


Abstract
Aim: To assess the patterns of disease progression in advanced/metastatic epidermal growth factor receptor (EGFR)-mutant non-small-cell lung cancer (NSCLC) on first-line treatment with erlotinib and identify potential prognostic factors for progression-free survival (PFS). Patients and Methods: Patients with stage IIIB/IV EGFR-mutation-positive NSCLC receiving first-line erlotinib were followed-up until 24 months after the last patient was enrolled or until premature withdrawal for any cause. Results: A total of 127 evaluable patients were enrolled. The median PFS and overall survival were 8.8 and 19.1 months, respectively. Disease progression was asymptomatic in 57.6% of patients and 53.3% developed new sites of metastasis. The presence of liver metastasis was identified as an independent prognostic factor for poor PFS. Conclusion: Metastatic progression with asymptomatic disease seems to be the predominant pattern of disease progression on first-line erlotinib in real-life practice in patients with advanced/metastatic EGFR-mutant NSCLC. Additionally, the presence of liver metastases may negatively affect PFS in these patients.
- Epidermal growth factor receptor
- EGFR
- tyrosine kinase inhibitors
- TKIs
- erlotinib
- non-small-cell lung cancer
- NSCLC
- progression patterns
- re-biopsy
Non-small-cell lung cancer (NSCLC), accounting for more than 85% of lung cancer cases, is the leading cause of cancer-related death worldwide (1). Most patients with NSCLC present with locally advanced or metastatic disease at initial diagnosis (1). The standard first-line treatment has traditionally consisted of platinum-based combination chemotherapy, but unfortunately, it provides a modest overall survival (OS) benefit (2-4).
Increased knowledge of the molecular biology of lung cancer has shifted the treatment paradigm towards individualized therapy based on molecular characterization of the tumor. Accordingly, epidermal growth factor receptor (EGFR) has become an important molecular target in NSCLC, and has led to the development of tyrosine kinase inhibitors (TKIs) such as gefitinib, erlotinib, afatinib, and the third-generation TKI osimertinib. The presence of EGFR-activating mutations has been associated with a superior clinical benefit of EGFR-TKIs in patients with advanced NSCLC (5-8). Compared to standard first-line platinum-based chemotherapy, treatment with EGFR-TKIs has shown a significantly improved clinical outcome in patients harboring activating mutations in exons 18-21 which encode the tyrosine-kinase domain of the EGFR gene (5-10). EGFR-TKI therapy has, therefore, emerged as the standard of care in the first-line setting for patients with NSCLC and EGFR-activating mutations.
However, despite the striking initial response and the significant survival benefit obtained with EGFR-TKIs, most patients treated with these targeted agents eventually develop local progression or distant metastases (11, 12). Acquired resistance to EGFR-TKIs typically occurs in most patients within a 10- to 14-month period (5-7, 9, 13, 14). Acquired EGFR T790M mutation in exon 20 is responsible for resistance in up to 60% of patients treated with EGFR-TKIs (15). However, other mechanisms have been identified to account for resistance, including target gene alteration (i.e. EGFR amplification); MET proto-oncogene, receptor tyrosine kinase (MET) or human epidermal receptor 2 (HER2) amplification; B-Raf proto-oncogene, serine/threonine kinase (BRAF) or phosphatidylinositide 3-kinase (PI3K) mutation; and phenotypic transformation (16). Updated data on tumor characteristics after development of clinical resistance should, therefore, be used for clinical decision making. Thus, re-biopsy on disease progression is now recommended as routine practice in current clinical practice guidelines, including those of the European Society for Medical Oncology (17).
Discontinuation of EGFR-TKIs and a switch to chemotherapy is a common strategy used when progressive disease (PD) occurs during treatment with EGFR-TKIs. However, due to the better tolerability of EGFR-TKIs compared with cytotoxic chemotherapy agents, continuing EGFR-TKI therapy beyond radiological PD has emerged as an adequate strategy for patients with EGFR-mutated NSCLC (14). Indeed, discontinuing treatment with EGFR-TKIs after disease progression may result in accelerated tumor growth and worsening of lung cancer-related symptoms, a phenomenon known as ‘disease flare’ (18).
