


Abstract
Background/Aim: The potential of the DNA mismatch repair (MMR) system as a prognostic predictor has been evaluated in several cancer types. However, associations between MMR and the prognostic factors of ovarian cancer are poorly understood. Patients and Methods: MLH1 expression was evaluated by immunohistochemistry in patients with advanced serous ovarian cancer treated with platinum- and taxane-based chemotherapy. Associations between MLH1 expression and clinicopathological factors as well as claudin-4 expression were examined. Results: Low MLH1 expression was significantly associated with increased progression-free and overall survival, and a normalisation of CA125 levels after chemotherapy. Additionally, low claudin-4 expression was more frequently found among the group with low MLH1 expression. Conclusion: Low MLH1 expression was associated with improved prognosis and is a possible predictor of the chemosensitivity of ovarian cancer. Claudin-4 might be involved in the molecular mechanisms underlying how MLH1 influences survival and chemosensitivity in patients with ovarian cancer.
Ovarian cancer is the leading cause of death from gynaecological malignancies and the fifth most common cause of cancer-related deaths in women (1). As effective screening methods have not been established and there is a lack of characteristic symptoms in early stages, most patients are diagnosed with advanced-stage ovarian cancer (2). The standard therapy for advanced ovarian cancer consists of radical debulking surgery followed by platinum-based chemotherapy. Since 1996, a combination of platinum and paclitaxel has become the standard-of-care first-line chemotherapy regimen (3). First-line chemotherapy with platinum and paclitaxel yields a response rate of >80% (4); however, despite this initial high response rate, nearly all patients experience relapse (5). The treatment for recurrent ovarian cancer is often difficult due to resistance to chemotherapeutic agents (6), and the 5-year survival rate for those with advanced ovarian cancer is <30% (1). Therefore, identifying novel biomarkers that can predict chemosensitivity and survival are needed to improve the clinical outcomes of patients with ovarian cancer.
One of the risk factors for ovarian cancer is hereditary predisposition, and the most recognized hereditary contributors to ovarian cancer are germline mutations in breast cancer susceptibility genes (7). Mutations in DNA mismatch repair (MMR) genes are the next most common cause of hereditary ovarian cancer (7). MMR genes are necessary for detecting DNA nucleotide mismatches and small insertions and deletions in the genome and play an important role in recruiting factors that repair damaged DNA (8, 9). Several proteins, such as mutL homolog 1 (MLH1), postmeiotic segregation increased-2, MutS homolog 2, and MutS homolog 6 are involved in the human MMR system (9, 10). MMR deficiency leads to the accumulation of mutations throughout the genome and causes various malignancies (11-14). Recently, detection of MMR deficiency in tumours has become increasingly important because of the recent approval of an immunotherapy-based programmed cell death protein 1 inhibitor by the U.S. Food and Drug Administration for patients with MMR-deficient solid tumours. The potential of members of the MMR system as prognostic biomarkers has been intensely evaluated in several cancer types (15, 16); however, associations between the MMR system and prognostic factors in ovarian cancer are poorly understood.
MLH1 is a key component of the MMR system, and inactivation of MLH1 is the primary reason for MMR deficiency (17, 18). Furthermore, MLH1 has been shown to interact with proteins involved in apoptosis signalling and other DNA repair systems, such as BRCA, P53, and X-linked inhibitor of apoptosis protein (19-21). It has not been confirmed whether MLH1 is a prognostic factor for ovarian cancer, and there have been few reports about the molecular role of MLH1 in ovarian cancer. In this study, we investigated MLH1 protein expression in advanced serous ovarian cancer treated with platinum- and taxane-based chemotherapy to determine if MLH1 is biomarker that can predict survival and chemotherapy response. Additionally, we evaluated the molecular mechanisms underlying the involvement of MLH1 in survival and chemotherapy response in ovarian cancer.
