


Abstract
Background/Aim: We evaluated the safety, feasibility, and preliminary efficacy of Wilms tumor gene 1 (WT1) peptide and Mucin 1 (MUC1)-pulsed dendritic cell (DC) (WT1/MUC1-DC) vaccination as an adjuvant immunotherapy for surgically resectable pancreatic ductal adenocarcinoma (PDA) patients. Patients and Methods: Eligible patients were administered WT1/MUC1-DC vaccination at least seven times every 2 weeks with concomitant adjuvant chemotherapy after surgical resection of PDA. Results: Ten patients were enrolled and no Grade 2 or higher toxicities were associated with DC vaccination. The estimated overall survival (OS) and relapse-free survival (RFS) at 3-years from the time of surgical resection were 77.8% and 35.0%, respectively. Immunohistochemical analysis suggested a possible relationship between induction of WT1-specific cytotoxic T lymphocyte after DC vaccination and higher infiltration of CD3/CD4/CD8 lymphocytes in tumor tissues. Conclusion: WT1/MUC1-DC vaccination in the adjuvant setting was safe and well-tolerated in PDA patients after tumor resection. A large-scale prospective study is warranted to evaluate the clinical benefit of this modality.
Pancreatic ductal adenocarcinoma (PDA) has been identified as an extremely aggressive malignant tumor. Most patients have relatively advanced disease at the time of diagnosis (1, 2). In spite of surgical resection being the only curative option, only a small fraction of patients with PDA present with resectable disease, and the 5-year overall survival (OS) rate remains at around 10%-15% after curative resection (1, 3). Although many cytotoxic drugs have been proven effective in treating this disease and are often used as adjuvant therapy after surgery, the median progression-free survival is still limited. Five-year survival rates remain inadequate at about 15%-25% using modern multimodal treatment strategies. Therefore, there is an urgent need to devise novel strategies for PDA treatment.
Recently, immunotherapy has been proposed as a new treatment approach for such cancers with poor prognosis including PDA (4), and various methods have been considered. Selection of a tumor-associated antigen (TAA) is an important consideration in cancer immunotherapy. The ideal TAA target should be expressed only on tumor cells, as they have very limited expression on normal tissues, and will produce the greatest effect on tumor cell survival. In a pilot project conducted to prioritize 75 known cancer antigens for this purpose, Wilms tumor gene 1 (WT1) antigen was identified as the most suitable (5). WT1 has been originally defined as a tumor suppressor gene encoding a zinc finger DNA-binding protein (6), which is involved in tumorigenesis through transcriptional regulation of several genes (7-9). The WT1 antigen is highly expressed in various malignancies, including PDA (10), and can have oncogenic functions (11). MUC1 (mucin-1, CD227) is a polymorphic, glycosylated type I transmembrane protein present in the glandular epithelium of different tissues, including the pancreas, breast, and lung, and it has been reported to be over-expressed in 90% of PDA tumors (12-14). MUC1 inhibits cell-cell and cell-stroma interactions and functions as a signal transducer promoting cancer progression characterized by tumor invasion and metastasis (15). Most tumor antigens are characterized by major histocompatibility complex (MHC)-restriction, whereas MUC1 recognition by cytotoxic T-lymphocytes (CTL) is not MHC-restricted. Furthermore, MUC1 has also been reported as a highly promising TAA for cancer immunotherapy (5). Therefore, WT1 and MUC1 have been used as immunotherapy targets for PDA.
Dendritic cells (DC) are widely considered to be the most efficient antigen-presenting cells responsible for T cell activation and are the link between innate and adaptive immunity (16). With the identification of TAAs, TAA-pulsed autologous DCs generated ex vivo by culturing monocytes with cytokine combinations have been used for therapeutic cancer vaccination (17). Comparative studies have suggested that TAA peptide-pulsed DC vaccines may elicit more CTL activity than peptides alone (18). Numerous studies suggest that DC-based vaccination is an ideal modality for immunotherapy for cancers including PDA (19, 20). However, most clinical trials regarding PDA have targeted advanced disease; thus, the significance of this therapeutic modality in surgically resectable patients remains to be unresolved.
Here, we conducted a phase I/IIa clinical study of WT1 peptide and MUC1-pulsed DC (WT1/MUC1-DC) vaccination as an adjuvant immunotherapy for resectable PDA patients. In addition to evaluating the feasibility, safety, and antitumor efficacy of this therapy, we evaluated various immunological parameters that may be correlated with the induction of immune responses and antitumor effects. In particular, we have focused on the immunological characteristics of the tumor microenvironment using immunohistochemical methods on resected tumor tissues.
Patients and Methods
Study design. This phase I/IIa open-label study was conducted between June 1, 2013 and February 6, 2019. The primary objectives of the study were to evaluate the safety, tolerability, and feasibility of DC-based vaccination pulsed with WT1 peptide and MUC1 as an adjuvant therapy for enrolled patients who underwent their respective operations for pancreatic cancer. The secondary objective was to evaluate potential predictive immunological and histochemical biomarkers associated with clinical activity and/or safety. The cutoff for data collection was December 31, 2018.