There is growing evidence to suggest that continuing EGFR-TKIs beyond disease progression might provide a survival benefit (19) even after the development of resistance, especially in patients who are asymptomatic at the time of progression (20). Indeed, second-line treatment selection for patients with EGFR-activating mutations who progress on anti-EGFR therapy depends not only on their T790M mutation status, but also on the pattern of progression, including location (single versus multiple sites) and the presence of cancer-related symptoms (asymptomatic or symptomatic) (21). However, data about progression patterns in patients with EGFR-mutant NSCLC are limited and in particular, the characterization of patterns and prognostic factors of disease progression on erlotinib in these patients is lacking.
The present study was conducted to investigate the patterns of disease progression in patients with advanced or metastatic EGFR-mutated NSCLC on first-line erlotinib and identify potential clinical and molecular characteristics that may affect progression-free survival (PFS) in these patients. Secondarily, this study also addressed the clinical outcome of first-line erlotinib treatment and the feasibility of re-biopsy after disease progression on erlotinib.
Patients and Methods
Study design and patients. The ASPET study was a multicenter, prospective, observational study conducted at 43 hospitals throughout Spain. The study was approved by the Ethics Committee of Miguel Servet Hospital (Zaragoza, Spain) (approval number: 10/2012), and written informed consent was obtained from all patients before they were included in the study. The study was carried out in accordance with the Declaration of Helsinki and applicable regulatory requirements.
Patients with histologically or cytologically confirmed advanced or metastatic (stage IIIB/IV) NSCLC with confirmed EGFR-activating mutations (mutations in the exons 18-21 of the EGFR gene) receiving erlotinib monotherapy as first-line treatment for advanced or metastatic disease according to routine clinical practice were eligible to be included in the study. Patients were excluded if they had received prior systemic chemotherapy for advanced or metastatic disease. However, the previous use of neoadjuvant or adjuvant chemotherapy was permitted as long as it had been completed more than 6 months before initiation of erlotinib treatment. Patients who had received radiotherapy within 14 days prior to starting erlotinib were also excluded.
Eligible patients were prospectively followed-up until 24 months from the inclusion of the last patient in the study or until premature withdrawal for any cause including death, whichever came first, in order to characterize their clinical management and outcome. Study visits were performed every 2 months during erlotinib treatment according to routine clinical practice. After completion or discontinuation of erlotinib, patients were followed-up every 3 months for evaluation of clinical outcome until death or study completion (24 months after the inclusion of the last patient), whichever was earlier.
Tumor response was evaluated according to local clinical practice and using version 1.1 of the Response Evaluation Criteria in Solid Tumors (RECIST) during erlotinib treatment (22). It was subsequently assessed at the follow-up visits after treatment completion (every 3 months). Patients were evaluated for toxicity during erlotinib treatment and for 30 days after the last administration of erlotinib.
Statistical analysis. The primary study endpoint was the description of disease progression patterns and the association of clinical and molecular characteristics with PFS after erlotinib treatment initiation.
Disease progression patterns were characterized on the basis of the presence of cancer-related symptoms (symptomatic or asymptomatic) and location of progression as follows: i) Local progression: defined as an increase in the size of a pre-existing tumor lesion; ii) metastatic disease: at least one new lesion; iii) general progression: defined as an increase in tumor size of two or more tumor lesions that either initially responded to or progressed on erlotinib treatment.
Secondary endpoints included the objective response rate (ORR) according to RECIST criteria, OS and 1-year survival, and the safety profile of erlotinib treatment based on the incidence of adverse events (AEs) which were graded according to the National Cancer Institute Common Toxicity Criteria (NCI-CTC) version 4.0 (23). The feasibility of performing re-biopsy of the tumor in routine clinical practice was also evaluated as a secondary endpoint on the basis of physician responses to a questionnaire containing five items. Patient attitudes to biopsy and potential re-biopsy were also assessed through their responses to a 5-item questionnaire.
A descriptive statistical analysis was performed on the study variables including calculation of measures of central tendency and dispersion (mean±standard deviation, median and interquartile range) for quantitative variables, and frequencies and valid percentages for qualitative variables.
The efficacy analyses were performed on all patients who met the selection criteria and who started erlotinib treatment within 1 month prior to study initiation. PFS was calculated as the time elapsed from erlotinib treatment initiation until disease progression or death from any cause. OS was assessed from erlotinib initiation to death. Time to progression (TTP) was defined as the period of time between the start of erlotinib treatment and the date of disease progression or death due to progression, whichever occurred first. The probabilities of PFS, TTP and OS were estimated using the Kaplan–Meier method.