Claudin, a primary component of tight junctions, plays a role in a wide variety of processes, including cell signalling, proliferation, differentiation, and motility (22, 23). Claudin is also associated with survival and chemotherapy response in ovarian cancer (24-27). Finally, it has been suggested that there is a close relationship between MLH1 and claudin (28-33). Therefore, we also evaluated the correlation between MLH1 and claudin expression in order to identify molecular mechanisms that link MLH1 to survival and chemotherapy responses in ovarian cancer.
Patients and Methods
Patients. This study included 28 patients with ovarian cancer who had been treated between April 2011 and December 2018. Informed consent was obtained from all patients, and the Ethics Committee of Saitama Medical University International Medical Center approved this study (approval no. 16-296). All patients were staged by the International Federation of Gynaecology and Obstetrics system (34). Patients were eligible if they had newly diagnosed, histologically proven advanced (stage III or IV) serous ovarian cancer, primary peritoneal cancer, or fallopian-tube cancer. Eligible patients had also received platinum- and taxane-based chemotherapy as their first-line treatment after undergoing either biopsy or up-front cytoreductive surgery. Patients who did not have pathological diagnoses, had insufficient clinical data, or who had received previous chemotherapy were excluded from this study. Responses to chemotherapy were assessed every three cycles by computed tomographic scans according to the Response Evaluation Criteria in Solid Tumors (RECIST) (35).
Immunohistochemistry. Ovarian cancer tissues were fixed with 10% buffered formalin and embedded in paraffin. Five-micrometre sections were deparaffinized in xylene and rehydrated in graded ethanol solutions. Antigen retrieval was performed for 20 min at 95°C using Target Retrieval Solution (K8004; DAKO, Kyoto, Japan). Endogenous peroxidase activity was blocked with 0.3% hydrogen peroxide for 10 min at room temperature. The slides were then stained according to the DAKO Envision protocol (DAKO) using a 1:50 dilution of mouse monoclonal antibody to MLH1 (ES05; DAKO) and a 1:300 dilution of mouse monoclonal antibody to claudin-4 (3E2C1; Thermo Fisher Scientific, Waltham, MA, USA). Slides were visualized using 3,3’-diaminobenzidine tetrahydrochloride and haematoxylin. Nuclear staining of normal lymphocytes and stromal cells was used as a positive internal control for MLH1, while normal colonic tissue was included as a positive control for claudin-4.
Immunohistochemical analysis. Quantitative analyses of MLH1 and claudin-4 expression were performed as follows (24). The percentage of positively stained tumour cells was determined in three separate fields at 100× magnification and assigned to one of the following categories: 0, no immunostaining; 1, 1-33% positive cells; 2, 34-66% positive cells; and 3, 67-100% positive cells. The intensity of immunostaining was scored as follows: 0, no immunostaining; 1, weak; 2, moderate; and 3, intense. The percentage of positively stained tumour cells and the staining intensity were then multiplied to produce an expression score for each specimen (score 0-9). Scoring of MLH1 and claudin-4 expression were performed by two experienced gynaecologists who were blinded to all patient data. Patients were then divided into two groups according to their MLH1 and claudin-4 expression scores. MLH1 or claudin-4 expression scores ≤4 were defined as low expression, while scores >4 were defined as high expression.
Statistical analysis. The Chi-square test and Student t-test were used to evaluate associations between MLH1 expression and clinicopathological variables. Kaplan–Meier curves were produced for progression-free survival (PFS) and overall survival (OS). Both PFS and OS were calculated from the date of initial surgery or biopsy. The log-rank test was used to compare survival between the two groups. Statistical significance was set at p<0.05.
Results
Patient characteristics regarding MLH1 expression. Immunoreactivity for MLH1 was observed in the nuclei of ovarian cancer cells. Figure 1A and B show examples of low and high MLH1 expression, respectively. In total, 11 out of the 28 (39%) patients with ovarian cancer examined in this study had low MLH1 expression, while 17 (61%) had high MLH1 expression.
