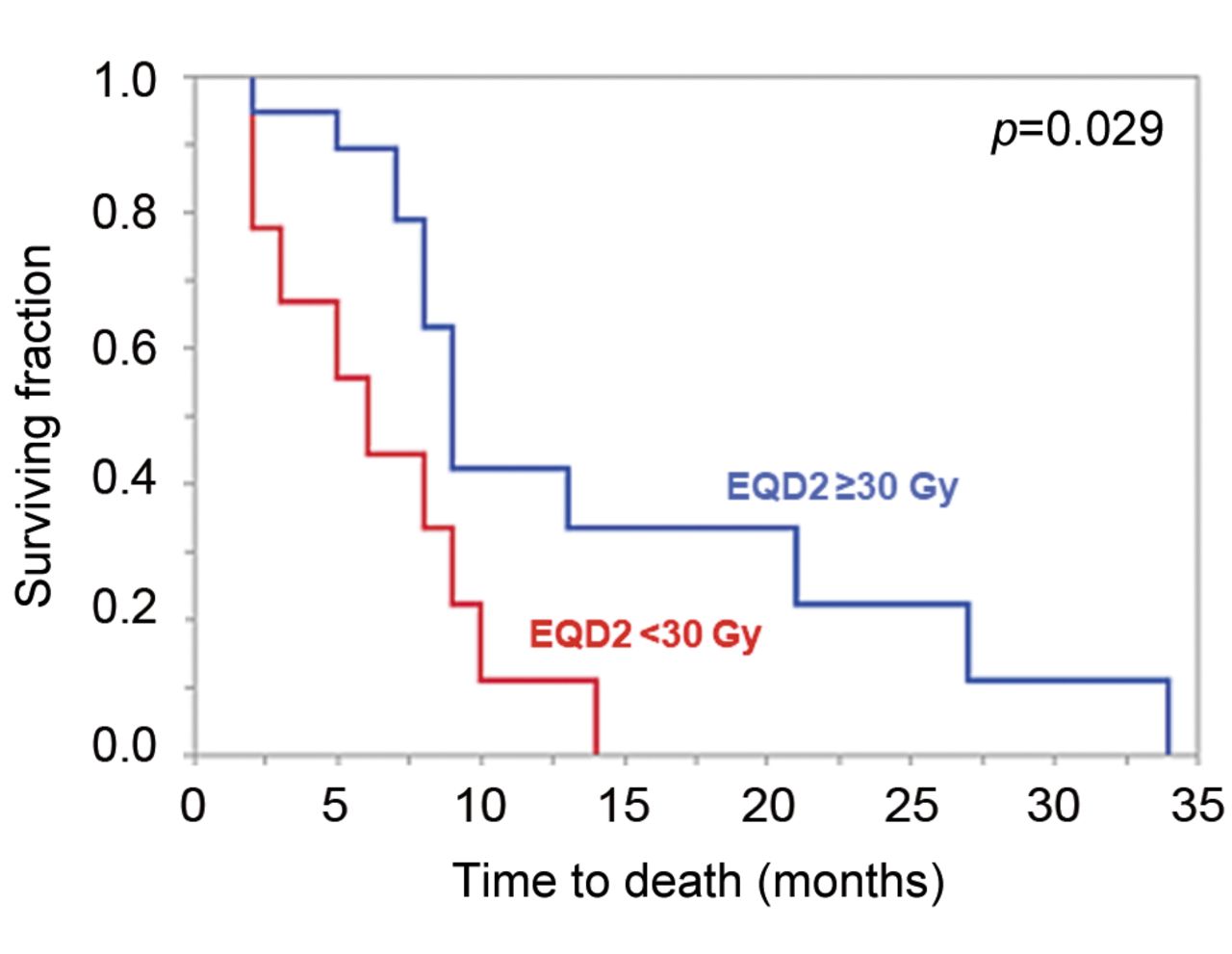
Median follow-up for the entire cohort was 9 months (range=2-34 months). Twenty-four patients (85.7%) died during the follow-up after median of 9 months. Median follow-up for the remaining four patients was 11 months (range=9-15 months). For the entire cohort, the survival rates at 6 months and 12 months were 75% and 32%, respectively. On univariate analyses (Table II), GTR (p=0.047), an EQD2 of re-irradiation ≥30 Gy (p=0.029, Figure 1) and a cumulative EQD2 of primary and re-irradiation ≥90 Gy (p=0.023, Figure 2) were significantly associated with more favorable survival. In addition, trends were found for frontal location of GBM (p=0.119) and a KPS of 80-100% (p=0.067).