Patients. Candidates for this study were consecutively enrolled during the registration period. Eligible patients met the following criteria: 18 to 80 years of age, were diagnosed with PDA, underwent respective operations after initial diagnosis, had Eastern Cooperative Oncology Group performance status (PS) of 0-1, had normal organ function, had no chemotherapy-disqualifying sign of infectious disease, had no blood abnormality or bleeding tendency, had no apheresis-disqualifying history of cardiovascular disease or respiratory disorders, and had human leukocyte antigen (HLA) class I genotypes compatible with restriction of the WT1 peptide. Furthermore, we confirmed the expression of WT1 protein and HLA class I (ABC) in resected PDA tissue using the immunohistochemical (IHC) methods described below in advance of registration. Expression of both proteins in PDA cells was required for registration to this study. Patients who received chemotherapy before surgery or were diagnosed within 6 months with other cancers were excluded from the study.
Production of WT1 peptide and MUC1-loaded DC vaccine. The WT1/MUC1-DC vaccine was prepared as previously reported (21), by a well-trained technical staff in the cell processing facility (CPF) of Nagasaki University Hospital under standard operating procedures (SOP) compliant with Good Gene, Cellular, and Tissue-based Products Manufacturing Practice. Briefly, leukapheresis was carried out when patients' peripheral white blood cell (WBC) count, hemoglobin concentration, and platelet count were above 2000 cells/μl, 9.0 g/dl, and 90,000 cells/μl, respectively. Peripheral blood mononuclear cells (PBMNCs) were isolated from leukapheresis products by Ficol-Hypaque (GE Healthcare Japan, Tokyo, Japan) gradient density centrifugation. PBMNCs were then cultured in tissue-culture plates, and adherent cells were harvested. Adherent cells were cultured in AIM-V medium (Gibco/Thermo Fisher Scientific, Yokohama, Japan) containing human recombinant granulocyte-macrophage-colony-stimulating factor (GM-CSF, 50 ng/ml, NCPC Genetech, Shijiazhuang, China) and human recombinant interleukin-4 (IL-4, 50 ng/ml, R&D Systems, Minneapolis, MN, USA) in order to generate immature DCs. Five days later, DCs were loaded with HLA-A*24:02-restricted WT1 (235-243: CYTWNQMNL) (mutant WT1 peptide, Neo-MPS; San Diego, CA, USA) and HLA-A*02:01/02:06-restricted WT1 peptide (126-134: RMFPNAPYL) (WT1 peptide, Neo-MPS) according to the compatibility of each patient's HLA typing. DCs were then stimulated with OK-432, streptococcal preparation (10 μg/ml, Chugai Pharmaceutical, Tokyo, Japan), prostaglandin E2 (PGE2, 50 ng/ml, Daiichi Fine Chemical, Tokyo, Japan), IL-4 (5 ng/ml), and granulocyte-macrophage colony-stimulating factor (5 ng/ml) for 24 h for maturation. MUC1 was added to the DC culture media concomitantly with OK-432 and PGE2. The MUC1 long peptide TRPAPGSTAPPAHGVTSAPDTRPAPGSTAP (Greiner Japan, Tokyo) was used for all HLA-A types. DCs were harvested, washed, and dissolved in AIM-V medium containing 10% dimethyl sulfoxide (DMSO, Nipro, Osaka, Japan) and 10% human albumin (Nihon Pharmaceutical, Osaka, Japan) and dispensed to cryo-tubes at approximately 1×107 cells per tube. After pre-freezing at −80°C for 4 h, DCs were cryo-preserved at −150°C in a deep freezer until the day of administration.
Criteria for DC vaccine release. Flow cytometry was used to determine the antigenic profiles of mature DCs. Mature DCs were defined as CD11c+, CD14−, HLA-DR+, HLA-ABC+, CD80+, CD83+, CD86+, CD40+, and CCR7+ cells. The following criteria were required for DC vaccine administration: purity (proportion of CD11c+, CD14−, CD86+, and HLA-DR+ cells >90%), >80% viability, mature DC phenotype, negative for bacterial and fungal infection after 14 days, endotoxin ≤0.05 EU/ml, and negative for mycoplasma.

