


Abstract
Aim: To investigate the feasibility of hookwire-guided sentinel lymph node biopsy (SLNB) using contrast-enhanced ultrasonography (CEUS) followed by a one-step nucleic acid amplification (OSNA) assay. Patients and Methods: Clinical T1-2N0M0 breast cancer patients scheduled to undergo SLNB participated in this study. Both Sonazoid® and dye were used as tracers, and the most upstream sentinel lymph node (SLN) at each lymphatic flow detected by CEUS (First-SLN) was sampled under hookwire guidance, a procedure called “Sona-Hook”. Results: In each of the 50 cases, at least one First-SLN was extracted by “Sona-Hook”. All contrast-enhanced SLNs (CE-SLNs) were dye-positive, and the mean number of CE-SLNs sampled per patient was lower than that of dye-positive SLNs (1.48 vs. 1.88, p<0.01). Through OSNA, qualitative assessment of tumor metastasis between First-SLNs and all SLNs completely matched together. Conclusion: “Sona-Hook” for First-SLN followed by an OSNA assay may be a feasible minimally invasive SLNB strategy.
- Breast cancer
- sentinel lymph node biopsy
- one-step nucleic acid amplification (OSNA)
- hookwire
- contrast-enhanced ultrasonography (CEUS)
- Sona-Hook
Sentinel lymph node biopsy (SLNB) for clinically node-negative breast cancer has been established as a standard minimally invasive procedure for axillary staging. Sentinel lymph nodes (SLNs) are conventionally identified using a radioisotope (RI) and blue dye. The RI method is easy to perform and helps surgeons identify SLNs with certainty; however, there are related issues, such as a limited number of facilities that can handle RIs as well as radiation exposure. On the other hand, although the blue dye method alone does not necessitate a special facility for radiation protection, time is required to master the procedure, and missing any of the lymphatic flows produces a false-negative result when multiple lymphatic flows are present. Actually, it has been reported that the false negative rate of SLNB is higher in the blue dye method alone than in the combination method using both blue dye and an RI (1).
To potentially compensate for this weakness of the dye method alone, a near-infrared fluorescence system using green dye (indocyanine green: ICG) to detect SLNs has been reported to be useful (2, 3). However, there are problems such as the necessity of expensive fluorescent infrared cameras and difficulty in observing detailed lymph flow with fluorescent cameras when the lymph vessels are damaged and ICG diffuses to the surroundings. Considering that 33% of hospitals in Japan adopt the blue dye method alone for SLNB (4), the development of an alternative concise and accurate SLNB method is needed.
Recently, SLNB using contrast-enhanced ultrasound (CEUS) has been reported (5-10). Peri-areolar injection of an ultrasound contrast agent visualized the lymphatic flow from breast to axilla, and the identification rate of SLN by CEUS (CE-SLN) was between 70% and 100%. A standard surgical technique for SLNB using CEUS has not been established. In these studies, ultrasound contrast agent was used for SLNB in combination with blue dye and an RI (5, 7, 8), blue dye and computed tomographic (CT) lymphography (9), blue dye alone (6, 10), blue dye and ICG (6), and ICG alone (6). For the purpose of sampling CE-SLNs, their localization was noted by marking the skin with ink (5, 6, 9). As a more precise CE-SLN localization method, ultrasonography-guided placement of a hookwire in CE-SLN has been successfully developed (7, 8, 10).
Pathological diagnosis has been a conventional, standard method for the diagnosis of metastasis in SLNs. In recent years, a one-step nucleic acid amplification (OSNA) diagnostic assay (Sysmex Corporation, Kobe, Japan) for SLN metastasis has been developed that enables us to examine whole SLNs in a short time during operations, with a high sensitivity (11-13). Because metastasis in CE-SLN has been diagnosed by means of pathological diagnosis in previous studies, confirmation of the utility of the OSNA diagnostic assay for CE-SLN will broaden the performance of SLNB by the CEUS method in hospitals that adopt the OSNA assay for SLNB.
In the present study, we investigated the utility of hookwire-guided SLNB using an ultrasound contrast agent (perflubutane microbubble: Sonazoid®; Daiichi-Sankyo, Tokyo, Japan) and dye, named “Sona-Hook”, to accurately sample the most upstream SLN (First-SLN) at each lymphatic flow. In addition, we examined the feasibility of the OSNA diagnostic assay for CE-SLN. With regard to the dye used as a tracer for SLNB, the ICG fluorescence system (which has not been used in combination with Sonazoid® in previous studies except for our study) (6) or patent blue were administered to each patient.
