


Abstract
Background: Bilateral asynchronous renal cell carcinoma (RCC) is infrequent. Immunotherapy is the first-line treatment for advanced RCC not controlled by locoregional therapy. Viscum album extracts (VAE) have been shown to improve quality of life as well as immunological and antineoplastic properties in different types of cancers. Case Report: A 67-year-old man was diagnosed with Fuhrman grade 3/4 RCC, stage pT1bN0M0 in the right kidney. During the subsequent 6 years, he underwent a right nephrectomy and two metastasectomies (lung). Then an RCC lesion of the left kidney was detected. The patient refused a second nephrectomy and was treated solely with high-dose intravenous and subsequent subcutaneous VAE. A central necrotic area and a peritumoral halo were seen on an ultrasound follow-up from month 7. The patient showed no further progression of RCC during the next 2.5 years. Conclusion: As far as we are aware of, this is the first report of a patient with metastatic RCC with an RCC lesion of the second kidney treated solely with high-dose intravenous and subcutaneous VAE, associated with 2.5 years of progression-free survival and a good quality of life. The use of VAE in RCC should be carefully documented and published to determine future research.
Renal cell carcinomas (RCCs), which originate within the renal cortex, constitute 80-85% of all primary renal neoplasms. The global incidence varies widely, with the highest rates in the Czech Republic and North America (1). In the United States, there are approximately 65,000 new cases and almost 15,000 deaths from RCC each year (2). RCC is more common in men and occurs predominantly in the sixth to eighth decade of life (3). The clear-cell subtype (ccRCC) is the most common (75-85%). A high nuclear grade (Fuhrman grade 3-4) or the presence of a sarcomatoid pattern is associated with poor prognosis (4). RCC presents as a localized (confined to the kidney, 65%), regional (spread to the regional lymph nodes, 16%), or metastatic (16%) disease. Bilateral RCC without a hereditary component is rare (3-5% of cases) and tends to be asynchronous, occurring within 10 years of the primary diagnosis and treatment (5). Studies suggested inferior survival rates for asynchronous RCC, but others did not find differences compared with synchronous bilateral RCC (6-8).
Surgery (radical or partial nephrectomy) can often be curative in patients with localized RCC. There is no defined systemic adjuvant therapy after complete surgical resection. For patients with a high risk of tumor recurrence after nephrectomy, sunitinib has been approved based on improvements in disease-free survival compared with placebo but at the cost of high toxicity (9). Resection of solitary metastases from RCC is associated with a 5-year survival rate of 35% to 50% in selected patients (10). Immunotherapy with checkpoint inhibitors and molecularly targeted therapy are the first-line treatments for patients with advanced RCC whose disease is not controlled by definitive locoregional therapy (11).
Viscum album extract (VAE) is made from European mistletoe (V. album), a hemi-parasitic shrub that grows on different host trees (e.g. ash, birch, apple, oak) and contains a variety of bioactive compounds, the most studied being mistletoe lectins and viscotoxins (12,13). VAE has strong cytotoxic- and apoptosis-inducing effects, leading to immune stimulation, and inhibition of tumor cell migration, and neoangiogenesis, including down-regulation of a variety of cancer genes involved in tumor progression (14-17). VAE is widely used as injectable standardized preparations in supportive therapy among patients with cancer, especially in German-speaking countries (13). Extracts are administered parenterally (subcutaneously, intravenously) in an increasing dose according to an individually adapted schedule. Intratumoral and intracavitary applications, even at high dosages, have been reported (18). Clinical trials have shown improvement in the quality of life and promising effects of VAE on survival in patients with cancer (19-21). Tumor remissions have been reported in small trials and single cases, usually after local high-dose VAE applications (22-26). In a recent case report, a long survival time was reported for a patient with RCC adjunctly treated with VAE (27). To our knowledge, no clinical data have been published on the sole use of high-dose intravenous and subsequent subcutaneous VAE in bilateral asynchronous ccRCC.