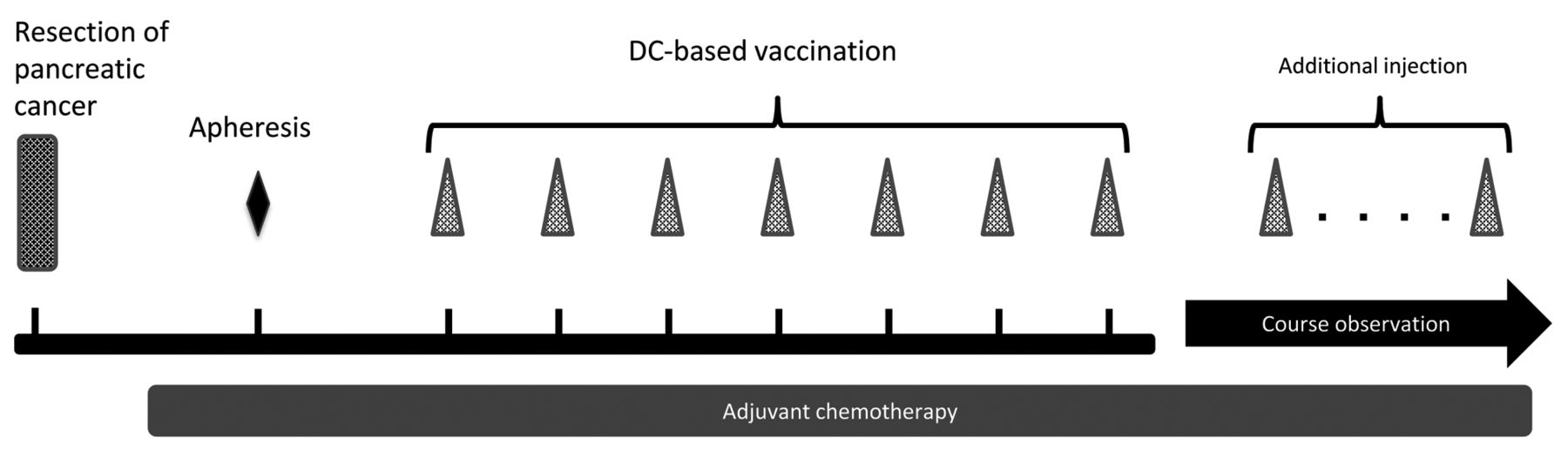
Treatment protocol schema. Harvested PBMNCs were processed and cultured for 14 days at the CPF of Nagasaki University Hospital. Cell products underwent quality inspections and were confirmed to meet shipping criteria. WT1 peptide and MUC1-pulsed DC (107 cells/injection) were injected intradermally at least seven times every 2 weeks. Concomitant administration of adjuvant chemotherapeutic agents was allowed in this study.
Treatment. A schematic of the trial design is given in Figure 1. The vaccination regimen has been described previously (21). Briefly, cryo-preserved DCs were thawed, washed with physiological saline (Otsuka Pharmaceutical, Tokyo, Japan) containing 10% dextran (10 mL, Otsuka Pharmaceutical) once, and washed with physiological saline (10 ml) twice to get rid of the remaining DMSO and human albumin. WT1/MUC1-DCs were suspended in a total volume of 1 ml of physiological saline, and approximately 1×107 WT1/MUC1-DCs were injected intradermally at four positions in the axilla and groin regions on each side (approximately 0.25 ml at each position). They were administered seven times in 2-week intervals. OK-432 was administered subcutaneously in each axilla (0.5 ml each) in the vicinity of vaccination sites to activate DC functions. Administration was initiated at a dose of 1 Klinische Einheit (KE, clinical unit) and increased to 5 KE if no side effects were observed.
In this study, concurrent adjuvant chemotherapy was acceptable. Chemotherapy was selected by the referring surgeons and included the oral tegafur-gimeracil-oteracil potassium combination agent S-1 in eight patients and gemcitabine (GEM) in one patient. S-1 was administered orally at a daily dose of 80-120 mg for 14-28 days with 1-2 weeks rest repeated every 3-6 weeks. GEM 100 mg/m2 was administered on day 1 and repeated every 3 weeks with 1-2 weeks rest. In one patient, no adjuvant chemotherapy was administered because of the patient's refusal.
Evaluation of adverse events (AEs). AEs were monitored and graded according to the National Cancer Institute's Common Terminology Criteria for Adverse Events Version 5.0 (CTCAE ver.5.0), including hematological (leukocytopenia, neutropenia, anemia, and thrombocytopenia) and non-hematological AEs (fatigue, nausea, diarrhea, constipation, anorexia, pain, hypertension, stomatitis, hematuria, pollakiuria, micturition pain, neurological symptoms, fever and abnormality in kidney function, electrolytes, or liver function) during or after treatment completion until the end of this study (22). Skin reactions at the injection site and fever, which are known AEs resulting from DC administration, were assessed after 24, 48, and 72 h after each vaccination in all patients. Furthermore, safety evaluations were undertaken for allergic reactions after intradermal injection of DC vaccine. Monitored symptoms included the presence of reduced blood pressure, tachycardia, breathing difficulties, or urticaria.
Evaluation of clinical response. The analysis of target populations in this study were as follows: 1) maximum analysis target group (cases excluded from eligible cases that did not receive therapy), 2) safety analysis target population (the maximum analysis target population), and 3) progression-free and overall survival analysis target cases (the maximum analysis population).