Patients and Methods
Patients. Clinically T1-2N0M0 breast cancer patients (n=52) who had been scheduled to undergo SLNB at Osaka University Hospital between November 2017 and October 2018 were recruited in this study. Male breast cancer patients and those treated with neoadjuvant therapy were excluded. Two patients withdrew from our study the day before the operation; thus, a total of 50 patients took part in the study. The patients' clinical and pathological characteristics are shown in Table I. The cut-off value for the Ki67 labeling index was determined to be 20%. Surgical procedures such as total mastectomy or partial mastectomy were selected according to multiple parameters, including tumor location, breast size, patient preference, and so on. Immediate breast reconstruction was performed in 29% (9 of 31) of the patients undergoing total mastectomy. This prospective study was approved by the institutional review board of Osaka University Hospital (approval number 17126), and informed consent was obtained from each patient before surgery.
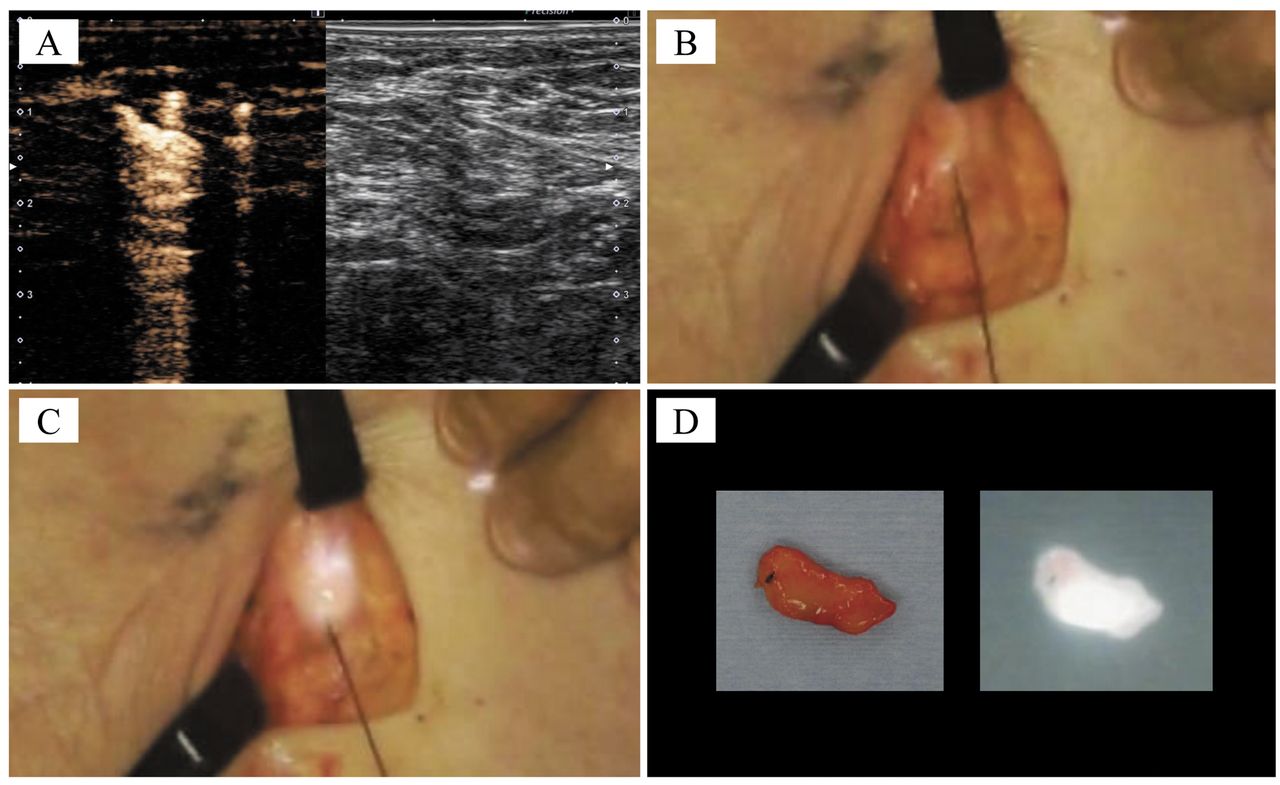
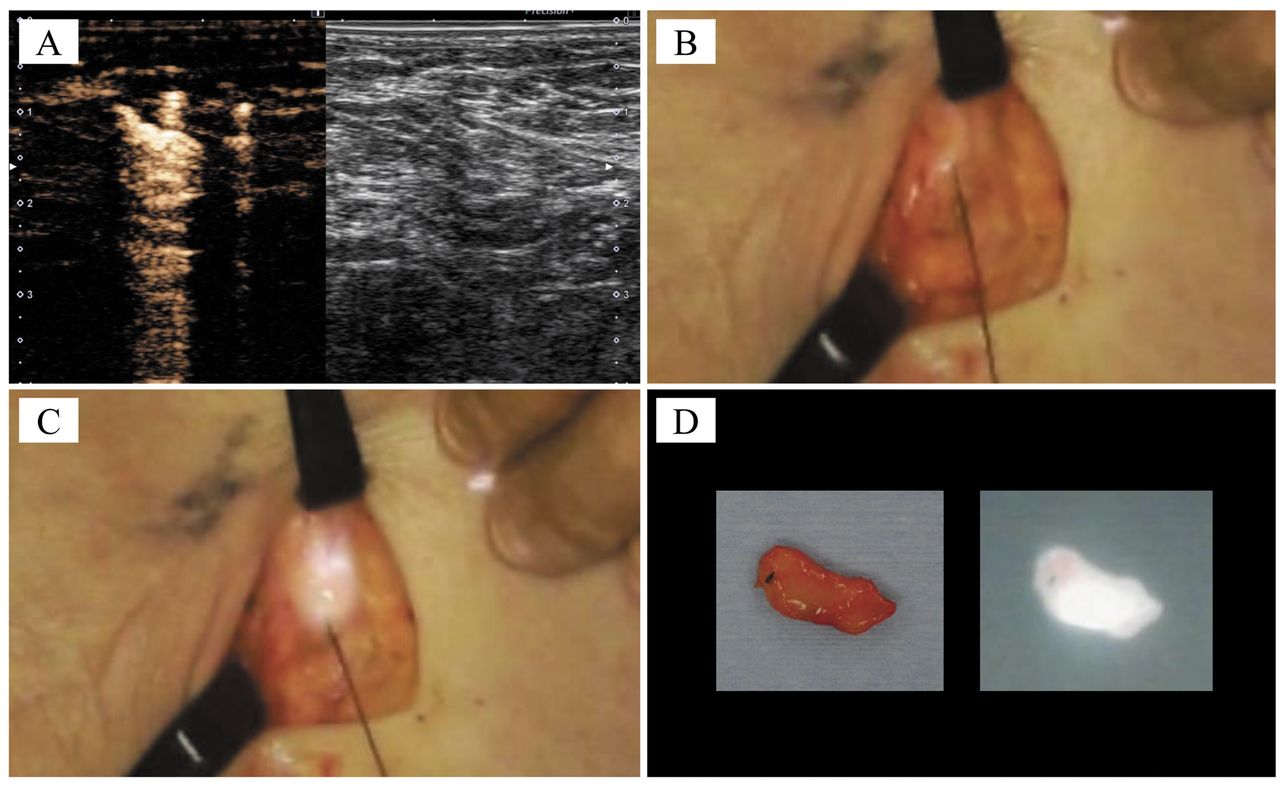
Sentinel lymph node biopsy. SLNB was performed using an ultrasound contrast agent (perflubutane microbubble: Sonazoid®; Daiichi-Sankyo, Tokyo, Japan) in combination with a dye (patent blue: n=40; ICG: n=10), and metastasis in SLN was detected by means of an OSNA assay (Sysmex