


Abstract
Background/Aim: Tyrosine kinase inhibitors are important in the treatment of metastatic renal cell cancer (mRCC). The aim of the study was to evaluate the costs and effects of sunitinib in mRCC. Patients and Methods: A total of 81 mRCC patients who received first-line sunitinib therapy between 2010 and 2014 were recruited. Drug doses, laboratory and imaging studies, outpatient visits and inpatient stays were recorded. Health-related quality of life (HRQoL) was measured (15D- and EQ-5D – 3L questionnaires). Results: The cost of sunitinib (mean 22,268 €/patient range 274 € to 105,121 €) covered 73% of the total costs during the treatment period. The total treatment cost was 30,530 €/patient (range=1,661-111,516 €). The median overall survival was 17.9 months. HRQoL decreased during treatment. Conclusion: The main cost during sunitinib treatment of mRCC was the drug itself (73% of the total costs). Drug costs and HRQoL should be considered when choosing treatment for mRCC.
Renal cell carcinoma (RCC) is the most common kidney carcinoma (other malignancies in kidney occur in the cortex, pelvis and ureters). In 2018, kidney cancers accounted for over 400,000 new cases and approximately 175,000 deaths worldwide (1). Lifestyle and health-related issues, such as smoking and obesity, have been identified as risk factors for RCC in many reports during recent decades (2, 3). Renal cell carcinoma presents little or no symptoms in its early stages (4). Due to a lack of symptoms, the disease is diagnosed in an advanced or metastatic phase (mRCC) in approximately one third of the cases. Currently, most RCC cases are discovered as an incidental finding (5).
Medical treatments for mRCC are constantly evolving, and many drugs targeting different pathways are used today (6). Originally, immunotherapy with high-dose interleukin-2 (IL-2) or interferon-alfa (IFN-α) was considered the primary choice (7-9). The recognition of the von Hippel-Lindau (VHL) tumor suppressor gene led to the presentation of vascular endothelial growth factor (VEGF) and VEGF receptor-targeted therapies, such as bevacizumab and tyrosine kinase inhibitors (TKIs) (10-12). Today, immune-check-point inhibitors, such as nivolumab and ipilimumab have changed the landscape for mRCC treatment (13-15). These agents have increased the overall survival and objective response rates of mRCC compared to sunitinib. Sunitinib is a TKI, that has shown an increase in progression-free survival (PFS) compared to IFN-α (16). Sunitinib is still the current standard of care especially in low-risk mRCC (15). It has been compared to several new TKIs, to their combination with check-point inhibitors and to everolimus (17-19). Recently, the combination of nivolumab and ipilimumab was shown to be superior to sunitinib as a first-line treatment of mRCC (14), but according to our new results, sunitinib may still have a beneficial effect after the combined treatment of nivolumab and ipilimumab (20). There is still a need to investigate sunitinib as a first-line treatment in mRCC patients, the costs of this treatment and the patients' use of other healthcare services during this treatment.

First-line sunitinib treatment doses divided (%) according to duration of treatment (days).
Patients and Methods
Based on real-world clinical practice, we conducted a prospective observational clinical study. We collected data from different clinical practices in four university hospitals and one central hospital in Finland during first-line sunitinib treatment from January 12, 2010, to November 30, 2014. The patients (n=81) were recruited among regular mRCC patients in the different clinics, and the study itself did not have an effect on physicians' decisions concerning the patients' treatment.
The inclusion criteria were as follows: patient was clinically fit for first-line sunitinib treatment in mRCC and signed an informed consent. The exclusion criteria were as follows: patient was not treated with sunitinib and/or did not give consent for collecting data from the patient register. The local ethics committee (R09045) approved the study. The trial identifier is NTC00980213.
Health related quality of life (HRQoL) was measured with the 15D- and EQ-5D-3L-questionnaires at baseline, at day 28 during sunitinib treatment and at the beginning of each new cycle (21, 22). The 15D-measures mobility, vision, hearing, breathing, sleeping, eating, speech (communication), excretion, usual activities, mental function, discomfort and symptoms, depression, distress, vitality, and sexual activity. The patient chooses a grade from one to five, that best describes his/her state of health at the moment. The 15D score, representing the overall HRQoL on a 0-1 scale (1=full health, 0=being dead) and the score on the different dimensions mentioned above (scale 0-1: 1=no problems, 0=being dead), are calculated from the questionnaire by using a set of population-based preference or utility weights. The minimum clinically important change or difference in the 15D-score has been estimated to be ±0.015 on the basis that people on average can feel such a difference (21). HRQoL measured with the 15D-questionnaire was compared to a sample of age- and gender-standardized general population based on an earlier National Health Survey (23).
