


Abstract
Background/Aim: To evaluate the outcomes of curative resection for Borrmann type IV gastric cancer through an analysis of the clinical, surgical and pathological data and through identifying which of these prognostic factors are associated with survival. Patients and Methods: We retrospectively analyzed 2798 patients who had undergone excision of the primary lesion and 122 patients with type IV gastric cancer undergoing curative resection (R0 or 1) at Yokohama City University Hospital and Kanagawa Cancer Center between November 1995 and May 2016. Results: Borrmann type IV gastric cancer had more advanced and unfavorable clinicopathological factors compared to other types. The 5-year overall survival rate was 28%, and the median survival was 21.8 months. The overall survival rate was influenced by the depth of invasion, lymph node metastasis, peritoneal lavage cytology (CY), stage and intraoperative blood loss. Of these, independent prognostic factors were intraoperative blood loss (<400 vs. ≥400 ml, risk ratio 1.64; p=0.045) and CY (0 vs. 1, risk ratio 2.25; p=0.004). Conclusion: The control of intraoperative bleeding had a positive impact on the survival of patients receiving curative resection for Borrmann type IV gastric cancer.
Gastric cancer is the fifth-most common malignancy and was the third leading cause of cancer-related death in 2018 (1). Radical gastrectomy with regional lymph node dissection is indispensable for curing localized gastric cancer (2). However, recurrence may occur in 20%-60% patients even if complete resection is achieved (3, 4).
The prognosis of advanced gastric cancer depends on a variety of different factors, including the tumor size, depth of invasion, nodal metastases and pathological type (5, 6). The classification of advanced gastric cancer according to Borrmann's criteria is presently accepted worldwide by endoscopists and surgeons. Among advanced gastric cancer types, Borrmann types I and II have relatively good outcomes, whereas the survival outcomes of Borrmann type IV cancer, known as linitis plastica, are extremely poor (1, 7-9). Although several neoadjuvant and postoperative adjuvant chemotherapies have been established, their effect on the long-term prognosis of Borrmann type IV gastric cancer is still insufficient (10). This is due in part to patients who undergo postoperative chemotherapy often having an inadequate nutritional intake, resulting in postoperative chemotherapy of insufficient dose intensity (11). The prognosis of patients with Borrmann type IV gastric cancer is poor, with a 5-year overall survival rate after gastrectomy ranging from 10.5% to 27.6% (12).