Case Report
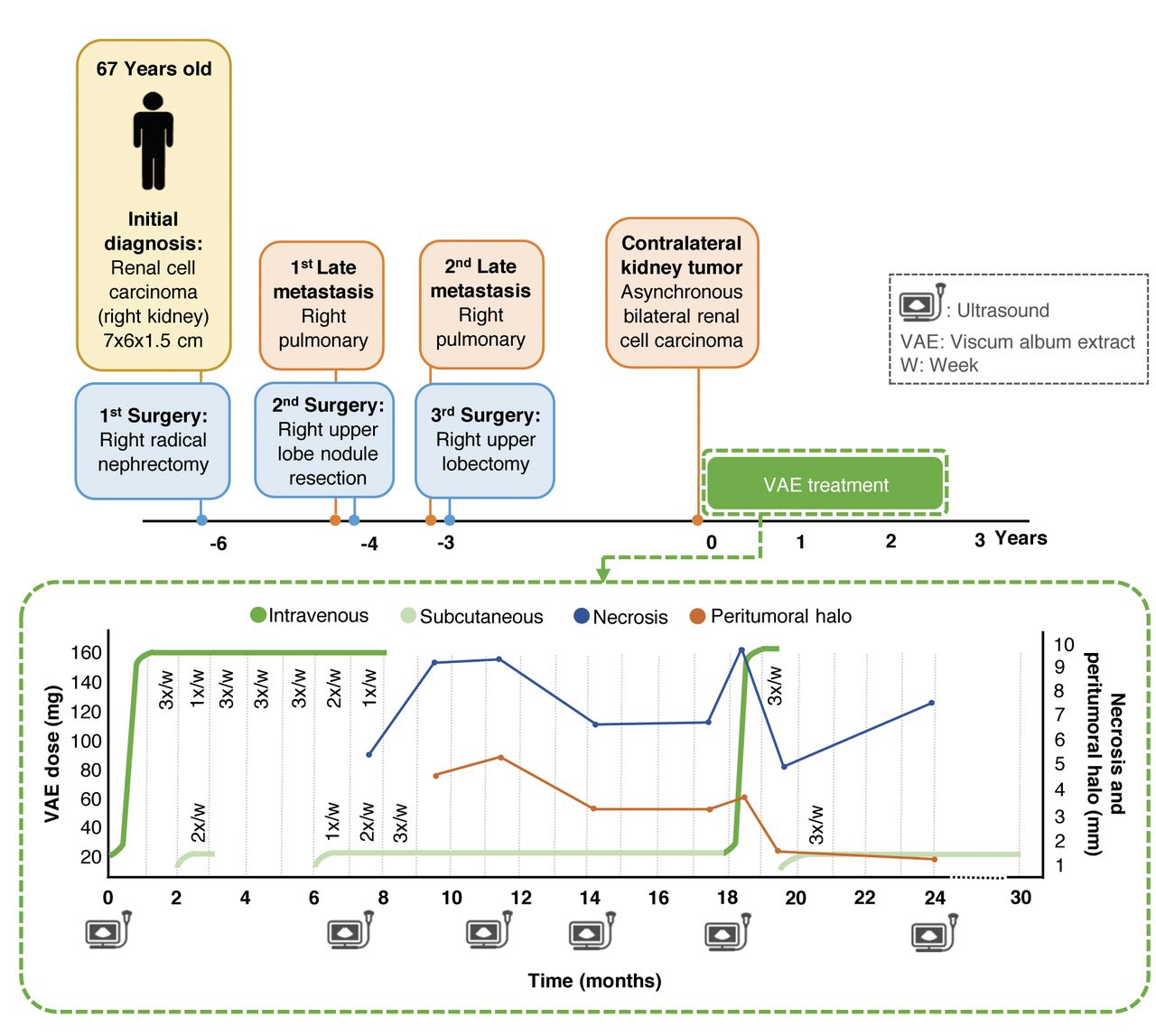
A 67-year-old Peruvian man had been suffering from unusual fatigue and fever for 4 months. A computed tomographic scan showed a lesion in the right kidney and no lesion in the left one. The patient underwent radical right nephrectomy, which showed a tumor of 5.5×5.0×4.9 cm with Fuhrman grade 3-4 and a clear-cell pattern (pT1bN0M0) (Figure 1 A and B). Three years later, he underwent segmentectomy for a lesion (1.9×1.8×1.6 cm) in the right upper lung, which was diagnosed as an RCC metastasis (Figure 1C). A year later, the patient underwent right upper lobectomy for a new metastatic lesion that appeared in the same lung (equally confirmed as a metastasis of the RCC). Another 3 years later, a contralateral kidney tumor was discovered during regular surveillance. There was no family history of hereditary RCC. His oncologist suggested radical left nephrectomy; however, the patient refused because of dialysis dependence after surgery. The patient decided to seek a different treatment option with an integrative approach and presented himself at our Institution (Centro Médico Antroposófico). Therapy with a high-dose intravenous and subsequent subcutaneous application of VAE from the host tree ash, AbnobaVISCUM® Fraxini (ABNOBA GmbH, Pforzheim, Germany) in an increasing dose thrice per week was started (for details of the course see Table I and Figure 2). No other cancer-specific treatments were used.