Kaplan–Meier curves (univariate analysis) for the survival of patients receiving re-irradiation with an equivalent dose in 2-Gy fractions (EQD2) of ≥30 Gy vs. <30 Gy).

Kaplan–Meier curves (univariate analysis) for the survival of patients receiving a cumulative equivalent dose in 2-Gy fractions (EQD2) of primary radiotherapy and re-irradiation of ≥90 Gy vs. <90 Gy.
Survival rates (univariate analyses) at 6 and 12 months after start of radiotherapy (RT) for recurrent glioblastoma (re-irradiation).
In the subsequent multivariate analyses, frontal location [risk ratio (RR)=1.65, 95% confidence interval (CI)=1.04-2.68, p=0.032] and cumulative EQD2 ≥90 Gy (RR=2.57, 95% CI=1.05-6.49, p=0.038) were significantly associated with more favorable survival. KPS of 80-100% (RR=2.24, 95% CI=0.84-6.21, p=0.110) and EQD2 ≥30 Gy (RR=2.27, 95% CI=0.89-5.52, p=0.083) showed trends, and GTR (RR=2.17, 95% CI=0.66-9.71, p=0.21) was not significant.
Discussion
GBM is the most common primary brain tumor in adults and is often associated with a poor prognosis (1-3). Despite the introduction of multi-modality treatment approaches and considerable pre-clinical and clinical research, the prognoses of patients with GBM need to be improved (4, 5, 15-17). The poor prognoses are mainly the consequence of intracerebral recurrences. In the trial of Stupp et al., median progression-free survival was less than 7 months after tri-modality treatment with neurosurgical resection followed by concurrent radiochemotherapy (60 Gy in 30 fractions over 6 weeks plus temozolomide) and maintenance treatment with temozolomide alone (4, 5).
When experiencing a recurrence of GBM, many patients receive re-irradiation. For this situation, the optimal dose of re-irradiation needs further clarification. Since many different dose-fractionation regimens are used for re-irradiation of recurrent GBM, the doses are often given as EQD2 in order to ensure comparability of different regimens (13, 14). The EQD2 considers both the total dose and dose per fraction and is based on the linear-quadratic model. The alpha/beta ratio represents the dose, where cell killing from the linear and the quadratic components are equal. The alpha/beta ratio for tumor cell kill is considered to be 10 Gy for the vast majority of malignant tumors. In a previous meta-analysis, no significant difference regarding outcomes after re-irradiation (external beam radiation therapy) of recurrent GBM were found between EQD2 <36 Gy and ≥36 Gy (2). However, the authors stated that in several studies included in their meta-analysis, many different dose-fractionation regimens were administered and that using the median EQD2 may not be the optimal method for defining a dose–effect relationship (2). A dose–effect relationship was found in a retrospective study of 20 patients with malignant gliomas (19 with GBM) receiving hypo-fractionated stereotactic radiotherapy (HFSRT) for persistent or recurrent disease (18). Response rates were 0% after 24 Gy in eight fractions (EQD2=26.0 Gy) and 79% after 30 Gy or 35 Gy in 10 fractions (EQD2=32.5 Gy or 39.4 Gy), respectively. In another retrospective study of 19 patients (14 with GBM, five with anaplastic astrocytoma) treated with HFSRT for recurrent disease, absolute total doses (not EQD2) of ≥30 Gy resulted in a borderline significantly better median survival than doses <30 Gy (11.1 vs. 7.4 months, p=0.051) (19). Since findings regarding the optimal dose of reirradiation conflict, additional studies would help better define the optimal dose for recurrent GBM. Moreover, additional cut-off doses of the EQD2 should be investigated.