A number of potential prognostic factors have recently been reported, such as perioperative blood transfusion and intraoperative blood loss. Burrow et al. (13) first reported the risk connected with perioperative blood transfusions in colorectal cancer patients in 1982. For gastric cancer, Kaneda et al. (14) reported that blood transfusion was correlated with a poor outcome. Similarly, excessive intraoperative blood loss increases the risk of postoperative recurrence and of a poor prognosis in patients with several cancers. However, there are still few articles concerning the correlation between intraoperative blood loss and long-term outcome of patients with gastric cancer.
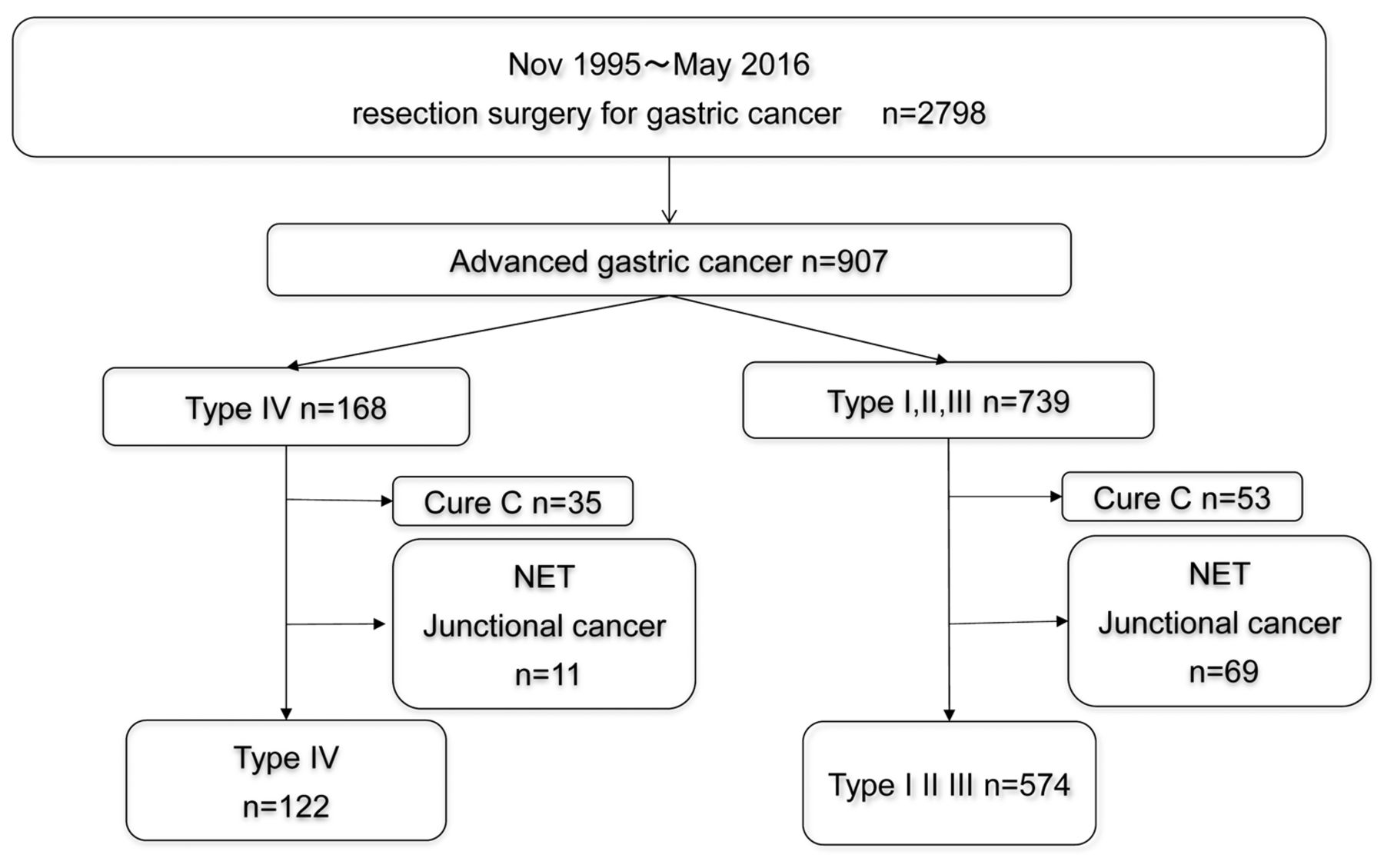
Consort diagram.
Comparison of patient background factors between the Borrmann type IV gastric cancer and other Borrmann types.

Relapse-free survival with Borrmann type I-III and type IV gastric cancer.
In this study, we performed a large-scale, retrospective, multi-center cohort analysis of stage II or III Borrmann type IV gastric cancer with curative gastrectomy to compare the outcomes with those from other types of cancer and clarify the significance of clinicopathological features, such as intraoperative blood loss, on survival.
Patients and Methods
Patients. The patients were retrospectively selected from among the medical records of consecutive patients who underwent gastrectomy with nodal dissection for gastric cancer at Yokohama City University and Kanagawa Cancer Center from November 1995 to May 2016. Patients with the following criteria were included: 1) histologically proven gastric adenocarcinoma, 2) D2 or D1+ gastrectomy with curative lymph node dissection as the first treatment and 3) achieved complete (R0 or R1) resection.
In principle, D1+ gastrectomy was selected for clinical T1 cancer, while D2 gastrectomy was selected for clinical T2-T4 disease according to the Japanese gastric cancer treatment guidelines, ver. 3. The resected specimens were histopathologically examined and staged according to the Japanese classification of gastric carcinoma: 3rd English edition. The location of lesions was determined by the macroscopic appearance of the surgical specimen and from a postoperative histological examination after the stomach was divided into three parts (upper, middle and lower).
All patients who underwent radical gastrectomy from November 1995 to May 2016 were followed up at an outpatient clinic and received surgery alone. After August 2006, pathological stage II and III patients received S-1 adjuvant chemotherapy based on the ACTS-GC trial, which became the standard treatment for advanced gastric cancer.