The following variables were assessed as potential factors associated with PFS by bivariate COX regression analyses: age (≤65 vs. >65 years), gender, baseline Eastern Cooperative Oncology Group performance status (ECOG PS) (0 vs. 1 and vs. 2-3; 1 vs. 2-3), smoking habit (never smoked vs. current smoker and vs. former smoker), EGFR mutations in exon 19 and exon 21 (yes vs. no), location of metastases (lung, pleura, central nervous system, lymph nodes, bone, adrenal gland, liver, other) (yes vs. no). Variables with associations of p<0.2 were analyzed in a multivariate COX regression model with stepwise selection to determine independent prognostic factors for PFS. Hazard ratios (24) and 95% confidence intervaIs (CIs) were calculated.
All patients who had received at least one dose of the study regimen were included in the safety analysis. Toxicities were graded according to NCI-CTCAE (version 4.0).
The statistical analysis was performed using SAS statistical analysis software version 9 (SAS Institute Inc., Cary, NC, USA).
Results
Patients. From January 2014 to June 2017, a total of 144 patients were enrolled in the study. Seventeen patients were excluded either for not fulfilling the inclusion criteria (n=14), because they did not receive erlotinib (n=1), or due to the fact that they had been receiving erlotinib treatment for at least 1 month prior to study initiation (n=2). Therefore, a total of 127 patients were evaluable for efficacy and 143 patients for safety analyses.
The demographic and clinical characteristics of the evaluable patients are shown in Table I. Briefly, approximately half of the patients were over 65 years of age, 97% were Caucasian, 65% were female, and about 65% had never smoked. The most common histological type was adenocarcinoma (93%). ECOG PS was 0 or 1 in 71% of patients at study initiation. Most patients (95.3%) had stage IV disease at diagnosis, involving three or more metastatic sites in about half of patients (48%). Metastases were mainly located in the lungs (72.4%) and were treated with radiotherapy in 28 (22.1%) patients.
Patient demographics and clinical characteristics (n=127).
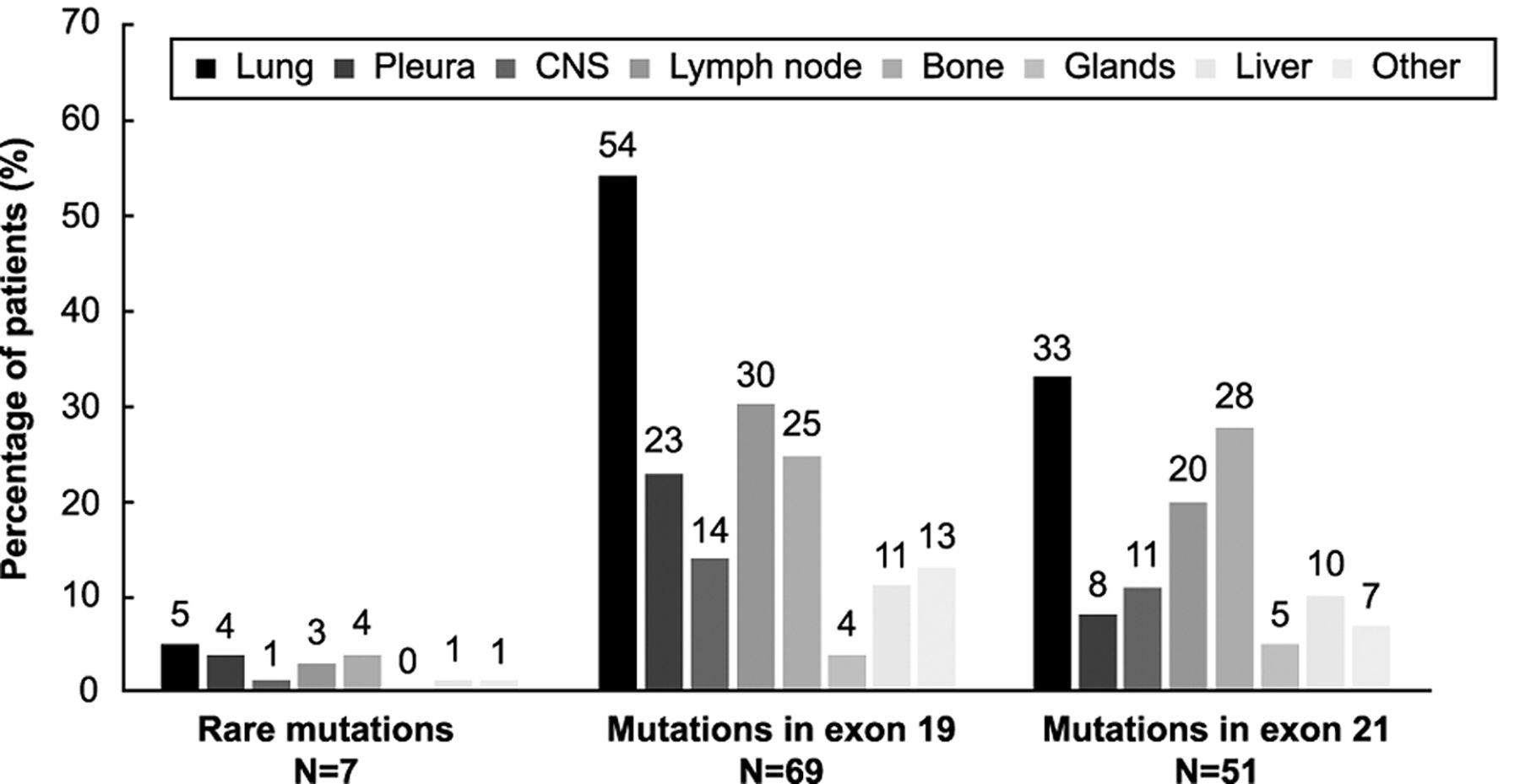
Location of metastases according to the type of epidermal growth factor receptor (EGFR)-activating mutation (mutations in exons 19 and 21, and rare mutations). CNS: Central nervous system.
Regarding EGFR mutational status, 69 (54.3%) patients had exon 19 deletions and 51 (40.2%) had exon 21 L858R point mutation. Rare mutations, defined as those present in exons 18 and 20 were found in seven (5.5%) patients. EGFR mutations in exons 19 and 21 were more frequently found in those patients with metastases located in the lungs, lymph nodes, and bone (>20% of patients) (Figure 1).