Magnetic resonance imaging after 21 months of VAE therapy showed a slightly increased tumor of 4.5×4.7×5 cm (vs. 4.5×3.6×3.3 cm at baseline). A follow-up ultrasound examination was periodically carried out. A central necrotic area and a peritumoral halo appeared in month 7 and was seen until the patient's last evaluation in month 28 (Figures 2 and 3). The largest width of the necrotic area (9.7 mm) and peritumoral halo (4-5 mm) were seen in months 11 and 18. From month 18, the peritumoral halo was observed to be incomplete (Figure 3). The tumor retained peripheral and central hypervascularity as observed by color Doppler ultrasound; the serum creatinine level and renal resistive index remained stable, within normal values.
The patient remained asymptomatic with a good quality of life during the whole treatment period. He did not present any adverse reaction to the intravenous and subcutaneous VAE applications. After 2.5 years of VAE treatment, 9 months of intravenous treatment and subsequent subcutaneous treatment, no tumor progression was detected.
Antecedent and concomitant therapies. At presentation, the patient was a retired engineer, married, and had two children. He swam regularly and had done so since he was very young. Further diagnoses were hypertension (at the age of 37 years) and bilateral inguinal hernias (operated). He had a presumptive diagnosis of renal tuberculosis and received specific antibiotic treatment for only 1 week; it was stopped because of the findings of computed tomography and, subsequently, the pathological report confirmed a diagnosis of RCC. Daily medications for hypertension included 100 mg atenolol, 25 mg chlortalidone and 20 mg enalapril. The patient also took food supplements: Vitamin C, folic acid, magnesium, and zinc. Furthermore, he followed a diet of reduced salt and proteins to protect kidney function.
Patient perspective. “From now on, my perspective is to consolidate my full security in the mistletoe. Further, (to) get more information about its properties and applications – in short, to know more. So, as far as possible, I contributed to its dissemination in my circle of friends within my reach. I knew the product at a very critical time; it would be my fourth oncological surgery and, this time, in my only kidney that would be very ill-treated with an operation that removes the tumor. I received the applications of mistletoe with a lot of faith and (was) convinced that I was right, I knew cases of close friends with surprising results too.”
Discussion
We report a case of a patient with detection of a ccRCC tumor of the contralateral kidney after a history of ccRCC and metastatic recurrences in the lungs (bilateral asynchronous ccRCC stage IV), who showed stable disease for 2.5 years under treatment only with high-dose intravenous and subcutaneous VAE, after having refused oncological surgery. During the VAE treatment, a central necrotic area and a peritumoral halo were seen on ultrasound. No other cancer-specific treatment was used.

Biopsy of the primary renal tumor (hematoxylin and eosin stain): A: Fuhrman grade 3/4 clear cell renal cell carcinoma with moderately irregular nuclear contours and visible nucleoli (400×). B: Fat tissue slightly compromised (100×). C: Biopsy of the pulmonary metastasis: compatible with primary clear-cell renal cell carcinoma (100×).
Viscum album extract (VAE) treatment (2.5 years=30 months).

Timeline of the patient with asynchronous bilateral renal cell carcinoma stage IV treated with Viscum album extract (VAE) for 30 months.
RCC is an immunogenic neoplasm with frequent infiltration of immune cells (28), occasional spontaneous regression (29), a high number of gene insertions and deletion mutations (30), and impressive results from immunotherapy in subpopulations (31).