Researchers in the participating clinics collected the data, and the data collection ended on November 30, 2014, or on the day that the patient died, if prior to the end of follow-up. The basic patient information, the data of their carcinoma and the data concerning the use of other health care services were collected on a structured form.
The recorded information was background information (date of birth, gender, nephrectomy information, date of diagnosis, and information on the risk-groups) and the use of health care resources (active medical cancer treatment, other medical treatment related to cancer, clinical visits, inpatient stay, radiation therapy, radiological imaging, laboratory tests and blood transfusions). The reason for ending the sunitinib treatment was to be recorded at the time when the final decision was made. The collected data were entered into a digital database.
The use of health care resources was valued mainly by using the average Finnish health care unit costs (24). If these costs were not available, unit costs (Helsinki University Central Hospital price tables) were used. The unit costs were converted to the 2014 value using the price index for public healthcare expenditures (24). The medical treatment costs based on the patients' individual dose were calculated with retail prices without taxes. The costs of medical treatment given in the hospital were calculated with wholesale prices without value-added tax. A national price catalogue was used as a source of single drug costs.
Results
In total, 81 patients were included in the analysis. The mean age of patients was 66.1 years (range=41.1-85.7 years), 55 were male and 26 were female (68% vs. 32%, respectively). Nephrectomy had been performed on 58 patients (72%). At the end of the follow-up, over half of the patients had died (n=47, 58%).
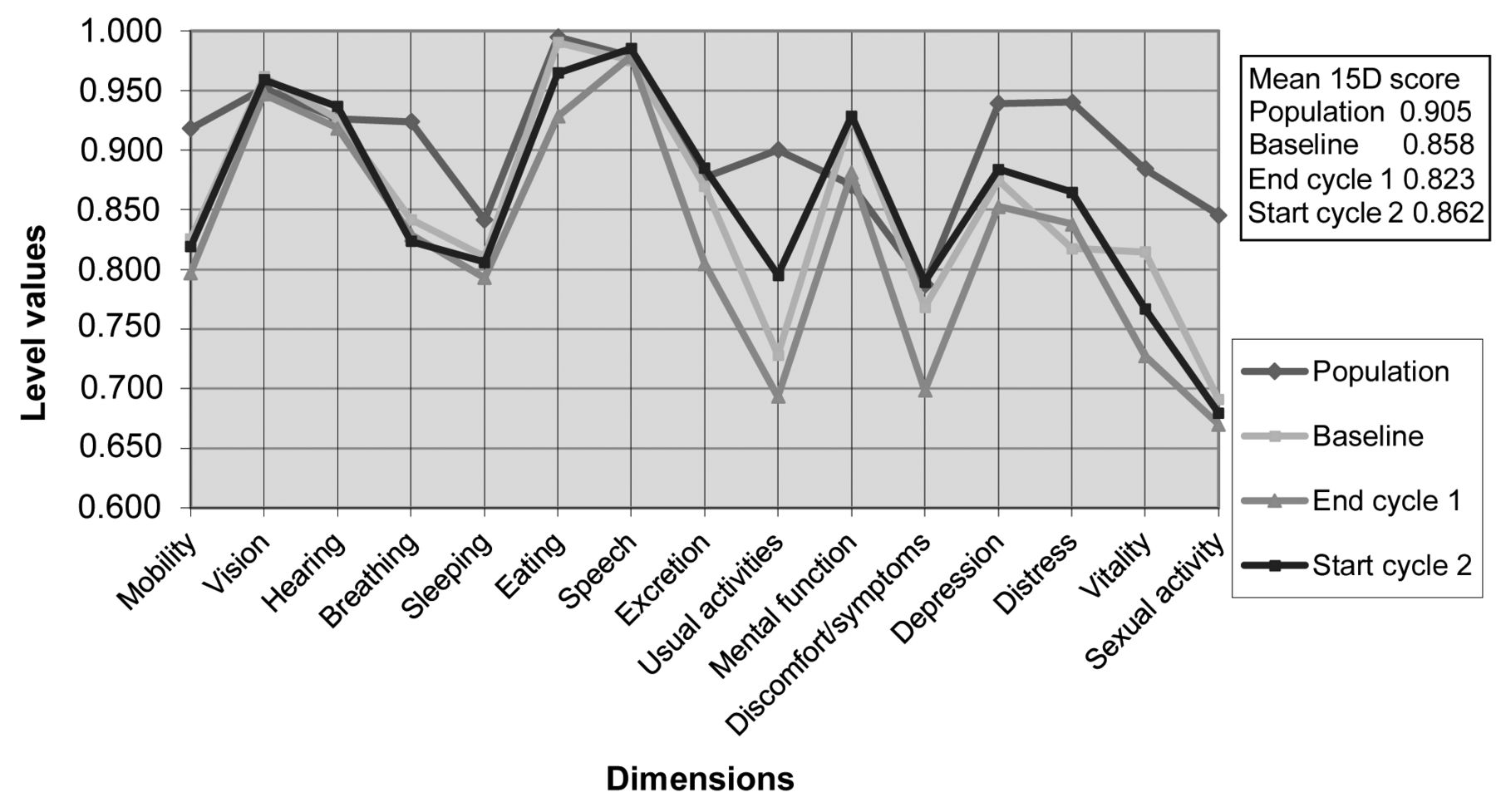
The mean 15D profiles and scores of the patients and those of an age- and gender-standardized sample of the general population.
All the costs during first-line sunitinib treatment (N=81).
The six-week treatment cycles included a four-week sunitinib period and a two-week-cycle pause. Treatment discontinuation for a longer period was considered a prolonged pause. For the entire study population (n=81), we received 20,513 follow-up days for sunitinib treatment, including pauses during treatment, with a mean of 253 days/patient (range=3-1,389 days). Sunitinib was given for a total of 12,741 days, with a mean of 157 days/patient (range=3-728 days). Figure 1 describes the doses used combined with the time of use during the treatment period.