Study treatment. Dose adjustment of erlotinib was required in 38 (29.9%) patients. Out of all dose adjustments performed (n=54), 11 (8.6%) were due to skin toxicity while three (2.4%) dose reductions were caused by transaminase elevation. Temporary interruption of erlotinib treatment was needed in 43 (33.9%) patients. The most common reasons for erlotinib interruptions were skin toxicity (n=18; 20%), diarrhea (n=6; 4.6%), and transaminase elevation (n=3; 1.5%). Erlotinib treatment was interrupted due to erlotinib-related adverse events (AEs) in 12 (8.4%) patients. The median relative dose intensity for erlotinib (ratio of doses received to doses planned) was 1.0 (range=0.8-1.0).
The median duration of first-line treatment with erlotinib was 8.5 (range=4.1-15.9) months. The most common reasons for premature erlotinib discontinuation were disease progression in 76 (59.8%) patients, AEs in 15 (11.8%) patients, and death in 15 (11.8%). Discontinuation of erlotinib was due to investigator decision in five (3.9%) patients and patient's decision in three (2.4%). Erlotinib was discontinued due to losses to follow-up in two (1.6%) patients and because of other unspecified reasons in three (2.4%) patients. Seven (5.5%) patients completed the planned duration of erlotinib treatment according to routine clinical practice.
Efficacy. The ORR was 53.8% and the disease control rate was 83%. Of 119 evaluable patients, three (2.5%) showed a complete response and stable disease was reported in 35 (29.4%). The best confirmed response was partial response in 51.3% of patients (n=61).
The median duration of follow-up from study treatment initiation was 15.7 (range=7.8-27.2) months. The median PFS was 8.7 (95% CI=8.0-10.9) months (Figure 2A) and the median time to progression was 9.8 (95% CI=8.4-11.9) months (Figure 2B). The median OS was 19.1 (95% CI=14.7-20.8) months (Figure 2C). At the time of the analysis, 65 (76.5%) patients had died due to disease progression. Disease flare was only observed in three (2.54%) patients after discontinuing erlotinib treatment.
Safety. Overall, 136 (95.1%) patients suffered from AEs related to erlotinib. Fewer than one quarter of patients (n=34; 23.8%) experienced at least one grade 3 toxicity, with skin toxicity (10.5%) and diarrhea (4.2%) being the most common toxicities reported (in more than two patients). Grade 4 toxicities were detected in only three patients (skin toxicity, gastrointestinal toxicity, and decreased lymphocyte count in one patient each). Erlotinib-related AEs are summarized in Table II.