Bioactive compounds of VAE have immunomodulatory properties that stimulate the innate and adaptive immune system pathways and lead to neutralization of tumor-induced immunosuppression (14, 32). The induction of an immune response against tumor tissue, with encapsulation of the tumor under VAE treatment, has been described in a case report on adenoid cystic carcinoma after intratumoral applications (26). Tumor encapsulation is described as a process of the creation of a fibrous layer with an intermediate phase of inflammation, associated with a better prognosis (33, 34). In our patient, the necrotic area and peritumoral halo observed in the unremoved tumor showed two peaks in maximum width, both after high-dose intravenous VAE. We presume the peritumoral halo and necrosis may have been a result of an inflammatory tumor response after high-dose intravenous VAE. The immunological reaction to VAE includes the stimulation and proliferation of CD4+ T-cells, which can activate inflammatory cells (macrophages, natural killer cells, and eosinophils) around the tumor (14, 35).
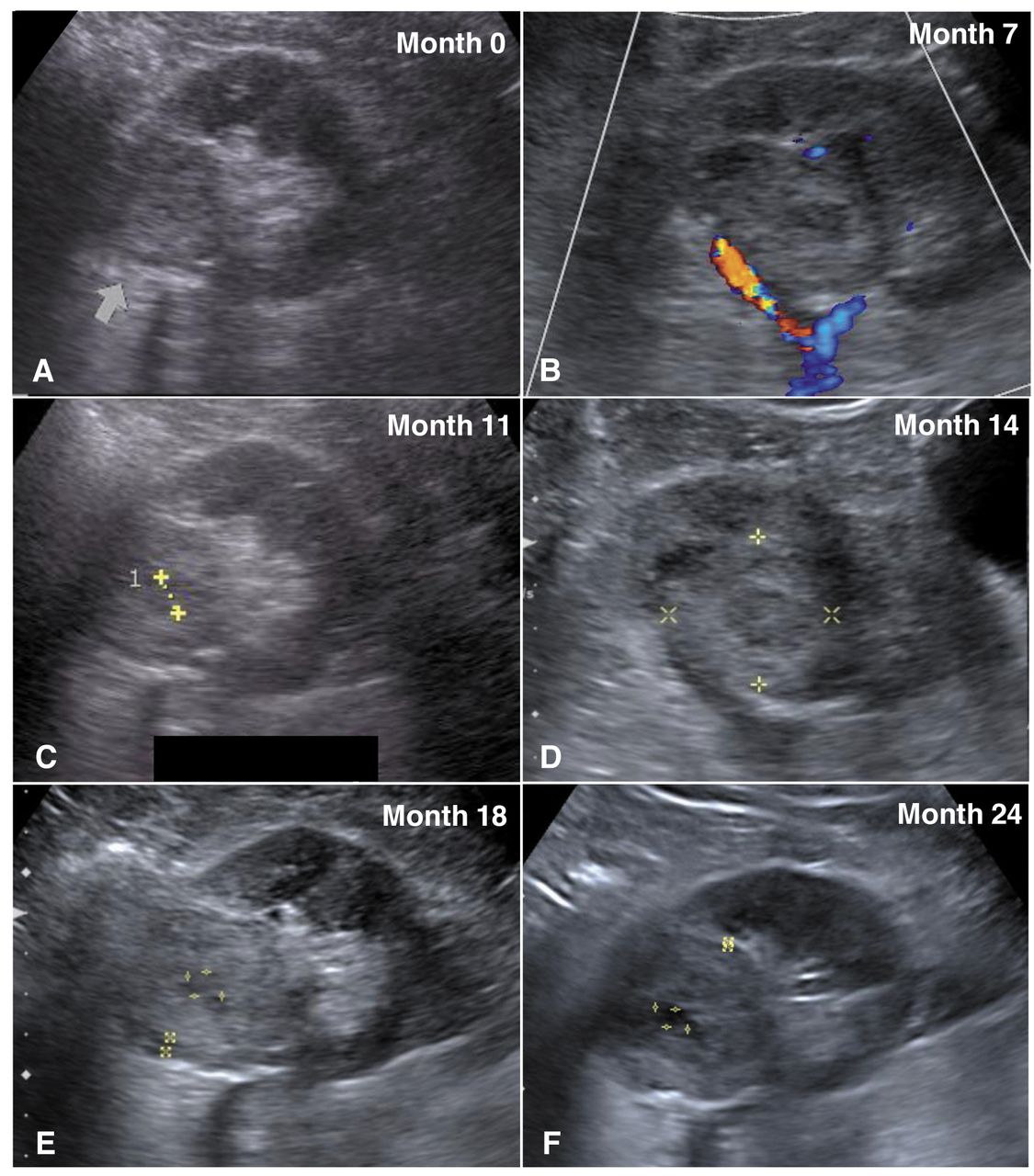
Kidney ultrasound evolution of the patient with clear-cell renal cell carcinoma during the first 24 months of treatment with Viscum album extract. A peritumoral halo and necrotic area were observed from month 7 until month 30 (last follow-up). A-F: Ultrasound images from 0, 7, 11, 14, 18, and 24 months, respectively. Arrow in A: The tumor.