We evaluated OS and relapse-free survival (RFS) at 3 years post-surgery, which was concomitant with the induction of WT1-specific CTLs during DC vaccination targeting WT1 in pancreatic cancer. Imaging techniques including computed tomography and positron-emission tomography/computed tomography were also used for post-surgical assessment of lesions. The clinical response after administration of the WT1-DC vaccine was determined according to Response Evaluation Criteria in Solid Tumors (version 1.1) (RECIST v1.1) (23). RFS has been defined as the lesser of the number of days until relapse of disease as determined by RECIST criteria or the number of days until death. RECIST criteria were evaluated 4 weeks after the final administration. After that, evaluation was repeated until relapse was determined. The follow-up period was 2 years from the first administration of DC vaccination for each participant.
Evaluation of WT1-specific CTLs. PBMNCs were obtained before initiating the first vaccination and at the completion of the seventh vaccination. The WT1 tetramer assay was performed only in patients who received the HLA-A*24:02-restricted mutant WT1 peptide. WT1 tetramer was assessed in the CD3/CD8 double-positive population using WT1-modified peptides/HLA-A*24:02 tetramers (MBL, Medical & Biological Laboratories Co., Ltd., Nagoya, Japan) (24).
IHC analysis of primary tumor samples. We analyzed resected samples of pancreas tumor from enrolled patients using a previously described IHC method (24, 25). For expression analysis of WT1 and HLA-ABC proteins in tumor cells, we used mouse monoclonal anti-WT1 (6F-H2; Dako, Carpinteria, CA, USA) and anti-HLA-ABC antigen antibodies (class I, W6/32; Dako). Negative control staining was applied to all samples using a mouse IgG isotype control monoclonal antibody (X0931; Dako). The intensity of WT1 protein expression observed in PDA cells was classified as follows: (i) negative; (ii) weak, faint, and barely perceptible cytoplasmic staining; (iii) moderate, moderate complete cytoplasmic staining; and (iv) strong, strong complete cytoplasmic staining (25). In addition, to analyze the immunophenotypes of tumor-infiltrating mononuclear cells, we used monoclonal antibodies binding CD20 (L26; Dako), CD3 (LN10; Leica, Nussloch, Germany), CD4 (1F6; Leica), CD8 (4B11; Leica), CD25 (4C9; Leica), FOXP3 (SP97; AbCam, Cambridge, UK), TIA1 (2G9A10F5; Beckman Coulter, Brea, CA, USA), and Programmed Cell Death-1 (PD1) (NAT105; AbCam) for these analyses. Observation was carried out using high-magnification light microscopy (400×). Expression was scored as negative if <5% of cells were positive, 1+ if 5% to 10% of cells were positive, 2+ if 10% to 30% were positive, 3+ if 30% to 60% were positive, and 4+ if >60% were positive. Two investigators who were not privy to the requisite clinical information independently interpreted the IHC results.
Clinical characteristics of registered cases.
Production and administration profile of DC vaccination.
Statistical analysis. We compared the results of tetramer assays before and after administration of the WT1-DC vaccine using the Wilcoxon signed-rank test. We used a Kaplan–Meier curve to evaluate OS and RFS and compared those measures between groups using the log-rank test. All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan). A p-value of less than 0.05 was considered statistically significant.
Ethics statement. The protocol for WT1-DC vaccination therapy at the Nagasaki University Hospital was approved by the Ethics Committee of Nagasaki University School of Medicine (approval number: 12102231). The Act on the Safety of Regenerative Medicine in Japan was enforced on November 25, 2014. Class III technologies were regarded as low-risk since they used somatic cells and accumulated clinical experiences. DC vaccination therapy (Class III technology) at the Nagasaki University was approved on November 25, 2015 (approval number: PC3150643). Written informed consent was obtained from all the patients. All procedures performed in this study were in accordance with the Ethical Guidelines for Medical and Health Research involving Human Subjects proposed by the Ministry of Health, Labour and Welfare in Japan (26). The trial was registered with the University Hospital Medical Information Network (UMIN) Clinical Trials Registry (27).
Results
Characteristics of enrolled patients. Table I shows the clinicopathological characteristics of the patients who were enrolled in the present study. Patients' ages ranged from 56 to 76 years old (median 62.5 years old), and their PS was well maintained. Clinical stage varied from IA to III (28) and curative resection was performed in all cases. Laboratory data regarding C-reactive protein (CRP), neutrophil-to-lymphocyte ratio (NLR), and prognostic nutritional index (PNI) were obtained for all patients. In the present setting, stable nutritional status was indicated, and NLR and CRP/albumin ratios indicated only minimal inflammatory status in all patients after resection (Table I).
Expression of WT1 and HLA-ABC in the surgical specimens of all the 10 patients with pancreatic cancer was confirmed. We classified IHC staining intensity of cytoplasmic WT1 in tumor cells into three categories, weak, moderate, and strong, as described by Kanai et al. (25). Strong, moderate, and weak staining patterns were observed in four, four, and two of ten cases, respectively.
DC-based vaccine preparation and characterization. Table II shows data related to the preparation of the DC-based vaccine. Apheresis of monocytes from peripheral blood was carried out in all patients. There were no adverse responses during apheresis. The numbers of harvested PBMNCs ranged from 339.0×107 to 814.0×107 cells (median 560.5×107 cells), allowing to reach the target cell number required to prepare and ship DC products.