Nine serious AEs considered to be related to erlotinib were reported in 7 (5%) patients. The most frequent serious AE was grade 3 diarrhea in four patients. Grade 3 skin toxicity, asthenia, acute renal failure, and enteritis were reported in one patient each. Only one patient experienced a grade 4 serious AE (decreased lymphocyte count). None of the patients died due to a serious AEs related to erlotinib.

Kaplan–Meier curves for progression-free survival (A), time to progression (B), and overall survival (C). Patients were censored at the date of last available follow-up if still alive or without disease progression at the time of the analysis. When analyzing progression-free survival, those patients receiving a second-line treatment without disease progression on first-line erlotinib treatment were censored. CI: Confidence interval.
Erlotinib-related adverse events (n=143) according to National Cancer Institute Common Terminology Criteria for Adverse Events (23).
Patterns of disease progression. Disease progression occurred during erlotinib treatment in 82 (89.2%) patients. Three (3.3%) patients experienced disease progression during the follow-up period after discontinuing erlotinib treatment and before any subsequent systemic treatment was administered. Six (6.5%) patients had disease progression on second-line therapy initiated for reasons other than disease progression to first-line erlotinib treatment.
Disease progression was asymptomatic in 53 (57.6%) patients. In about half of the patients, disease progression was defined by the presence of at least one new metastatic lesion (n=49, 53.3%), while local progression was found in 15 (16.3%) patients. Local progression along with metastatic progression was reported in 27 (29.4%) patients.
Demographic and clinical factors associated with PFS. Among the sociodemographic and clinical variables, the presence of liver metastasis (p<0.001) was the only one significantly associated with PFS in the univariate analysis (Table III). Gender, age, ECOG PS, exon 19 deletion mutation, and the presence of metastases in lymph nodes and bone were also retained in the multivariate model (p<0.2). The multivariate analysis only identified the presence of liver metastasis (hazard ratio=2.043; 95% CI=1.251-3.336; p=0.004) as an independent prognostic factor for PFS. Patients with liver metastasis were more likely to have a shorter PFS.
Re-biopsy. A total of 35 (27.6%) patients underwent re-biopsy. Among those patients in whom biopsy was not repeated (n=83), investigator decision (n=35, 42.2%) was the most frequent reason for not performing re-biopsy, followed by patient's decision (n=5, 6%) and inaccessibility (n=5; 6%). Other non-specified reasons were reported in 38 (45.8%) patients.
Investigator attitudes to re-biopsy. Among the participating investigators (n=115), approximately 70% stated they would repeat biopsy for re-evaluation of mutational status at the time of disease progression. When physicians were asked about the second-line treatment-of-choice at the time of disease progression on EGFR-TKI therapy (questionnaire item 2), nearly half of the investigators (45.2%) would maintain erlotinib and would try to perform a re-biopsy to assess the mutational status. Discontinuation of erlotinib treatment and initiation of chemotherapy was stated as the strategy that would be adopted by nearly 34.8% of investigators. Overall, 11.3% of physicians said they would choose to add empiric chemotherapy to EGFR-TKI treatment after disease progression. Most investigators (80%) believed that re-biopsy would be technically feasible in terms of tumor tissue availability and sampling procedure (Table IV).
Patient attitudes to the first biopsy and potential re-biopsy. A total of 104 (82%) patients answered the questionnaire. Most patients considered that biopsy was bothersome or painful (63.5%). However, only seven (6.7%) patients stated they would refuse a repeat biopsy in the future (Table V).
Therapy after disease progression. Nearly 60% of patients (n=74) received EGFR-TKI therapy after disease progression. A total of 47 (37%) patients continued on erlotinib treatment. Thirteen (10%) patients received gefitinib and seven (5.5%) patients were treated with afatinib as second-line treatment. Osimertinib was used in seven (5.5%) patients. Overall, 30% of patients (n=37) received cisplatin or carboplatin-based chemotherapy after disease progression. Pemetrexed and platinum combination treatment was administered to 8% of patients (n=10). Radiotherapy was administered to 28 (22%) patients.