Corporation, Kobe, Japan) (6, 12, 13). After periareolar injection of patent blue or ICG in an operating theater, Sonazoid® was injected into the adjacent area of the dye and manually massaged for 1-2 minutes. Then, lymphatic flow from the breast to the axilla was identified by contrast-enhanced ultrasound (CEUS) using Aplio i700® (Canon Medical Systems, Otawara, Japan) under the same conditions as Aplio 500® (6). The mechanical index and frame rate were set to 0.2 and 13 frames per second, respectively. After a short skin incision was made, a hookwire (D Wire BLN®, Argon Medical Devices, Inc., Athens, TX, USA) was indwelled under ultrasonic guidance to the most upstream CE-SLN (First-SLN) at each lymphatic flow, and the First-SLN was sampled while pulling the wire (called “Sona-Hook”). Downstream CE-SLNs, identified preoperatively, were also sampled by the “Sona-Hook” procedure. Following the First-SLN sampling, dye-positive SLNs were additionally biopsied. All extracted SLNs were examined by CEUS to investigate the remaining contrast agent inside them. Moreover, the axilla was subsequently examined by CEUS to confirm that all CE-SLNs had been extracted. When ICG was used for SLNB, ICG in the lymphatic flow from breast to axilla and SLNs were confirmed using a near-infrared monitor (Hyper Eye Medical System®, Mizuho Medical Co., Ltd., Tokyo, Japan). A representative “Sona-Hook” procedure is illustrated in Figure 1.