Mature DCs were injected at a dose of 11.3×107 to 28.0×107 cells per vaccination (median 22.5×107). Seven patients received WT1 peptide-pulsed vaccination restricted to HLA-A*24:02. Patients received 7-12 vaccinations (median 7). The total dose of OK-432 was 18-23 KE (median 20.5 KE). The maximum dose of OK-432 per session was 5 KE.
Safety and toxicity. AEs were reported in a total of nine (90.0%) patients. As indicated in Table III, the most common AE of any grade was skin reaction (erythema) at the DC vaccine injection site (n=9, 90.0%). Meanwhile, fever (n=6, 60.0%) was observed in six patients, including three patients (30.0%) with Grade 1 fever (>38°C). Both AEs recurred in most cases and disappeared after a few days. Grade 1 fatigue was observed in six patients (60.0%). Grade 1 leukocytopenia, neutropenia, and anemia were observed in 3, 3, and 1 of the 10 patients, respectively. Other non-hematologic AEs included grade 1 anorexia, diarrhea, hepatic transaminase, and γ-glutamyl transpeptidase elevation, all of which have been previously reported as major AEs associated with S-1 or GEM. Overall, no Grade 2 or higher CTCAE v5.0 toxicities were found to be associated with DC vaccination. Therefore, no patient discontinued DC vaccination. Although four patients died during the observation period, relapse and progression of PDA was the cause of death in all four patients as described below.
Therapy-emergent adverse events profile of DC vaccination (Number of patients).
Clinical outcome. As shown in Table IV, seven of the ten patients relapsed, and the final outcome recorded six deaths because of recurrence and disease progression. The maximum follow-up period was 65 months after completion of vaccine administration. The OS and RFS from the time of surgical resection were 18.5-72.8 months (median 46.4 months) and 12.5-72.8 months (median 17.7 months), respectively. As shown in Figure 2, the estimated OS and RFS at 3-years were 77.8% (95%CI=0.37-0.94) and 35.0% (95%CI=0.09-0.64), and those at 5-year were 19.4% (95%CI=0.01-0.55) and 23.3% (95%CI=0.04-0.53), respectively. There were no statistically significant correlations between various clinical parameters and OS or RFS.
Clinical and immunological response to DC vaccination.
Immune response. As described above, a skin reaction was observed in nine of ten patients (90.0%) after vaccination. In all nine cases, skin reactions emerged around 48 h after the first vaccination and recurred after each vaccination. All skin reactions were Grade I and resolved within a week. In four of nine patients, the diameters of skin reactions were measured to be over 3 cm (Patients 1, 7, 8, and 9). No correlations were found between skin reaction and PFS or OS.
Tetramer assays were performed for each of the five patients treated with WT1-pulsed therapy who received the HLA-A*24:02-restricted mutant WT1 peptide. WT1-specific CTLs were detected after vaccination in four patients (Table IV, Figure 3). Although positive tetramer assays and longer survival tend to be related, no statistically significant correlations were found between tetramer assay results and OS or RFS in the present study.
IHC characteristics of tumor cells and tumor microenvironment. In the present study, IHC staining revealed that WT1 protein expression was detected in the nuclei and cytoplasm of PDA samples from all patients. WT1 proteins were found to predominantly localize to the cytoplasm in all cases. Patients were subdivided into three groups according to cytoplasmic WT1 staining intensity in PDA cells: weak (4/10 cases), moderate (3/10 cases), and strong (3/10 cases) (Table I). There were no correlations between cytoplasmic WT1 intensity and various clinicopathological parameters, including age at surgical resection, sex, and tumor characteristics. The median survival time for patients with PDA with weak and moderate-to-strong cytoplasmic WT1 expression was 46.4 and 50.5 months, respectively. However, there were no correlations between the cytoplasmic WT1 staining intensity and OS or RFS. In all 3 cases that were strongly positive for WT1 (Patients 1, 3 and 4), induction of WT1-specific CTL was observed by tetramer analysis (Table I and IV, Figure 3).
IHC findings of infiltrating MNCs in tumor tissue are summarized in Table V. There were varying levels of infiltrating MNCs in all patients, and CD3-positive cells were the most common. In Patients 1, 3, and 6, there were more infiltrating CD8-positive cells than in the other cases. In eight of ten patients, there was moderate infiltration of TIA1-positive mononuclear cells. Infiltration of PD1-positive MNCs was observed in seven patients. Although the degree of infiltration of CD8 positive cells is typically associated with longer survival, no such statistically significant correlations were found between tumor-infiltrating MNC immunophenotypes and OS or RFS. Moreover, although the statistical significance was not clear because of the limited case numbers, there was a tendency for induction of WT1-specific CTL after DC vaccination in cases with a higher degree of infiltrations of CD3+, CD4+, or CD8+ MNCs (Figure 3).
Discussion
We report the results of a phase I/IIa clinical trial of the WT1/MUC1-DC vaccination combined with chemotherapy (mainly S-1) after resection in patients with an initial diagnosis of PDA. To the best of our knowledge, this study is the first to report on the safety and feasibility of DC-based tumor-specific vaccination using a combination of WT1 peptide and MUC1-DC for PDA as an adjuvant setting after surgical tumor resection.