Patients were followed up at outpatient clinics. The dates and causes of death were collected from the follow-up data based on hematological tests and physical examinations performed at least every three months for the first three years after surgery and then every six months until five years after surgery. The serum CEA and CA19-9 levels were checked at least every three months for five years. Patients underwent a computed tomography (CT) examination every six months during the first three years after surgery and then every year until five years after surgery. Postoperative complications of grade 2-5 according to the Clavien-Dindo classification that occurred during hospitalization and/or within 30 days after surgery were retrospectively determined from the patient's records. Grade 1 complications were not evaluated in order to exclude the possibility of a description bias in the patient's records.

Overall survival with Borrmann type I-III and type IV gastric cancer.
Statistical analyses. The significance of the correlation between the Borrmann Type I-III group, Borrmann Type IV group and clinicopathological parameters was determined using Fisher's exact test or the χ2 test and the Mann–Whitney U-test for continuous variables. The overall survival (OS) was defined as the period between surgery and death. Recurrence-free survival (RFS) was defined as the period between surgery and recurrence or death, whichever came first. The data of the patients who did not experience an event were censored on the date of the final observation. OS and RFS curves were calculated by the Kaplan–Meier method and compared by the log-rank test. OS was evaluated by univariate and multivariate analyses using Cox's proportional hazard model. To select a model, we used backward elimination in the multivariate analysis. Patients with missing covariate values were excluded. Standard clinical thresholds were used, dividing the continuous variables into no more than two categories. p-Values of <0.05 were considered to indicate statistical significance. The survival data were obtained from hospital records or from the city registry system. The SPSS software program (ver. 23.0; IBM Corp., Armonk, NY, USA) was used to perform all the statistical analyses.
This study was approved by the Institutional Review Board (IRB) of the Yokohama City University (IRB Number: B160707003) and Kanagawa Cancer Center (2016.epidemiologic study-22).
Results
Clinicopathological features. A flow diagram of the selection process is shown in Figure 1. We evaluated 696 patients in the present study, including 122 patients with stage II or III Borrmann type IV gastric cancer who underwent curative resection and 574 patients with other types of gastric cancer.
Table I summarizes the clinicopathological data of the patients with Borrmann type IV gastric cancer and other types of cancer. There were significant differences in the distribution of age, gender, body mass index, surgical method, tumor size, histological types, pathological T factor and adjuvant chemotherapy between the two groups. The Borrmann type IV cases tended to be younger, more often female and had a lower body mass index than the other cases. Regarding the treatment method, total gastrectomy was performed frequently, but there were a few cases in which adjuvant chemotherapy was given for the Borrmann type IV group. The size of the tumor was larger, depth of cancer invasion deeper and lesions more poorly differentiated in the Borrmann type IV group than in the other types.
Long-term outcomes. During a median follow-up of 36 months, the 5-years RFS rate in patients with Borrmann type IV and other types of cancer was 25.3% and 63.8% (Figure 2), respectively, and the 5-years OS rate was 28.4% and 70.5% (Figure 3), respectively (p<0.001). In patients with Borrmann type IV gastric cancer, the median survival was 21 months. The 5-year OS rate was influenced by the tumor size, depth of invasion, lymph node metastasis, locations of lesion, CY and intraoperative blood loss (Table II). A significant survival benefit was noted for an intraoperative blood loss of <400 ml, with a 5-year RFS rate of 2.1% compared to patients who lost ≥400 ml (0%, p<0.001) (Figure 4). The 5-year OS was 34.9% for <400 ml and 16.3% for ≥400 ml of blood loss (p<0.001) (Figure 5). Six factors that were significant in the univariate analysis were included in the multivariate analysis, which indicated that survival was independently influenced by intraoperative blood loss and CY positivity (Table II).
Univariate and multivariate Cox proportional hazards analyses of the clinicopathological factors associated with overall survival in Type IV gastric cancer.