The total cost of sunitinib treatment was 1,803,714 € and 88€/treatment day when pauses were also taken into account. The average cost for a sunitinib treatment day was 142 €, and the mean cost per patient was 22,268 € (range=274-105,121 €) for the entire treatment and follow-up period. The most often used dose of sunitinib was 37.5 mg, which represents 42% of all treatment days. The second most common dose used was 50 mg, equivalent to 33% of all treatment days.
At the end of the study, 77 out of 81 patients had discontinued sunitinib treatment. The most common reasons for ending the treatment were disease progression (55%) or side effects (25%). Four patients proceeded with first-line sunitinib treatment at the study endpoint. The drug costs related to adverse effects were not reported. Concerning the total costs of sunitinib first-line treatment, the expense of the medication itself was significant (73% during the sunitinib treatment period).
Costs and their breakdown are presented in Table I. Inpatient stays and outpatient visits created most of the costs related to the use of other healthcare resources (other than relevant medical treatment) during first-line sunitinib treatment. The cost for individual patients based on these findings was 30,530 € (range=1,661-111,516 €). The average cost per month was 3,617 €.

The mean 15D- and EQ-5D-3L scores at different time points.
Approximately 51% of patients who had received first-line sunitinib treatment proceeded with a second-line active treatment. The most common second-line treatment medications were everolimus (27.3%), pazopanib (10.4%) and sorafenib (9%). In general, active treatment was discontinued after the third- or fourth-line medication, yet some patients received up to seven lines of treatment. The mean drug costs for treatment lines 2, 3, 4, 5, 6 and 7 were 19,794 €, 20,429 €, 59,106 €, 11,706 €, 2,923 € and 18,696 €, respectively.
At the beginning of treatment, the average 15D-score of patients was lower than that of the age- and gender-standardized general population (0.858 vs. 0.903). The difference was statistically significant and clinically important. The patients were significantly worse off, especially on the dimensions of mobility, breathing, daily activities, mental functions, depression, anxiety, vitality and sexual activity (Figure 2). The mean 15D-score declined 0.035 from the beginning to 28 days of sunitinib treatment, and the score returned to its original level during the two weeks of medication pause. In some cases, the 15D-score during the pause was even higher than at the beginning of the treatment.