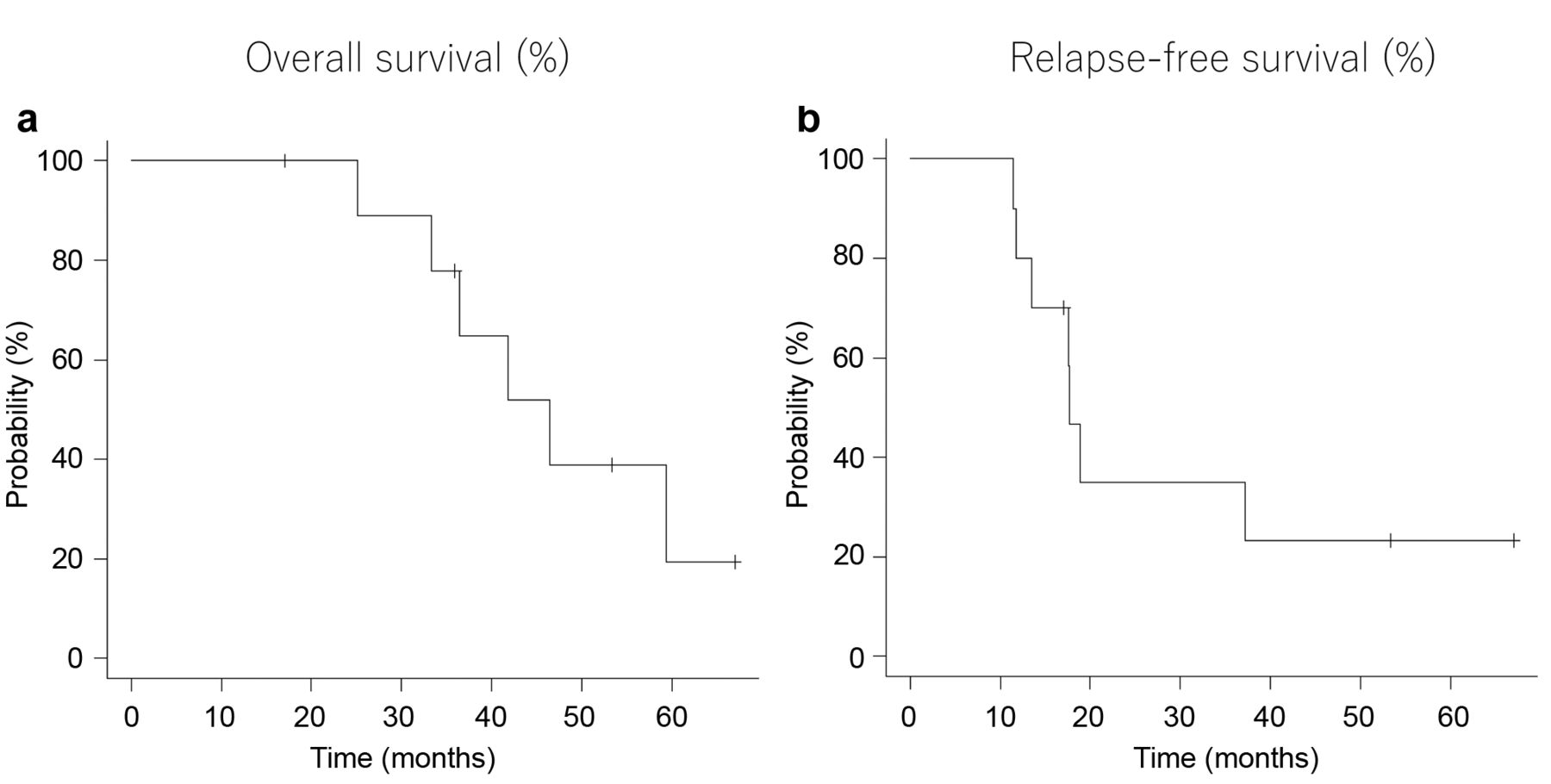
Kaplan–Meier plots of the survival of enrolled patients (n=10) from the day of surgical resection of PDA. a) Overall survival (median 46.4 months), b) Relapse-free survival (median 17.7 months).

Correlation between clinical outcome and immunopathological findings. Numbers indicate all patients listed in Table I. Each bar graph indicates the survival period from surgical resection of the PDA tumor. Down arrows indicate time point of relapse. Cross markers indicate death of each case. tet: WT1-specific CTL by tetramer assay; wt1: expression of WT1 protein in tumor cells of PDA by IHC; NE: not evaluable. As to the description in “tet”: (−), (1+) and (2+) represent the difference in positivity between post- and pre-vaccination as being less than 0.1%, between 0.1% and 1.0% and more than 1.0 %, respectively. As to the description in “wt1”: +++; strong, ++; moderate, +; weak (25). As to the description in IHC findings for CD3, CD4, and CD8: −, <5% of cells were positive; +, 5% to 10% of cells were positive; ++, 10% to 30% were positive; +++, 30% to 60% were positive; and ++++, >60% were positive.