Discussion
The present study demonstrated that metastatic progression with the development of new sites of metastasis and asymptomatic disease are the predominant patterns of disease progression on first-line erlotinib in real-life practice in patients with advanced or metastatic NSCLC carrying EGFR-activating mutations. Our findings also highlight the feasibility of repeat biopsy on disease progression in order to determine the most appropriate subsequent treatment. In addition, our data suggest that the presence of liver metastasis seems to be an independent prognostic factor for PFS in these patients. This analysis also supports the benefit of first-line erlotinib in patients with advanced or metastatic EGFR-mutated NSCLC in a real-life setting.
Efficacy data obtained in the present study show that erlotinib is an active treatment in terms of tumor response and survival in patients with advanced EGFR mutation-positive NSCLC. As a descriptive comparison only, our efficacy results are in keeping with those previously reported in the EUTARC trial with erlotinib first-line treatment in European patients with EGFR mutation-positive NSCLC (7). Thus, the median PFS achieved in this study with erlotinib (8.8 months), although slightly shorter, was consistent with that described in the EUTARC trial with this targeted agent (9.7 months), wherein PFS with erlotinib was significantly longer than that observed with chemotherapy (5.2 months) (7). In addition, the median OS achieved with erlotinib in our series (19.1 months) was in line with the survival data described in the abovementioned trial with erlotinib (19.3 months), wherein no significant OS advantage was demonstrated compared with chemotherapy, probably due to the high crossover rate from chemotherapy to an EGFR-TKI, confounding the detection of any OS advantage. It is noteworthy that nearly 30% of patients were alive 36 months after erlotinib treatment initiation in our series. Additionally, the ORR of 54% was also comparable to that shown in the EUTARC trial with erlotinib (58%). Of note, despite the inclusion of approximately 6% of patients with mutations in exon 20 which are less sensitive to EGFR-TKIs (25), the clinical outcome data from this study are comparable to those reported in the EUTARC trial in which only patients with sensitizing mutations were included.
Univariate analysis of demographic and clinical characteristics associated with progression-free survival in patients treated with first-line erlotinib therapy.
Our findings suggest that erlotinib, administered as first-line treatment, is well tolerated in patients with advanced or metastatic NSCLC. Toxicity related to erlotinib was generally mild and manageable, and no treatment-related deaths were reported. Fewer than one quarter of patients experienced grade 3 toxicities and only three patients suffered from grade 4 toxicities. Safety findings are in line with phase III trials with erlotinib, with no new or unexpected safety signals observed (7, 8). In keeping with randomized trials using erlotinib, the most common grade 3 AEs were skin rash and diarrhea. Although erlotinib was temporarily interrupted in about 30% of patients, this was caused by erlotinib-related toxicity in fewer than 9% of patients. The high relative dose intensity for erlotinib treatment supports the tolerance of this regimen in a real clinical setting.
Results from physician questionnaire concerning re-biopsy (n=115).
Results from patient questionnaires regarding their attitude to biopsy and potential re-biopsy (n=104).
In line with previous evidence, the liver seems to be a less common site of metastasis than the brain and bone in patients with NSCLC harboring EGFR mutations (26). Our results suggest that the presence of liver metastasis is independently correlated with PFS, with a higher risk of shorter PFS in patients with liver metastases treated with erlotinib in the first-line setting. These findings are therefore in line with a previous report demonstrating a worse prognosis associated with liver metastasis (27), although the study was limited by a small number of patients with NSCLC with metastasis in the liver. Hepatic metastasis has also been shown to predict poor response to erlotinib as second- and third -line treatment in patients with stage IV lung adenocarcinoma (28). The worse prognosis associated with the presence of liver metastasis is probably explained due to more aggressive disease with liver metastasis usually being associated with additional distant metastases and a higher number of metastatic sites which typically predicts worse survival (29). Our findings suggest that management of liver metastases should therefore be a priority in patients with advanced EGFR-mutation-positive NSCLC for early detection of disease progression.
However, other factors which have been associated with prognosis in advanced NSCLC such as age, ECOG PS, and EGFR mutation status were not identified as factors predicting PFS in our study (29, 30). The lack of difference in PFS by age and performance status may suggest that both older patients (>65 years) and those with a poorer ECOG PS (2-3) may benefit from erlotinib treatment in the first-line setting. Additionally, in contrast with previous reports which have shown that a Del19 mutation is generally predictive of better efficacy than an L858R mutation (31), we found that the PFS benefit did not seem to differ between patients carrying exon 19 mutations and exon 21 mutations.