Discussion
Since the Borrmann classification system was developed in 1926, it has been generally accepted and widely adopted. However, despite advances in diagnostic methods, Borrmann type IV gastric cancer is still detected at an advanced stage, and survival rates for these patients remain poor (15, 16). Some retrospective studies reported that the 5-year OS of patients with Borrmann type IV gastric cancer was only 10.5% to 16.7% (12, 17, 18). In our study, the 5-year RFS rate in patients with Borrmann type IV disease was 25.3%, while the 5-year OS rate was 28.4%. In previous studies, Borrmann type IV gastric cancer was reported to have characteristic features, such as a young female prominence, advanced stage of detection, high frequency of peritoneal recurrence and low rate of curative resection compared to other types (12, 19-21). In this study, the age at diagnosis tended to be younger, female gender more frequent and detection made at a more advanced stage in cases of Borrmann type IV gastric cancer than in other cases.

Relapse-free survival in the low and high intraoperative blood loss groups.
The present study examined the clinicopathological parameters in Borrmann type IV gastric cancer and identified six significant risk factors affecting the long-term survival, and CY positivity and intraoperative blood loss were independent risk factors according to the multivariate analysis. In Borrmann type IV gastric cancer, previous studies have reported an early diagnosis and prompt treatment as crucial for improving prognosis. Zhu et al. (12) reported that the independent prognostic factors were lymph node metastasis and radical resection, and Yook et al. (22) found in their univariate analysis that the prognostic factors affecting the survival rate following curative resection were the location, occupied area and depth of the primary tumor along with the presence of lymph node metastasis and also the tumor stage. The early detection and radical resection have been reported to be essential for improving the prognosis of patients with Borrmann type IV gastric cancer.
Intraoperative blood loss has been reported to be associated with the prognosis of digestive carcinoma (23, 24). In hepatocellular carcinomas, Katz et al. (23) reported that increased intraoperative blood loss during hepatic resection is an independent prognostic factor for tumor recurrence and death. In pancreatic cancers, Nagai et al. (24) reported that intraoperative blood loss was a prognostic determinant of survival after surgery for pancreatic cancer and that operative blood loss could be used to stratify risk for pancreatic cancer mortality. There have also been reports that suggest that minimizing intraoperative blood loss is very important for ensuring a good outcome, although it was not found to be an independent prognostic factor for cancer patients (25, 26). Several papers describe the correlation of intraoperative blood loss and prognosis in cases of gastric cancer. Yue-Xiang Liang et al. (27) reported that intraoperative blood loss was an independent prognostic factor for gastric cancer after curative resection. Reducing intraoperative blood loss can improve the long-term outcome of gastric cancer patients following curative gastrectomy. Ito et al. (28) also reported that intraoperative blood loss adversely influenced the long-term outcomes of patients with stage II/III gastric cancer. However, no reports have described the correlation of intraoperative blood loss with the prognosis of Borrmann type IV gastric cancer. In the present study, the survival was independently influenced by intraoperative blood loss and the presence of CY in patients with Borrmann type IV gastric cancer.
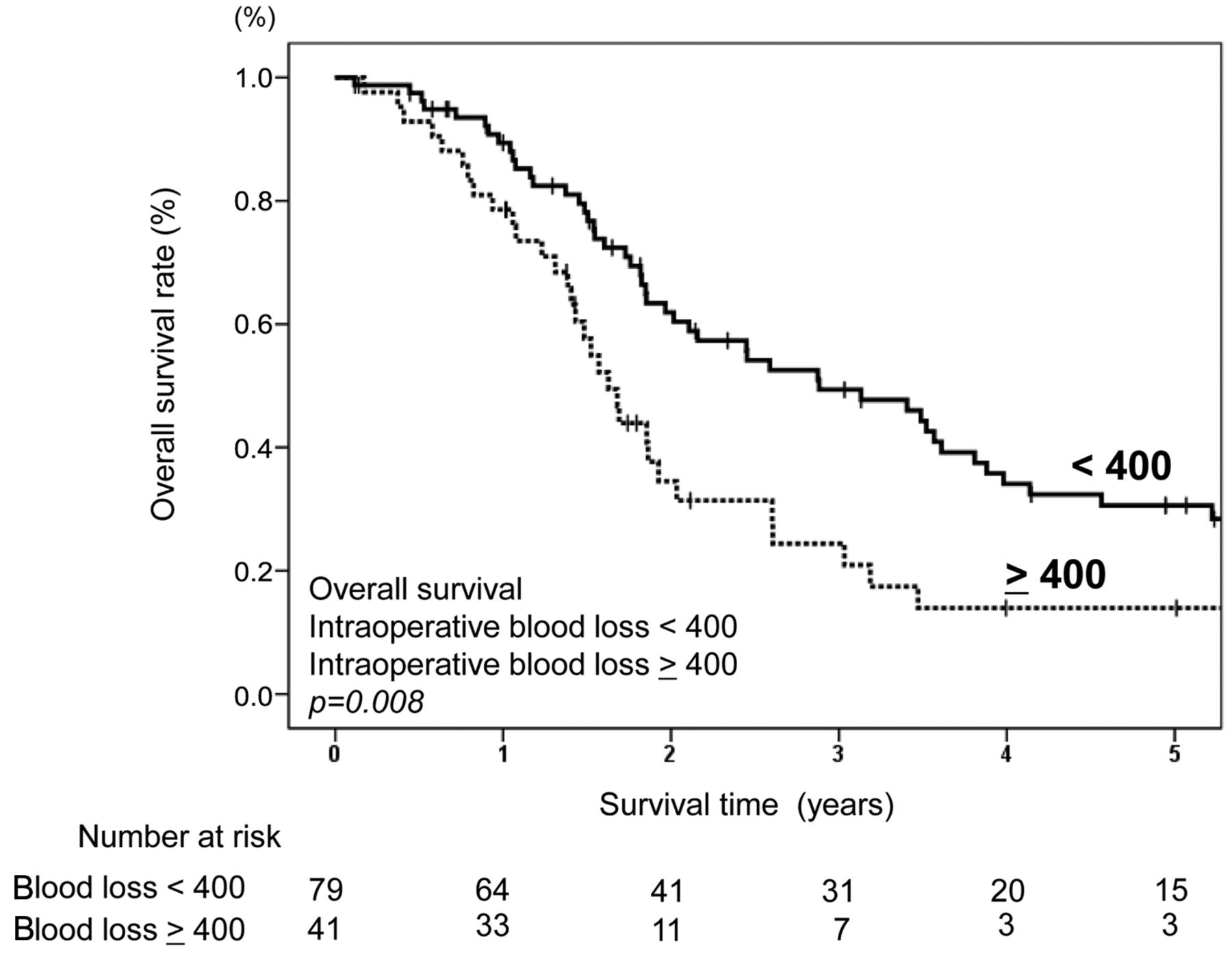
Overall survival in the low and high intraoperative blood loss groups.
Several limitations associated with the present study warrant mention. First, this was a retrospective study with a relatively small sample size, so a large-scale prospective validation study is needed. Second, the present study did not use a uniform cut-off value for intraoperative blood loss. Therefore, different statistical methods may obtain different values. Third, the use of different postoperative therapies might have introduced a confounding result.
In conclusion, this study of a multicenter database showed that intraoperative blood loss was an independent prognostic factor for Borrmann type IV gastric cancer after curative resection. Reducing the intraoperative blood loss may improve the prognosis of Borrmann type IV gastric cancer.
Footnotes
↵* These Authors contributed equally to this study.
Authors' Contributions
HT and TA made substantial contributions to conception and design. HT, TA, KK (Kazuki Kano), MN, YA, KH, KK2 (Keisuke Kazama), KK3 (Keisuke Koumori), MM1 (Masaaki Murakawa), IH, YM, TY1 (Takanobu Yamada), NY, TY2 (Takaki Yoshikawa), MM (Munetaka Masuda), TO, and YR made substantial contributions to acquisition of data, or analysis and interpretation of data. TA, KK, YA, HT, AT, KK2 and YR have been involved in drafting the manuscript or revising it critically for important intellectual content. TA, YM, KK3, KH, MM, MN, TO, and MM have given final approval of the version to be published. Each Author participated sufficiently in the work to take public responsibility for appropriate portions of the content, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All Authors read and approved the final manuscript.
Conflicts of Interest
The Authors declare that they have no competing interests related to this study.
- Received November 29, 2019.
- Revision received December 4, 2019.
- Accepted December 6, 2019.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}