Clinical and pathological characteristics of breast cancer patients.

Procedure of hookwire-guided sentinel lymph node biopsy using a contrast agent and a blue dye, a protocol called “Sona-Hook”. The “Sona-Hook” procedure is presented. After periareolar injection of Sonazoid® (A), lymphatic flow from breast to axilla was observed by CEUS (B). The parallel display of CEUS shows a contrast-enhanced SLN located in the most upstream portion of a lymphatic flow (First-SLN) in a CEUS-mode setting (C, left) but not in a normal B-mode setting (C, right). After a short skin incision was made, the hookwire was inserted into the axilla (D) and was confirmed to be correctly positioned in the First-SLN (white arrow, E). Following placement of the wire, the insertion needle covering the wire was removed (yellow arrow, F). Subsequently, the skin incision was extended, the subdermal axillary tissues surrounding the hookwire were dissected while pulling the wire, and the First-SLN dyed with patent blue was detected (G) and then extracted (H). CEUS confirmed that Sonazoid® remained inside the sampled First-SLN (I), and there were no remaining CE-SLNs in the axilla (J). CEUS, contrast-enhanced ultrasonography; SLN, sentinel lymph node; CE-SLN, contrast-enhanced sentinel lymph node.
In vitro feasibility study of sentinel lymph node biopsy using contrast agent by means of one step nucleic acid amplification system (n=2).
At the beginning of the study, the accuracy of the OSNA diagnostic assay for SLNs containing Sonazoid® was examined in vitro (n=2). In the OSNA assay, SLNs are homogenized by 4 ml of lysis buffer, and each sample is diluted ten times. Therefore, assuming that a total amount of 16 μl (=1 vial) of Sonazoid® reached an SLN, the final added concentration of Sonazoid® in the sample tube was 0.04% (v/v), which was defined as the top concentration. Then, 0.04%, 0.004%, 0.0004% and 0% of Sonazoid® were added to OSNA lysis buffer in each sample tube, respectively, and the OSNA assay was conducted for the CK19 mRNA high sample, CK19 mRNA low sample and CK19 mRNA negative sample, respectively (Table II). Because the qualitative assessment did not differ irrespective of the concentration of Sonazoid®, we concluded that Sonazoid® did not affect the results of the OSNA assay in vitro.
Statistical analysis. The number of SLNs sampled per patient according to the dye and/or Sonazoid® was compared using a paired t-test. JMP® PRO 14 software (SAS Institute, Inc., Cary, NC, USA) was used for all statistical analyses. p-Values <0.05 were determined to indicate statistically significant differences.
Results
“Sona-Hook” for First-SLNs. In all cases, lymphatic flow from breast to axilla was clearly visualized, and at least one First-SLN was detected by CEUS. Details of the lymphatic flow to First-SLNs were as follows: one lymph duct flowed into one First-SLN (n=33), two lymph ducts flowed into one First-SLN (n=2), and two lymph ducts flowed into two First-SLNs separately (n=15). The median size of 65 First-SLNs in 50 cases was 8.4 mm (range=3.5-19.3 mm). All First-SLNs were sampled successfully under hookwire guidance, and it was confirmed that the hookwire was positioned inside (n=47) or adjacent to the surrounding tissue (n=18) of the First-SLNs. Additionally, the remaining contrast agent inside all extracted First-SLNs was confirmed by CEUS. A small hematoma with a diameter of approximately 2 cm due to the hookwire insertion was observed in the axilla of one case, but no severe complications were observed in the present study.