The safety profile was the primary end point. No grade 2 or higher CTCAE v4.0 toxicities were found to be associated with DC vaccination. Skin reactions at the injection site and fever were the main AEs considered to be related to DC vaccination. These AEs were transient and manageable with symptomatic treatment and without any delay of treatment schedule. Previous reports have indicated the safety and feasibility of TAA peptide-pulsed DC vaccination as an adjuvant therapy after surgical PDA resection (29, 30). Lepisto et al. reported that no treatment delay occurred due to AEs in patients with PDA or biliary cancer who were treated with MUC1-pulsed DC vaccination after surgical tumor resection (29). Yanagisawa et al. have also reported that fever and skin reaction at the injection site were frequently observed but were transient and tolerable in their pilot study of WT1 peptide-pulsed DC vaccination for patients with PDA after tumor resection (30). Grade 1 fatigue in some patients was associated with fever during administration, and both were relieved concurrently. Fatigue in others was persistent, which may have been due to concomitant chemotherapy. Other hematological and non-hematological AEs were consistent with frequently observed events associated with concomitant chemotherapy. Altogether, this strategy should be considered safe and feasible for patients with PDA as an adjuvant therapy after surgical resection.
Immunohistochemical profiles of infiltrating immune cells in tumor tissue.
Since PS and WBC counts were well maintained even in patients who started their adjuvant chemotherapy after resection as shown in Table I, leukapheresis for harvesting DCs was carried out successfully and safely from all patients. At the time of shipment, it was confirmed that the prepared DCs had the immunophenotype of mature DCs. It has been confirmed that mature DCs produced by equivalent preparation methods have sufficient function in T cell proliferation stimulation and secretion of IL-12 and interferon γ (IFNγ) in ex vivo assays (31, 32). Thus, we believe that well-defined SOPs can be used to prepare sufficient quantities of stable, high-quality DC vaccines derived from autologous peripheral blood, even in the clinical setting.
In our study, the median OS and RFS were 46.4 months and 17.7 months, respectively, and the 5-years OS and RFS were 19.4% and 23.3%, respectively. These results were comparable to recent findings from previous clinical trials of surgical resection followed by adjuvant chemotherapy for PDA, in which 5-year survival ranged from 10% to 25% (33-35). Several phase III trials in recent years have demonstrated the survival benefit of post-resection adjuvant chemotherapy (33-36) and the usefulness of GEM or fluorouracil in the adjuvant setting (34). The JASPAC 01 study has revealed that S-1 had better efficacy in preventing recurrence than GEM for resected PDA (36). In their study, in the S-1 group, the estimated OS at 3-years and 5 years were 59.7% and 44.1%, and RFS were 39.2% and 33.3%, respectively. While, 9 of 10 cases were treated with S-1 as adjuvant chemotherapy and the estimated OS and RFS at 3 years were 77.8% and 35.0%, respectively, in the present study. Thus, these data suggested that the higher estimated OS at 3 years compared to JASPAC 01 study might be a unique characteristic of cancer vaccination that could not be adequately captured by the RECIST criteria. Further, add-on DC vaccination in this study enabled us to obtain data on the clinical efficacy compared to that of conventional post-resection adjuvant chemotherapy. However, controversies remain regarding the immunological efficacy of the combined use of WT1 peptide and MUC1. Although it is difficult to make a rigorous comparison with the previous studies in which every single vaccination was performed (29, 30), its add-on effect on survival could not be clarified. Large-scale controlled trials are warranted to clarify the clinical significance of these findings. Recently, Koido et al. have shown that multiple DC vaccinations with both MHC class I and II-restricted WT1 peptides not only stimulated CTL but also maintained long-term memory T cells that were specific to WT1, and that this phenomenon was significantly linked to beneficial clinical outcomes of patients with advanced PDA (37). Therefore, the introduction of such novel vaccination methods might be associated with improvement of the long-term prognosis of patients with PDA as an adjuvant therapy.
We assessed the associations of the prognosis of PDA patients who received surgical resection with several inflammatory and immunological findings. Previous studies on several types of cancer have reported that laboratory data indicating systemic inflammatory response can serve as markers of poor prognosis in patients undergoing treatment that includes immune cellular therapy (38-40). In the present setting, NLR and CRP/albumin ratio results indicated only minimal inflammatory status in patients after resection. Thus, such a post-operative immunologic status may be favorable for immunologic induction through DC vaccination.
Our previous report has indicated that delayed skin reaction at the DC injection site may be correlated with long-term survival in DC-treated patients with advanced cancer (41). Previously, it has been indicated that such a local response represents an important source of information concerning in vivo T cell function and TAA-specific T cells (42). Thus, delayed local skin reactions may have significance regarding tumor-specific immunogenicity. However, we did not detect a significant correlation between clinical efficacy of DC vaccination or WT1-specific CTL induction detected by tetramer assay and enhancement of delayed skin reaction. Further studies are needed to clarify whether such local skin reaction after DC vaccination definitively reflects a therapeutic effect and whether monitoring skin lesions might be a simple approach to evaluate the immunogenicity of vaccination.