The predominant pattern of first progression on erlotinib was metastatic progression with development of new sites of metastases in half of patients followed by local progression along with metastatic progression in 30% of patients. Overall, fewer than 20% of patients had local progression alone. Our results therefore suggest that erlotinib might be more effective in preventing local progression than in avoiding the development of new metastases as has previously been reported with EGFR-TKIs in a retrospective study in Asian patients (32). Additionally, nearly 60% of patients progressed asymptomatically, in whom continuing EGFR-TKI therapy is recommended (20). Indeed, 60% of patients received an EGFR-TKI in the second-line setting, with 40% of patients continuing erlotinib treatment after disease progression.
After progression on EGFR-TKI therapy, a molecular analysis of resistance should be performed. In this regard, the feasibility of re-biopsy of patients with NSCLC at disease progression has already been demonstrated, as well as its potential benefit in the management of NSCLC and reassessing treatment options (33). Unfortunately, re-biopsy is not routinely used in clinical practice. Accordingly, we found that fewer than 30% of patients underwent re-biopsy on disease progression. However, when participating physicians were asked about their willingness to perform re-biopsy after disease progression, most of them (70%) answered that they would perform a repeat biopsy in order to evaluate the mutational status on disease progression. These discrepant findings may be due to local clinical practice and the fact that re-biopsy may have not been generally adopted as a part of routine clinical practice. In addition, this study began before the approval of osimertinib for patients with EGFR-mutated NSCLC whose disease progressed on EGFR-TKI therapy and who acquired resistance due to T790M. Therefore, the fact that re-biopsy to detect T790M mutation after PD was not performed at that time may explain the relatively low rate of re-biopsy on disease progression. However, the re-biopsy rate may have increased in recent years after the incorporation of osimertinib and may continue to rise in the future. In addition, it is possible that liquid biopsy was used as an alternative method to detect T790M mutation in those cases in which tissue biopsy was not feasible, and only when liquid biopsy showed a negative result for EGFR T790M mutation (34) was tissue biopsy performed for confirmation (17, 24). However, the fact that performance of liquid biopsy was not recorded in the study does not allow us to know whether the relatively low rate of re-biopsy is actually explained by the performance of liquid biopsy instead of re-biopsy on disease progression.
Nearly half the physicians affirmed that they would maintain EGFR-TKI therapy after disease progression, while switching to empiric chemotherapy would be the choice made by 35% of physicians according to the questionnaire findings. Accordingly, 60% of patients received an EGFR-TKI in the second-line setting, with 40% of patients continuing erlotinib therapy beyond disease progression. These findings suggest a common treatment strategy used in routine clinical practice. However, the conventional practice of discontinuation of EGFR-TKI and initiation of platinum-based chemotherapy remained the preferred approach for 30% of physicians despite the evidence on the feasibility and survival advantage of continuing EGFR-TKI therapy after PD compared to switching to chemotherapy (35). These findings can be explained due to the fact that osimertinib was not approved until 2016 and because there was limited and conflicting evidence outlining the clinical benefit of continuing an EGFR-TKI treatment at initial PD (35, 36). Therefore, guidelines at the time recommended a switch to platinum-based chemotherapy at the time of disease progression on EGFR-TKI therapy (37). Additionally, despite the limited effectiveness demonstrated by EGFR-TKIs used in combination with a cytotoxic drug after radiological PD (36), approximately 11% of physicians stated they would add empiric chemotherapy to the EGFR-TKI therapy. Nevertheless, most investigators affirmed that they may change their decision about the treatment to be used as second-line therapy based on the results of a re-biopsy.
Disease flare after EGFR-TKI therapy discontinuation is a concern in patients with EGFR-mutant NSCLC progressing on EGFR-TKI therapy. However, in this study the appearance of disease flare was lower than that previously reported (18, 36), probably due to the continuation of erlotinib treatment in around 40% of patients, while it might also be explained by the rapid initiation of subsequent therapy.
Although re-biopsy can be challenging in routine clinical practice due to limited tissue availability and the feasibility of the procedure, most investigators believed that re-biopsy would be technically feasible in terms of tumor tissue availability and sampling procedure. In addition, the majority of physicians assumed that the patient would be willing to undergo a repeat biopsy on disease progression. Indeed, although most patients considered that the biopsy at diagnosis was bothersome or painful, fewer than 7% of patients said they would refuse a repeat biopsy in the future.
