


Abstract
Background/Aim: Cancer immune therapy by immune checkpoint inhibitors (ICIs) is a promising therapeutic strategy for various cancer types. Among ICIs, anti-programmed cell death protein-1 (PD1) and anti-programmed death-ligand 1 (PD-L1) antibodies have shown a remarkable clinical benefit. The present study aimed to address the functional and clinical significance of serum levels of soluble PD-L1 (sPD-L1) in patients. Materials and Methods: A total of 21 patients, 11 with NSCLC, nine with gastric cancer and one with bladder cancer, who underwent anti-PD-1 therapy were evaluated for sPD-L1 concentration by ELISA analyses at diagnosis and after treatment. Results: Pretreatment levels of sPD-L1 in patients who received ICIs were not remarkably correlated with the overall survival of these patients (r=0.3394, p=0.1323). Reduction of plasma sPD-L1 level was significantly correlated with tumor regression in patients administered four cycles of treatment (p<0.05). Conclusion: sPD-L1 might be derived and secreted from tumors and might be useful to identify primary responders to ICIs at a relatively early treatment timepoint.
Programmed death protein (PD1) and its ligand PD-L1 are central components in immune suppression, comprising the so-called ‘immune checkpoint’ (1, 2). Accumulating evidence revealed that the PD1/PD-L1 pathway is closely involved in resistance to antitumor immunity in multiple cancer types. Therefore, targeting immune checkpoints using immune checkpoint inhibitors (ICIs), such as those against PD1/PD-L1, has contributed to recent advances in cancer therapeutics (3, 4). However, many patients failed to respond or developed resistance after an initial response to ICIs. Predictive biomarkers for identifying potential responders to ICIs are currently under debate (5). Notably, several lines of evidence suggest a correlation between tumor PD-L1 expression and response to ICIs in variable malignancies including lung adenocarcinoma, melanoma, refractory Hodgkin's lymphoma, and other solid tumor types (6-10). Intriguingly, such correlation was reported for the expression level of membrane-bound PD-L1 (mPD-L1) on tumor tissues and plasma level of soluble PD-L1 (sPD-L1) in the blood of patients with cancer, highlighting the importance of their prognostic value. Several studies showed that high expression of sPD-L1 was associated with a poor prognosis in multiple types of malignant tumor. This suggests that sPD-L1 might be a predictive marker for low treatment responses to conventional chemotherapy and patients with high expression of sPD-L1 might be suitable for ICI therapy (11-20). However, it remains unclear whether the plasma sPD-L1 level is derived from malignant tumors pre-existing in patients and reflects a potential response to ICIs. Here, we measured the plasma level of sPD-L1 collected from patients with non-small cell lung cancer (NSCLC) and those with gastric cancer who underwent anti-PD1 therapy and analyzed change in sPD-L1 expression from diagnosis to after treatment in order to address the clinical implications of measuring sPD-L1 in patients.
Patients and Methods
General information. We retrospectively analyzed data for 21 patients, 11 with first-line or previously treated NSCLC, nine with gastric cancer and one with bladder cancer, who received ICI treatment (240 mg nivolumab intravenously every 2 weeks, or 200 mg pembrolizumab intravenously every 3 weeks) at Showa University Hospital from January 2017 to April 2019. The patient characteristics, immunohistochemical assessment of PD-L1 in the tumor at the time of diagnosis, serum sPD-L1 concentration at the time of diagnosis and after 1-4 cycles of ICI treatment were evaluated. Relative change in sPD-L1 concentration was determined by dividing the sPD-L1 concentration after four cycles of ICI treatment by that at diagnosis. Overall survival (OS) referred to the time from diagnosis to the date of last follow-up or mortality. The efficacy of ICIs was assessed according to the Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1 (21). Target lesions were assessed by computed tomography, and change in tumor size was defined as the percentage change in the tumor size from baseline to that after four cycles of ICI treatment. The control group for sPD-L1 consisted of samples collected from five healthy volunteers. The Ethics Committee of Showa University Hospital approved the study. All patients who participated in this research provided informed consent in participation.