At the beginning of treatment, the average EQ-5D-3L-score was 0.755. It declined by 0.080 following 28 days sunitinib treatment. It also returned to its original level during the two-week break and, in some cases, to an even higher level (0.781). All of these changes in the quality of life parameters were statistically and clinically significant. During the second treatment period, the EQ-5D-3L-score declined in a statistically significant way, yet the difference was no longer clinically significant. In all the later measurements from both instruments, there were no statistically or clinically significant differences in the HRQoL of those patients continuing on sunitinib treatment (Figure 3).
Discussion
The majority of the costs (73%) for treating mRCC patients during first-line sunitinib, came from the medication itself. This finding is similar to our earlier study concerning mRCC treatment with IFN (25). It is also in line with other results in the literature: cancer-specific targeted therapy itself is the largest expense in contemporary cancer treatment, especially in the first-line treatment of many metastatic diseases.
According to our research, most patients received second-line treatment, but treatment proceedings after that were less common. In total, six complete responses were recorded, and the average overall survival from the start of the first-line sunitinib treatment was two year. These results are also similar to findings in the literature (17-19, 26). In most patients, treatment was discontinued because of disease progression, which is very typical of metastatic cancer. The general treatment doses and protocols were performed according to international guidelines (15, 16). The overall HRQoL in our patients was already lower than that in the age- and gender-standardized general population, yet it remained stable during treatment cycles. Similar results have been observed in other RCC trials (27).
According to the latest cost-effective analysis in mRCC, life expectancy of patients receiving nivolumab plus ipilumab was 3.99 life years, which was 1.27 life-years more than that of intermediate- or poor-risk patients receiving sunitinib as first-line treatment. The cost per additional QALY gained was USD108,363 (28). As discussed earlier, the drug itself remains the largest cost driver in the treatment of mRCC. Sunitinib seems to be a much less expensive treatment option than nivolumab plus ipilumab. However, sunitinib does not offer a survival gain in intermediate- or poor-risk patients, so to reach cost-effectiveness, sunitinib should be directed to good-risk patients. According to recent guidelines, this seems to be the case (28-30). When comparing previously mentioned treatments, the adverse effects and drug administration should also be taken into account.
Acknowledgements
The study was supported by Pfizer Finland and by Grants from the Research, Development and Innovation Center of Tampere University hospital (9UO020 and 9V017).
Footnotes
Authors' Contributions
Vuorinen has taken part in designing the study, gathering data, analyzing the data, and is the main author of the article. Paunu, Turpeenniemi-Hujanen, Reunamo Jekunen, Kataja, Sintonen, Purmonen, have taken part in designing the study, collecting the data, interpretation of the data and critically reviewing the manuscript. Kellokumpu-Lehtinen is the principle investigator.
Conflicts of Interest
Vuorinen, Reunamo, Jekunen and Kataja have no conflicts of interest. Sintonen is the developer of the 15D and one of the developers of the EQ-5D-3L. Paunu has received conference support from Amgen, Bayer, Merck, Roche, Servier, BMS, Lilly, Pfizer and Novartis. Turpeenniemi-Hujanen has attended domestic congress (MSD). Purmonen is currently employed by Novartis Finland Oy. Kellokumpu-Lehtinen has received expert report fee from Bristol-Myers Squibb and conference support from Sanofi.
- Received August 24, 2019.
- Revision received September 3, 2019.
- Accepted September 10, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Efficacy of Sunitinib in Patients With Favorable and Intermediate Risk Metastatic Renal Cell Carcinoma - Lithuanian National Cancer Institute Experience
- Gonadal Function in Male Patients With Metastatic Renal Cell Cancer Treated With Sunitinib
- G-Protein-coupled Estrogen Receptor 1 Agonist G-1 Perturbs Sunitinib Resistance-related Phosphoproteomic Signatures in Renal Cell Carcinoma
- Estimating the Lifespan of Elderly Patients With Cerebral Metastases from Kidney Cancer
- PTEN Is Involved in Sunitinib and Sorafenib Resistance in Renal Cell Carcinoma
- Interval Between Cancer Diagnosis and Radiotherapy - An Independent Prognostic Factor of Survival in Patients Irradiated for Bone Metastases from Kidney Cancer
- Management of Patients With Metastatic Renal Cell Cancer and Bone Metastases