Association of the number of sampled SLNs according to different tracers for SLNB. Based on the analysis on a node-by-node basis, 68 CE-SLNs, including 65 First-SLNs and 3 downstream CE-SLNs, were identified preoperatively and were sampled by “Sona-Hook”. In addition, 5 downstream SLNs containing both dye and Sonazoid® were detected by trimming of sampled First-SLNs, and 3 SLNs sampled by the dye method were shown to contain Sonazoid®. As a result, 76 SLNs containing Sonazoid® were sampled and confirmed to be dye-positive. On the other hand, the number of SLNs detected by dye alone was 18. Thus, the total number of extracted SLNs was 94. Based on the analysis on a patient-by-patient basis, only First-SLNs were detected as CE-SLNs in 94% (47 of 50) of the patients and were sampled by “Sona-Hook”. As a result, the mean number of SLNs sampled by “Sona-Hook” for each patient was lower than that sampled by the dye procedure (1.48 vs. 1.88, p<0.01).
Association of metastasis diagnosis between only First-SLNs and all SLNs. In the present study, 4 cases (8%) and 5 cases (10%) were shown to have macrometastasis and micrometastasis in SLNs, respectively. Detailed metastatic information of the SLNs in these 9 cases is shown in Figure 2. Among the 9 SLN metastatic cases, 4 cases with SLN macrometastasis and 1 case with SLN micrometastasis underwent additional axillary lymph node dissection (ALND), and 3 of 4 cases with macrometastasis had non-SLN metastasis. In each metastatic case, at least one First-SLN harbored metastasis. On the other hand, of 41 cases without First-SLN metastasis, 18 cases had additional downstream SLNs, and none of them harbored metastasis. The association of the metastatic diagnosis between First-SLN and whole SLNs is shown in Table III. Consequently, diagnosis based on the findings of First-SLNs and that based on the findings of all SLNs, which also include SLNs detected by dye alone, completely matched each other.
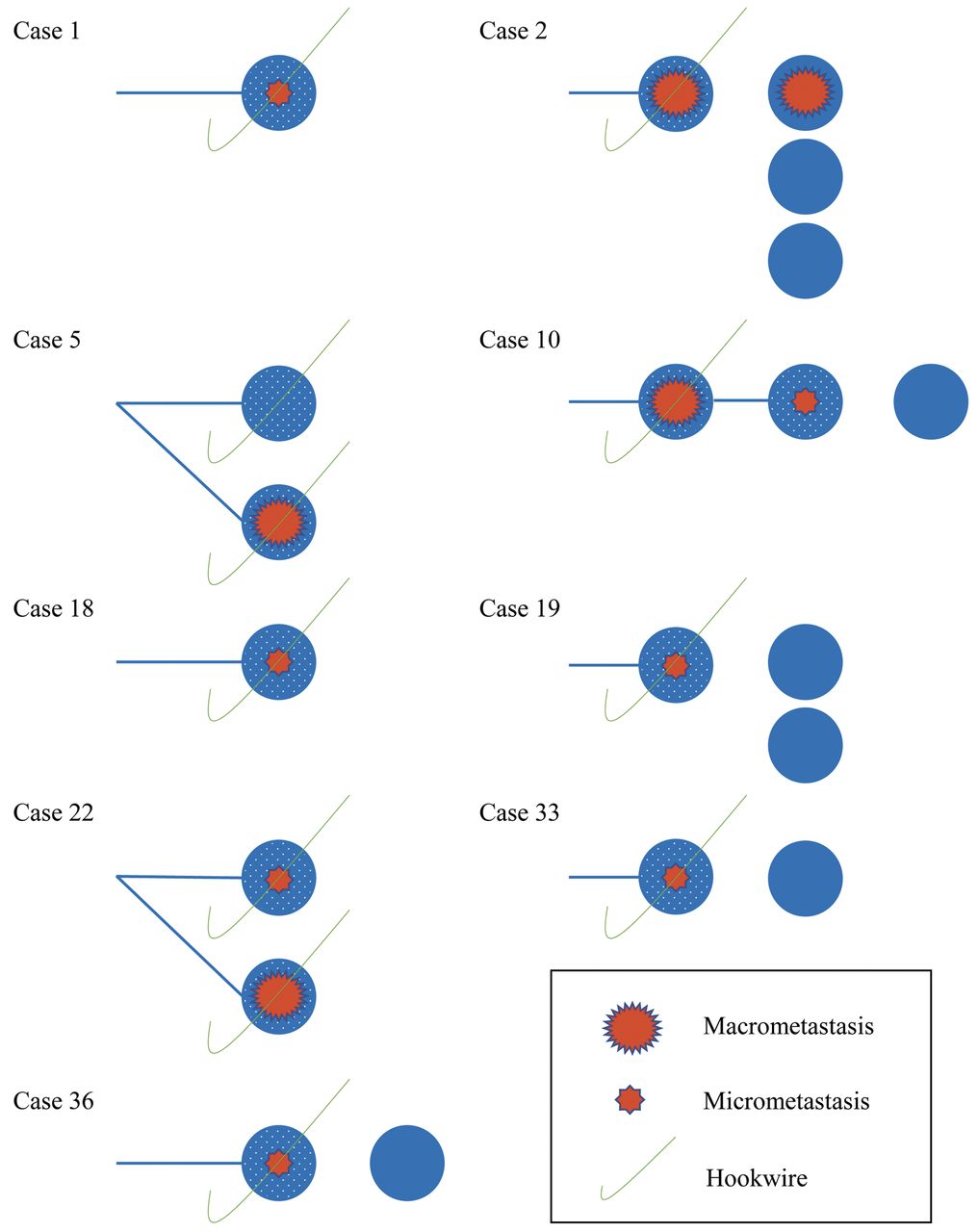