Our findings, therefore, support the idea that re-biopsying the tumor for molecular testing at the time of progression is feasible and should become a routine procedure to guide therapeutic decision-making by physicians in a real-life setting. However, although the gold standard for the detection of resistance mechanisms is tissue re-biopsy, liquid biopsy is a useful and feasible technique when re-biopsy cannot be performed (34).
The main limitation of this study mainly arises from the limited sample population that was eventually analyzed in relation to the sample initially considered (n=150). Additionally, the time period during which patients should have received erlotinib treatment was not initially defined as a part of the inclusion criteria. Therefore, patients who had been on erlotinib treatment for more than 1 month were removed from the analyses at the time of the statistical analysis for the assessment of the primary and secondary endpoints, with the exception of the safety evaluation. In addition, a further limitation that should be acknowledged is the lack of data regarding new sites of metastases on disease progression.
However, despite the abovementioned limitations, this study provides useful real-world data on disease progression patterns and the clinical outcomes of patients with advanced or metastatic EGFR-mutant NSCLC undergoing first-line erlotinib treatment. Indeed, to the best of our knowledge, this is the first study evaluating the feasibility of re-biopsy on disease progression according to physicians and the attitudes of real-world patients with NSCLC regarding potential re-biopsy. In addition, to our knowledge, this is the largest prospective series focused on the assessment of patterns of disease progression and factors associated with PFS with erlotinib treatment for patients with advanced NSCLC harboring EGFR mutations.
The population of patients with NSCLC included in this real-world study reflects the demographic and clinical data traditionally described as being associated with the presence of EGFR-activating mutations. Thus, most patients were females, had never smoked, and had adenocarcinoma histology as previously seen in Caucasian patients with EGFR-mutant NSCLC (38, 39). Additionally, most EGFR-activating mutations were exon 19 deletions (54%) and exon 21 L858R point mutations (40%), which is consistent with previous data in Caucasians. Our findings might, therefore, be extrapolated to the general population with EGFR mutation-positive NSCLC.
In conclusion, this study supports the use of erlotinib as an effective first-line treatment option with manageable toxicity in patients with advanced or metastatic NSCLC carrying EGFR mutation. Furthermore, metastatic progression with asymptomatic disease has been identified as the predominant pattern of disease progression. This analysis also supports the potential prognostic value of liver metastasis on PFS in this population. Additionally, the feasibility of re-biopsy on disease progression with erlotinib treatment has been emphasized.
Acknowledgements
The Authors would like to thank the ASPET Study investigators for their contribution to the study. We also thank Roche Farma S.A. for supporting the study.
The Authors would also like to thank Cristina Vidal and Antonio Torres, from Dynamic Science (Spain), for their medical writing and editorial support, funded by Roche Farma S.A.
Footnotes
Authors' Contributions
J. Trigo contributed to the conception and design of the study, acquisition and interpretation of data, and manuscript preparation and critical review. A.L. Ortega-Granados, A. Artal-Cortes, D. Aguiar-Bujanda, J. Oramas, J.L. Fírvida, J. de Castro, and J. Campillo Fuentes contributed to the acquisition of data and critical review of the manuscript. R. Gordo and R. Galán participated in the conception, design and follow-up of the study, and in the critical review of the manuscript. All Authors approved the final version of the manuscript.
Conflicts of Interests
Dr. Trigo has served on advisory boards for Takeda, BMS and Boehringer and has also received speaker fees from BMS, Boehringer, Roche and Astrazeneca. Dr. Ortega-Granados has received research funding from Roche, Boehringer Ingelheim, Bristol-Myers-Squibb, and MSD. She has also received personal fees and non-financial support from Roche, Boehringer Ingelheim, Bristol-Myers-Squibb, MSD (lectures, travelling and writing assistance). Dr. Artal-Cortes has received travel support from Roche and served on advisory boards for this company. Dr. Aguiar-Bujanda has received personal fees for giving lectures from Roche and AstraZeneca. Dr. Fírvida has participated in advisory boards for Astra Zeneca, Boehringer, Lilly, MSD, and Roche. Dr. Oramas and Dr. Campillo declare that they have no competing interests. Rocio Gordo and Raquel Galán are Roche Farma employees (Medical Department).
- Received December 31, 2018.
- Revision received January 29, 2019.
- Accepted February 4, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.