PD-L1 determination. Formalin-fixed paraffin-embedded tissue samples were prepared from biopsy tissues of the patients before treatment. Immunohistochemical staining of mPD-L1 was performed by companion diagnostics according to the manufacturer's instructions: PD-L1 immunohistochemistry (IHC) 28-8 PharmaDX and PD-L1 IHC 22C3 PharmaDX were used before treatment with nivolumab and pembrolizumab (Dako, Glostrup, Denmark). Two investigators were blinded to the corresponding clinical outcome and independently evaluated specimens stained as serial sections. PD-L1 expression was quantitatively evaluated as tumor proportion score (TPS) according to the manufacturer's instructions.
Blood samples were collected before and after treatment, and the plasma levels of sPD-L1 were measured by enzyme-linked immunosorbent assay (ELISA) (DuoSet ELISA Development System Human PD-L1/B7-H1 and DuoSet Ancillary Reagent Kit 2; R&D Systems, Inc., Minneapolis, MN, USA), according to the manufacturer's instructions. Standards and samples were prepared as follows. Recombinant human B7-H1 was diluted with 1% Bovine serum albumin (BSA) in phosphate-buffered salts (PBS) for standards. Plasma was centrifuged and the supernatants were diluted 1:4 with 1% BSA as samples. A flat-bottom 96-well microplate was coated with 4.0 μg/ml mouse anti-human B7-H1 capture antibody in PBS, and the plate was sealed with an adhesive strip followed by overnight incubation. Thereafter, the plate was washed and blocked with 1% BSA in PBS for 1 hour. After washing, standards or samples were added to each well and the plate was sealed. Two hours after incubation, the plate was washed and then 50 ng/ml biotinylated goat anti-human B7-H1 detection antibody in PBS containing 1% BSA and 2.5% goat normal serum (R&D Systems) was placed in each well. The plate was sealed and incubated for a further 2 hours. After washing, for colorimetric detection, streptavidin-horseradish peroxidase (1:200) was added to each well which was sealed and then incubated for 20 minutes avoiding direct light. After the plate was washed, a substrate solution consisting of a 1:1 mixture of H2O2 and tetramethylbenzidine was placed in each well and incubated for 20 minutes in a dark room. A termination solution was then added and the absorbance of each well was measured using a microplate reader (wavelength, 450 and 570 nm; Powerscan HT; DS Pharma Biomedical Co., Ltd., Osaka, Japan). The reading at 570 nm was subtracted from that at 455 nm to correct for optical imperfections in the plate. Concentrations of sPD-L1 were determined using a calibration curve. The minimum detectable concentration of sPD-L1 was 9.82 pg/ml.
Data analysis. Statistical analysis was performed using Microsoft Excel (Microsoft Co., Redmond, WA, USA) and validity of the results was confirmed by JMP version 14.0 (SAS Institute, Cary, NC, USA). Data were analyzed using the unpaired Student's t-test. The results are presented as the mean±standard deviation. Linear correlation analysis was performed using Spearman's rank correlation. The comparisons of patient variables and sPD-L1 levels according to pretreatment levels were performed using Fisher's exact test. All tests were two-sided, and a p-value of less than 0.05 was considered statistically significant.
Results
Pretreatment levels of sPD-L1 in association with different clinicopathological characteristics and clinical responses. To explore whether there is an association between plasma sPD-L1 concentration and clinicopathological characteristics, as well clinical responses, in patients on PD1 blockade therapy, we measured sPD-L1 concentrations at diagnosis and after four cycles of ICI treatment in plasma collected from 21 patients, 11 with NSCLC, nine with gastric cancer and one with bladder cancer. Four patients with NSCLC and nine with gastric cancer were treated with nivolumab; seven patients with NSCLC and 1 with bladder cancer were treated with pembrolizumab. The mean sPD-L1 level in the experimental group pre-ICI treatment was 469.7±298.8 pg/ml and was 323.0±108.4 pg/ml in the control group. In contrast, with previous reports (12, 14-16, 18-20), there was no significant difference between the groups (p=0.2969). We evaluated the potential association between pre-ICI treatment levels of sPD-L1 and clinicopathological characteristics in the patients. For this purpose, we divided patients into two groups according to the median sPD-L1 level: low sPD-L1 ≤347.37 pg/ml and high PD-L1 >347.37 pg/ml. As shown in Table I, no significant correlation was observed between sPD-L1 level and patient's sex, age cancer type and pathological stage.