Case series of breast cancer patients whose sentinel nodes harbored metastasis. Detailed axillary status of nine cases with SLN metastasis, including macrometastasis in 4 cases and micrometastasis in 5 cases, are presented. All First-SLNs, which are defined as the most upstream SLNs of lymphatic flows (blue lines) from breast to axilla, were positive for both ultrasound contrast agent and dye (blue circle with dots inside). SLNs that were positive for dye alone (blue circle without dots) were identified in 5 cases. Metastatic diagnosis based on the findings of First-SLNs sampled by the “Sona-Hook” procedure reflected the diagnosis based on whole SLNs. SLN, sentinel lymph node.
Representative procedure of sentinel node biopsy using a contrast agent and green dye (ICG). SLNB using Sonazoid® in combination with ICG was performed on 10 patients. A CE-SLN was detected in the axilla (A), and subsequently, a hookwire was placed in the SLN according to the “Sona-Hook” procedure. At the beginning of dissection of the axillary subdermal tissue surrounding the wire, ICG in the SLN was not visualized by a near-infrared camera (B) but was clearly visualized by the camera by pulling the hookwire (C). An extracted CE-SLN stained by ICG was unclear to the naked eye (D, left), whereas ICG inside the SLN was clearly identified by the near-infrared camera (D, right). SLNB, Sentinel lymph node biopsy; ICG, indocyanine green; CE-SLN, contrast-enhanced sentinel lymph node.
Discussion
In the present study, we investigated the feasibility of the “Sona-Hook” procedure. First, lymphatic flow from the breast to axilla was clearly visualized by periareolar injection of Sonazoid® using CEUS, and First-SLNs were identified in all cases, yielding an identification rate that was almost the same as that reported in previous studies (6, 9). Subsequently, all First-SLNs were successfully sampled under hookwire guidance, which was also the same result as in previous reports (7, 8, 10). For 10 of 50 patients, lymphatic flow and SLNs were visualized by periareolar injection of ICG using a near-infrared camera at the same time as CEUS, and First-SLNs were clearly demonstrated to be ICG-positive (Figure 3). As we have reported previously, no severe complications were observed in the study (6).
Association of metastatic diagnosis between First-SLNs and all SLNs.