Exceptionally long survival times under VAE therapy without progression of the tumor have been described in several cases reports in different cancer types, including RCC (25, 27, 36-40). Given the immunological properties of VAE and the immunogenic nature of RCC, we presume the VAE treatment to have contributed to tumor control in our patient.
RCC is also known for late recurrence; lesions can appear 10 years or more after the initial surgical treatment (41). A contralateral kidney tumor may be considered a late recurrence (asynchronous) but may also represent a de novo pathology. For this case, the patient did not have a pathological report of the left kidney tumor. However, it is difficult to distinguish between the two possibilities on clinicopathological features alone (8). The presence of two previous lung metastases and a second kidney tumor in a period of 6 years is suggestive of the presence of latent metastases rather than a new primary. The prognosis of latent asynchronous RCC does not significantly differ from that of unilateral RCC, suggesting that, despite treatment, these types of tumor tend to recur; generally, they grow slowly (41). However, 3 months before the diagnosis of the second renal lesion, the ultrasound assessment did not reveal a tumor, probably because it was too small to be detected at that point. This may suggest a rather fast pattern of tumor growth. Additionally, the patient had risk factors for early recurrence, such as male gender, advanced age, stage IV tumor, and Fuhrman grade 3-4.
Radical nephrectomy of localized primary RCC can be curative. However, 20-30% of patients will eventually develop recurrent or metastatic disease (42). Our patient has had three recurrences across a period of 6 years (since diagnosis). He decided not to undergo a second nephrectomy for the latest recurrence. Then he started with VAE treatment alone, and after 2.5 years with continuous surveillance, no progression of the tumor has been reported.
As no other tumor-specific treatment was used, we presume that VAE contributed to this positive outcome. Still, this represents a single case. Regarding the current state of evidence, VAE injections cannot replace surgery or other effective anticancer treatments.
Conclusion
To our knowledge, this is the first report on the sole use of high-dose intravenous and subcutaneous VAE treatment in a patient with bilateral asynchronous stage IV ccRCC, who has shown a stable disease for 2.5 years and a good quality of life. The use of VAE in RCC should be carefully documented and reported in order to determine future research.
Acknowledgements
The Authors are thankful to the Stiftung Integrative Medizin, Stuttgart, Germany, and the Christophorus Stiftung, Stuttgart, Germany for financial support. We also thank Dr. Cesar Vela-Velasquez from the Instituto de Investigación de Citopatología (CITOPAT) for the histological images and Dr. Yober Espinoza Zárate from the Centro Médico Antroposófico (CMA) for the ultrasound images and reports. This case report was prepared following the CARE guidelines (43).
Footnotes
Authors' Contributions
MR contributed to the case report design, collected and provided data, was the principal author of the article, and is the guarantor of the article and all data. YV contributed to the case report design, was the physician-in-charge for the patient, provided data, and reviewed the article. PW, GK, and HK contributed to the case report design, reviewed the article, and supervised the report and publication process. All authors approved the final version of the article.
This article is freely accessible online.
Informed Consent
Written informed consent for patient information and images to be published was provided by the patient, who read the final version of the article and confirmed his content.
Conflicts of Interest
The Authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
- Received August 18, 2019.
- Revision received September 3, 2019.
- Accepted September 11, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.