The present study compared EQD2 doses of <30 Gy to ≥30 Gy. On univariate analysis, doses ≥30 Gy were significantly superior to <30 Gy, resulting in an absolute difference of 45% points (89% vs. 44%) at 6 months and 31% points (42% vs. 11%) at 12 months. In the multivariate analysis, the results showed at least a trend. In addition, the cumulative EQD2 of the radiotherapy of the primary GBM and re-irradiation of the recurrent GBM was significantly associated with survival in both univariate and multivariate analyses; doses ≥90 Gy were significantly superior to <90 Gy.
In addition to the appropriate dose of re-irradiation, other pre-radiotherapy factors showed a significant association with survival or at least a trend. Frontal location of recurrent GBM was significantly associated with better survival in the multivariate analysis, demonstrating the main site of GBM to be an independent predictor of survival. A better performance status (KPS of 80-100%) showed a trend for being associated with better survival in both univariate and multivariate analyses, and GTR was significantly associated with improved survival on univariate analysis. These prognostic factors can be used to support physicians who aim to select a personalized treatment for a patient with recurrent GBM. Patients with one or more of these favorable prognostic factors may benefit from longer-course radiotherapy with higher doses that may be combined with systemic treatment (6). Patients without favorable prognostic factors appear more appropriately treated with short-course radiotherapy alone such as 5×5 Gy given over 1 week (12).
When considering these suggestions, one should keep in mind the limitations of the present study. These include the limited size and retrospective nature of the data always bearing the risk of a hidden selection bias. However, the 6-and 12-month survival rates of this study (75% and 32%) were similar to those reported in the meta-analysis of Kazmi et al. (73% and 36%) and within the 95% confidence intervals (69-77% and 32-40%) of that meta-analysis (2). This demonstrates consistency of the data of our present study. The consistency is further supported by the fact that the three pre-radiotherapy predictors of survival were found in other studies. In 2007, Carson et al. presented data of 333 patients with recurrent glioma and found positive associations of survival with KPS ≥80% and with tumors confined to the frontal lobe (20). Similar results were reported in a pooled analysis of 300 patients with recurrent GBM from eight phase I or II trials (21). KPS ≥80% was significantly associated with improved survival in two studies and a pooled analysis from Germany including patients with recurrent gliomas of any grade (22-24). The value of re-resection has been shown in several studies (7-11). Two of these studies performed comparisons of reirradiation with vs. without re-resection (8, 11). In the retrospective study of Skeie et al., median survival times were 9 months after Gamma Knife radiosurgery alone (n=32) and 15 months after Gamma Knife radiosurgery plus re-resection (n=19) (11). In the retrospective study of Kim et al. that included 36 patients with recurrent GBM, surgical resection when added to stereotactic radiosurgery or HFSRT was associated with significantly improved survival (p=0.010), and the extent of resection showed a trend for being positively associated with survival (p=0.071) (8).
In summary, predictors of survival after re-irradiation for recurrent GBM were identified that can help when designing personalized treatments and future clinical trials. Use of an EQD2 of re-irradiation ≥30 Gy and a cumulative EQD2 of primary and re-irradiation ≥90 Gy appeared superior to lower doses and should be administered.
Footnotes
Authors’ Contributions
The study was designed by all Authors. The data were collected by J.W. and analyzed by D.R. and S.E.S. The article was drafted by D.R. and S.E.S. and finally approved by all Authors.
This article is freely accessible online.
Conflicts of Interest
The Authors report no conflicts of interest related to the present study.
- Received October 27, 2020.
- Revision received November 2, 2020.
- Accepted November 3, 2020.
- Copyright © 2020 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.





{kind=link}
{kind=link}