Detection of mPD-L1 expression in tumors was approved as a companion diagnostic to predict a responder to PD1/PD-L1 blockade therapy. We assessed whether mPD-L1 expression, assessed by tumor IHC, routinely evaluated in 11 patients with NSCLC, was associated with sPD-L1 level. There was no significant correlation between mPD-L1 and sPD-L1 levels (r=0.1955, p=0.5645). Then whether expression of mPD-L1 and sPD-L1 pre ICI treatment correlated with patient outcome was assessed because a previous report showed mPD-L1 expression determined by tumor IHC was associated with a poor prognosis in various cancer types (22). Furthermore, pretreatment serum levels of sPD-L1 in patients who received conventional chemotherapy other than ICIs were positively correlated with a poorer prognosis (11-20). In contrast to these previous studies, mPD-L1 expression as well as pretreatment levels of sPD-L1 in patients who received ICIs were not significantly correlated with the OS of these patients (r=−0.1981, p=0.5592 and r=0.3394, p=0.1323, respectively). The clinicopathological characteristics including the sPD-L1 concentration as well as OS are summarized in Table II.
Association of clinical factors with plasma level of soluble programmed death-ligand 1 (sPD-L1). Patients were divided according to the median sPD-L1 level.
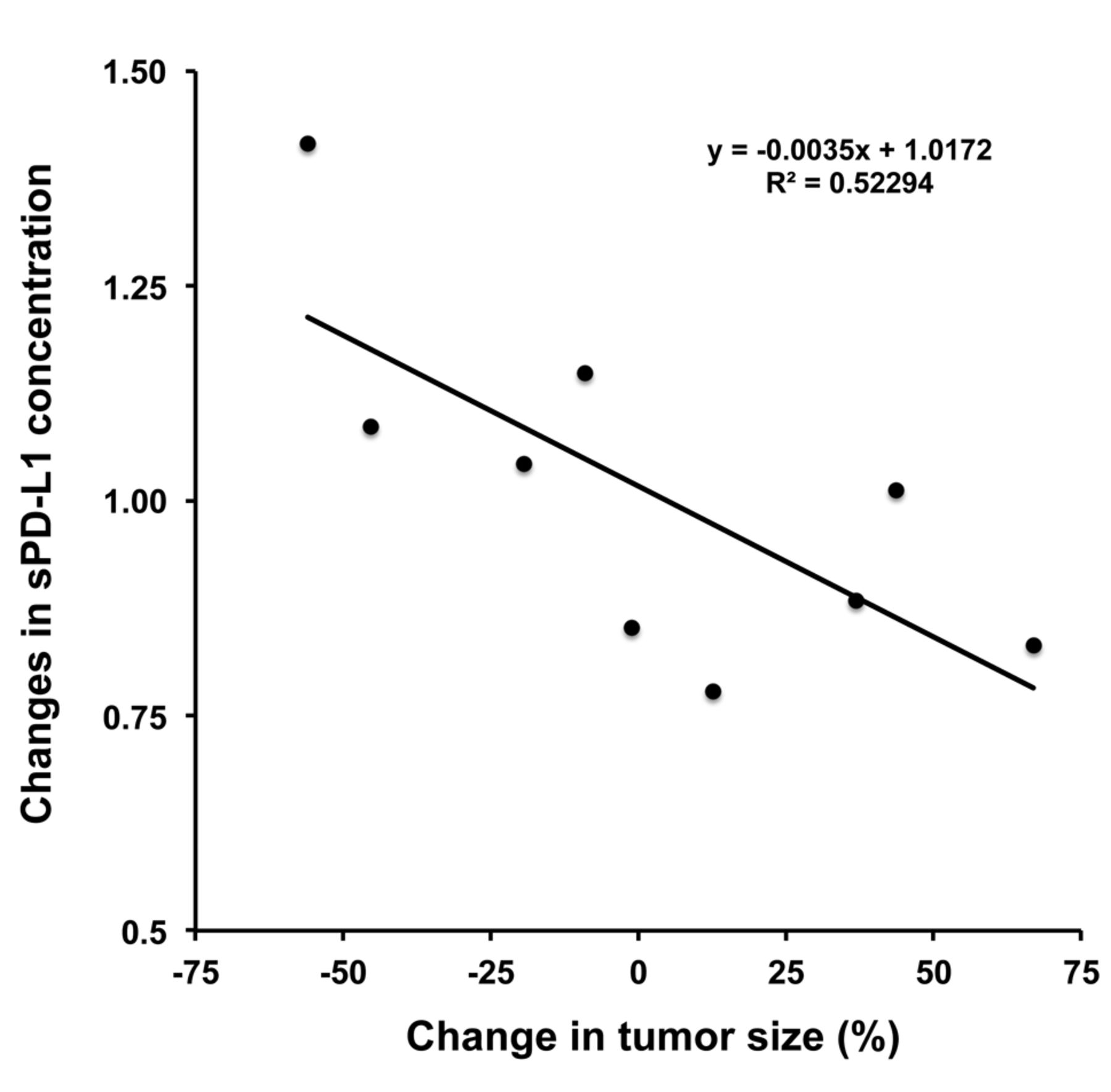
Association between sPD-L1 levels and tumor regression after four cycles of ICI treatment. Because the sPD-L1 levels pre-ICI treatment appeared to have no prognostic significance before PD1 blockade therapy, it prompted us to investigate whether a change in sPD-L1 level would be observed in response to ICI treatment. For this purpose, we calculated changes in sPD-L1 concentration from baseline to after four cycles of ICI treatment and evaluated its potential association with OS, mPD-L1 expression and percentage change of tumor size. Among 21 patients, data for nine were available who had been administered more than four cycles ICI treatment. Interestingly, the change in sPD-L1 concentration was significantly correlated with the percentage change of tumor size (r=0.7231, p=0.0277; Figure 1), but not with OS (r=−0.3211, p=0.3995) or mPD-L1 expression (r=0.4045, p=0.4262). In addition, as shown in Figure 2, the patients of this study that showed the greatest tumor regression and progression in response to ICIs, case 3 and case 14, respectively (Figure 2A), had similar levels of sPD-L1 in response to four cycles of ICI, but remarkably different levels pre-ICI therapy (Figure 2B). Table II summarizes the clinicopathological characteristics including the change of plasma sPD-L1 concentration from pre to post ICI treatment (four cycles), as well as the OS of nine patients for whom sPD-L1 levels at post four cycles of ICI were available.

Linear correlation between change in serum level of soluble programmed death-ligand 1 (sPD-L1) and tumor regression. Relative change in serum sPD-L1 was calculated as the concentration after four cycles of immune checkpoint inhibitor therapy divided by that by that at diagnosis. Percentage change in the tumor size after four cycles of ICI treatment was calculated relative to that at baseline. A decrease in sPD-L1 concentration from pre to post immune checkpoint inhibitor treatment was significantly correlated with reduction of tumor size (r=0.7231, p=0.0277).