Recent studies have confirmed that different types of host immune cells co-exist and interact with tumor cells in the tumor microenvironment (43-45). In the networks formed between varied cellular and molecular factors, various interactions have been shown to provide important signals to initiate the growth of cancer cells and promote invasion into blood vessels and lymph nodes leading to tumor metastasis. Furthermore, it has been considered that the local immune response in the tumor microenvironment could modulate the clinical outcome and is used as a prognostic factor of solid tumors, including PDA (46). Tewari et al. (47) have shown a correlation between prognosis and the presence of tumor-infiltrating T cells. Homma et al. (48) have found that CD4+ and CD8+ cells were significantly increased after neoadjuvant chemotherapy with gemcitabine and S-1 and subsequent radiation therapy and that high CD4+ cell accumulation was an excellent prognostic marker for PDA treated with this regimen. In the present study, we did not detect statistically significant correlations between prognostic data and the degree of infiltration of various types of immune cells, although a higher degree of infiltration of CD3+, CD4+, or CD8+ MNCs indicated a trend toward induction of WT1-specific CTL after DC vaccination. However, our immunohistochemical analysis was limited in scope, and considering the complexity of the tumor microenvironment, examination of additional factors is needed to clarify the clinical impact of increased infiltration following vaccination. We posit that it may be necessary to develop a combined index for this purpose. Recently, several groups have highlighted important future directions in the research of this subject (49, 50). In this context, resected tumor tissue may become important to predict each patient's prognosis and to develop treatment strategies including immunotherapy.
There were several limitations to this study. Due to the small number of samples analyzed, it was not possible to adequately discern the clinical effect of this treatment method, various clinical parameters, immunological findings, and association with IHC findings, including WT1 expression in tumor cells and infiltration of various immune cells. The purpose of this study was to clarify the safety and feasibility of this treatment, for which the sample size was adequate. Previous trials of DC vaccination for PDA indicated its safety and clinical effects and revealed several prognostic markers, including reduced NLR, increased expression of HLA-DR on DCs, and a lack of increased interleukin-6 levels in peripheral blood after administration. However, these findings were in the context of advanced PDA, leaving the clinical safety, feasibility, and efficacy of this treatment unproven in the setting of resectable disease. Thus, a larger sample size will be required to clarify and confirm the clinical and biological implications of this therapy in the setting of resectable PDA. Additionally, we did not carry out testing of MUC1-specific immune reaction due to technical limitations. It is not clear whether tumor reduction by surgical resection has a differential effect on the tumor immunity obtained by the DC vaccination as compared with the case with a larger tumor burden. Thus, in vivo monitoring of TAA-specific immunity to minute residual lesions or micrometastasis might require longer-term observations than the setting of our study (30). It is necessary to clarify the clinical significance of DC vaccination and TAA-specific CTL detection by observing changes over time and by increasing the number of analysis points after DC vaccination.
In conclusion, the present phase I/IIa study evaluating WT1 peptide and MUC1-pulsed DC vaccination in combination with chemotherapy in patients with resected pancreatic cancer demonstrated the safety and feasibility of this therapy in the adjuvant setting. It was suggested that there appeared to be a survival benefit of add-on DC vaccination in this study compared to that of conventional post-resection adjuvant chemotherapy. A large-scale prospective study is warranted to evaluate the clinical benefit of this strategy and to elucidate biological markers of prognosis and tumor-specific immunogenicity focusing on the tumor microenvironment.
Acknowledgements
The Authors thank the patients who participated in this study and the referring surgeons who performed concomitant therapy and provided follow-up information. The Authors also thank Dr. Wataru Uegami (Department of Pathology, Nagasaki University Hospital) for his helpful advice on the pathological analysis. This study was supported in part by Grants-in-Aid for Scientific Research from the Japan Society for Promotion of Science (26221005). This study was funded by Tella Inc., Tokyo, Japan.
Footnotes
↵* These Authors contributed equally to this work.
Authors' Contributions
All Authors had access to the data and participated in data collection and interpretation. K.N. and T.A. conceived and designed the study; H.H. and K.N. performed production and quality management of DC products; K.N. and T.A. acquired the data; K.N. and H.H. performed pathological observation and analysis; K.N., T.A., and S.E. analyzed and interpreted the data; H.H. performed the statistical analysis; K.N. and T.A. wrote the manuscript; H.S. provided technical advices; and S.E., H.S. and Y.M. supervised the project. All Authors approved the final version of the manuscript.
This article is freely accessible online.
Conflicts of Interest
Nagai K. was funded for this research by Tella Inc. Adachi T., Harada H., Eguchi S., Sugiyama H. and Miyazaki Y. have no conflicts of interest directly relevant to the content of this article.
- Received August 17, 2020.
- Revision received August 31, 2020.
- Accepted September 1, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.