Flow chart of treatment based on intraoperative diagnosis of First-SLNs sampled by the “Sona-Hook” procedure. A proposal of the decision tree for the management of SLNB is shown. First, “Sona-Hook” followed by an intraoperative detection method of SLN metastasis such as OSNA or conventional pathological assay is recommended as an initial SLNB for First-SLNs. Next, if there is no metastasis or only micrometastasis in the First-SLNs, ALND can be spared. In case macrometastasis is detected in First-SLNs of a patient undergoing breast-conserving surgery, additional sampling of residual SLNs in the axilla followed by treatment according to the ACOSOG-Z0011 criteria is recommended. On the other hand, when macrometastasis is found in the First-SLNs of patients undergoing breast mastectomy, conventional ALND or additional sampling of residual SLNs followed by radiation therapy to the axilla as an option are recommended. SLNB, Sentinel lymph node biopsy; SLN, sentinel lymph node; OSNA, one-step nucleic acid amplification; ALND, axillary lymph node dissection; Bp, breast-conserving surgery; Bt, breast mastectomy; ACOSOG, American College of Surgeons Oncology Group; RT, radiation therapy.
Next, differences in the number of SLNs sampled according to the SLN identification method were analyzed. As a result, a patient-by-patient analysis demonstrated that the mean number of CE-SLNs was significantly lower than that of dye-positive SLNs and that all CE-SLNs were dye-positive. This result is the same as that in our previous reports (6), suggesting that Sonazoid® tends to remain in the upstream SLNs longer than the dye, possibly because the mean diameter of Sonazoid® (2-3 μm) is larger than that of the dye. In fact, 96% (65 in 68) of CE-SLNs identified preoperatively were First-SLNs, and only 4% of them were downstream SLNs. Consequently, the application of Sonazoid® as a tracer for SLNB may enable us to perform a more efficient SLNB.
In our study, 18% of the total patients showed macrometastasis (8%) or micrometastasis (10%) in SLNs. The patient-by-patient analysis showed that the diagnosis based on the results of First-SLNs was perfectly consistent with that based on the results of whole SLNs. This result led us to re-realize the significance of the sampling of First-SLNs for an accurate SLNB. Considering our results showing that the mean number of SLNs sampled by the “Sona-Hook” procedure was lower than that sampled by the dye procedure and that the diagnoses based on the First-SLN findings completely aligned with those based on the findings for whole SLNs, sampling only First-SLNs is expected to enable us to minimize unnecessary surgical manipulation of the axilla, leading to a minimally invasive SLNB.
Based on the analysis of lymphatic flow from the breast to axilla, 30% of the patients were shown to have two lymphatic flows to two SLNs, and in one of these patients (case 5), metastasis was found in one SLN. In such a case, SLNB using the dye-alone method poses a risk for overlooking one of the lymphatic flows to a First-SLN, producing a false-negative result. SLNB using the dye-only method has been reported to yield a lower identification rate as well as a higher false-negative rate than those using both dye and RI (1, 14). On the other hand, SLNB using both dye and an ultrasound contrast agent yielded a high identification rate in our present and past trials, although the false-negative rate has not been investigated (6). Therefore, the combination method using a dye and an ultrasound contrast agent for SLNB may contribute to reducing the risk of overlooking First-SLNs, leading to more precise axillary staging.
The OSNA assay, but not the conventional pathological assay, was used for the detection of SLN metastasis in the present study. This assay enables us to determine the necessity of additional ALND during the operation for patients undergoing total mastectomy or those undergoing partial mastectomy and do not meet the criteria of the American College of Surgeons Oncology Group (ACOSOG) Z-0011 (15). In addition, we developed a nomogram to predict four or more axillary lymph node metastases based on the OSNA results (16). Therefore, the OSNA assay in combination with the nomogram also facilitates the decision regarding optimal adjuvant therapy for patients undergoing breast partial mastectomy and meet the criteria of ACOSOG Z-0011. At the beginning of this study, it was confirmed that the use of Sonazoid® does not affect the results of the OSNA diagnostic assay in vitro. As an in vivo finding, 18% of patients showed macro- or micro-metastasis in SLNs, which is a slightly lower frequency than that reported in the previous reports (17, 18). This may be because 78% of the patients participated in this study had clinical stage I tumors that had a low possibility of disseminating to the axilla. On the other hand, as mentioned above, the diagnosis of SLN metastasis was completely in accordance between First-SLNs and all SLNs that also contained SLNs detected by dye alone, demonstrating that the ability of OSNA to diagnose CE-SLNs is the same as that for SLNs that contain dye alone.