Discussion
Recently, the presence of mPD-L1 expression in tumors has been used clinically to predict ICI responders: Clones 28-8, 22C3 and SP142 have been approved as companion diagnostic antibodies for nivolumab, pembrolizumab and atezolizumab, respectively (23). However, not all patients who present with high levels of mPD-L1 expression respond to ICI treatment, and therefore attempts to establish new companion diagnostic biomarkers using liquid biopsy are underway (24). In line with this, increasing numbers of studies have suggested that the plasma level of sPD-L1 expression is associated with tumor aggressiveness and shorter patient survival, and thus might be a predictive biomarker to identify ICI responders (11-20). To date, it is still unclear whether ICI treatment-dependent fluctuations of sPD1 level occur during treatment cycles. In this study, we demonstrated, for the first time, that reduction of sPD-L1 level after four cycles of ICI treatment did not correlate with OS, but significantly correlated with tumor regression in patients with NSCLC and gastric cancer. This result indicated that the sPD-L1 level might reflect the total active cancer cells in an individual, and therefore might be linked to the size of lesions evaluable for ICI response. Notably, these observations might address one of the unresolved questions of where sPD-L1 is derived from. Although treatment associated-tumor disruption should increase tumor-derived PD-L1, including mPD-L1, we observed that sPD-L1 significantly decreased in association with regression of the tumor. Thus, we presumed that sPD-L1 might not be derived from tumors disrupted by ICI treatment but mainly secreted from viable tumors. Our notion is supported by previous reports showing that sPD-L1 levels in patients with lymphoma were reduced by treatment with conventional chemotherapeutic agents (18, 19). Furthermore, it was reported that a secreted form of PD-L1 derived from alternative splicing might be involved in therapeutic resistance to ICIs in malignant melanoma (25). Notedly, Gong et al. identified other forms of sPD-L1 splice variants that might act as decoys, resulting in resistance to PD-L1 blockade therapy. In addition, levels of sPD-L1 in patients harboring sPD-L1 splice variants were much higher than in healthy controls and patients without sPD-L1 splice variants (26). Taken together with our finding, this shows that sPD-L1, to which resistance to ICIs such as anti-PD-L1 is attributed, might be secreted by tumors and therefore might be a useful marker when combined with RECIST for estimating the volume of viable cancer in patients. In addition, patients whose levels of sPD-L1 decreased after four cycles of ICI treatment might be primary responders for ICI therapy irrespective of their OS. However, in conflict with several previous reports (12, 14-16, 18-20), there was no significant difference in sPD-L1 levels between healthy volunteers and patients with regard to our experimental settings. This conflict might be causally related to antibody specificity, especially when detecting sPD-L1 splice variants. However, the functional role as well as clinicopathological significance of the secreted sPD-L1 splice variants is still enigmatic. Further improvements to the detection system to distinguish between sPD-L1 variants are needed.

Changes in tumor size and serum level of soluble programmed death-ligand 1 (sPD-L1) level during treatment. A: Representative computed tomographic images of cases 3 (greatest tumor regression) and 14 greatest tumor progression) at baseline (upper panel) and after four cycles of treatment with immune checkpoint inhibitor (lower panel). White arrows indicate measurable and assessable lesions. Bars=5 cm. B: sPD-L1 concentration before and during immune checkpoint inhibitor treatment. Case 3 was treated with nivolumab and case 14 was treated with pembrolizumab.
Clinicopathological features, plasma soluble programmed death-ligand 1 (sPD-L1) concentration, tumor regression and overall survival (OS) for all study patients.
In summary, although our study had a low sample size, a significant correlation between a reduction of sPD-L1 levels and tumor regression was observed after four cycles of ICI treatment in patients with NSCLC and gastric cancer. Therefore, our data suggest that sPD-L1 might be secreted from tumors and be useful for evaluating primary responders to ICIs at a relatively early time point during treatment cycles. Importantly, our samples were collected from patients administered PD1 blockade agents, nivolumab and pembrolizumab. However, it is still unknown how the use of PD-L1 blockade agents affects the PD-L1 level. New insights might be provided regarding the clinical significance of determining the sPD-L1 level to investigate whether there is a differential effect on sPD-L1 level arising from use of anti-PD1 or anti-PD-L1 agents.
Acknowledgements
The Authors thank Edanz Group (www.edanzediting.com/ac) for editing a draft of this article.
Footnotes
↵* These Authors contributed equally to this study.
Authors' Contributions
KH and SW conceived and designed this study. KH, RO, MS, RO, YK, HM, TI, YH, HA, TA and SW collected samples and recorded the general data and the observation indicators of patients. MW performed all ELISAs. KA analyzed the data and wrote the first draft of the article. JT, KY, TT, SK and SW critically reviewed and corrected the article. All Authors reviewed and approved the final version of the article.
Conflicts of Interest
None of the Authors declares any conflict of interest.
- Received July 15, 2019.
- Revision received July 28, 2019.
- Accepted July 30, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Nivolumab for the Treatment of Advanced Pediatric Malignancies
- Soluble PD-L1 is associated with local and systemic inflammation markers in primary and secondary brain tumours
- Therapeutic plasma exchange clears circulating soluble PD-L1 and PD-L1-positive extracellular vesicles
- Two Malignancies With Differential Responses to Immune Checkpoint Inhibitors: A Case Report
- Clinicopathological and Prognostic Significance of Programmed Death Ligand 1 Expression in Korean Patients With Triple-negative Breast Carcinoma