In recent years, the combination of microbubble technology and ultrasound has shed light on the field of antitumor therapy, such as drug delivery systems (19-21) and hyperthermia (22), as well as the diagnosis of cancer (23). A drug delivery system using microbubbles and US is reportedly based on the finding that microjets produced by oscillations or destruction of the microbubbles increase the permeability of vessel membranes (24, 25). On the other hand, the use of hyperthermia is reported to be based on the fact that destruction of microbubbles induced by acoustic exposure increases the temperature around a tumor (22). In the present study, perflubutane microbubbles were used as a tracer for SLNB, and SLNs were detected by US. Perflubutane tends to be destroyed under the conditions of a high mechanical index (MI) and a high frame rate, and the possibility that microbubbles under the conditions of our study damage the surrounding tissue is low (26). In fact, CEUS-guided liver needle biopsy using perflubutane microbubbles under conditions similar to our study has been reported to be useful (27). In addition, in this study, we could not find any specific abnormal alteration of the cellular morphology or protein expression of CE-SLNs by means of hematoxylin-eosin or immuno-histological staining compared to the findings for SLNs detected by dye alone (data not shown). In summary, performing SLNB by the “Sona-Hook” procedure followed by the OSNA and pathological diagnostic assays seems clinically reasonable.
Based on the results obtained from the present study, a decision tree for the management of SLNB can be proposed, although future studies including larger patient samples are needed to evaluate this strategy (Figure 4). First, “Sona-Hook” followed by intraoperative detection of SLN metastasis using OSNA or conventional pathological assay is recommended as an initial SLNB for First-SLN. Next, if there is no metastasis or only micrometastasis in the First-SLNs, ALND can be spared. If macrometastasis is detected in First-SLNs of a patient undergoing breast-conserving surgery, then additional sampling of residual SLNs in the axilla followed by treatment according to the ACOSOG Z-0011 criteria, which indicate the possibility of omission of ALND for clinical T1-2 breast cancer patients with at most two SLN macrometastases who will be treated with optimal systemic therapy, is recommended (15). On the other hand, when macrometastasis is found in the First-SLNs of patients undergoing breast mastectomy, conventional ALND or additional sampling of residual SLNs followed by radiation therapy to the axilla as an option is recommended (28, 29). In the application of the decision tree using the “Sona-Hook” procedure to the patients of the present study, 92% (46 in 50) of the patients could be treated with only First-SLN biopsy for axillary staging; thus, it is expected that the decision tree will give such patients the benefit of undergoing minimally invasive axillary staging. In addition, OSNA can provide us with the metastatic information on SLNs intraoperatively based on the examination of the whole specimen; thus, OSNA has the advantage that it does not contain a risk of a mismatch between intra- and postoperative diagnosis, whereas conventional intraoperative pathological diagnosis has a risk of a false negative result. Furthermore, an intraoperative predictive model for non-SLN metastasis based on the finding of SLN metastasis by means of OSNA has been developed recently (16) and is expected to help us choose the indication for additional ALND.
In conclusion, our results indicated that a hookwire-guided First-SLN biopsy using Sonazoid®, named “Sona-Hook”, was successfully performed and shown to be technically feasible for SLNB. In addition, the diagnostic feasibility of the OSNA assay for SLNs containing Sonazoid® was demonstrated. First-SLN biopsy by means of “Sona-Hook” followed by OSNA may enable us to perform accurate and minimally invasive SLNB. The results of our study need to be validated in a larger prospective study.
Acknowledgements
The Authors are grateful to Hiroki Shoji of the Laboratory for Clinical Investigation at Osaka University Hospital for performing the OSNA diagnostic assay.
Footnotes
Authors' Contributions
TM, KS and SN designed the study, and wrote the initial draft of the manuscript. All Authors have contributed to data collection, analysis and interpretation, and critically reviewed the manuscript. All Authors approved the final version of the manuscript, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
This article is freely accessible online.
Conflicts of Interest
Dr. Noguchi has received research funding and honoraria from Daiichi-Sankyo Co., Ltd., and Sysmex Corporation for work performed outside of the current study. Dr. Shimazu received honoraria from Sysmex Corporation for work performed outside of the current study. Dr. Naoi received research funding and honoraria from Sysmex Corporation for work performed outside of the current study. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
- Received September 22, 2019.
- Revision received October 10, 2019.
- Accepted October 11, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.