Patient characteristics and tumour features are compared between the two groups in Table I. There were no significant differences in age, Eastern Cooperative Oncology Group performance status score (36), FIGO stage, tumour grade, or residual tumour size after initial surgery between the two groups. Clinical characteristics did not differ significantly between the two groups.
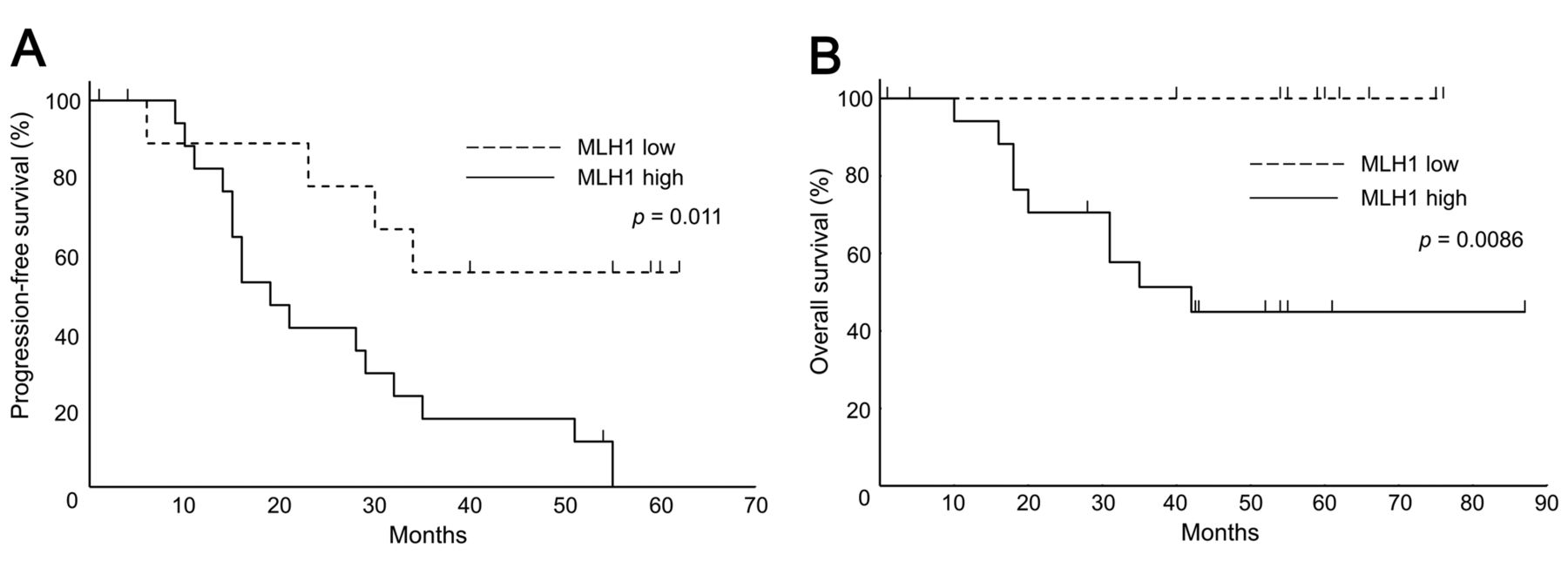
Survival analysis according to MLH1 expression. We evaluated the association between MLH1 expression and survival of patients with advanced serous ovarian cancer. The median length of follow-up for patients overall was 43 (range=1-88) months. Patients with low MLH1 expression had significantly longer PFS than those with high MLH1 expression (p=0.011, Figure 2A). Furthermore, all patients with low MLH1 expression were alive at the time of the last follow-up visit, and these patients had significantly longer OS than those with high MLH1 expression (p=0.0086, Figure 2B).
Chemotherapy response regarding MLH1 expression. We assessed the impact of MLH1 expression on response to platinum- and taxane-based chemotherapy. Tumour responses were assessed every three chemotherapy cycles by computed tomography. Two patients in the low MLH1 expression group were excluded from evaluations of response because they refused to receive chemotherapy after two or fewer cycle. Assessments of tumour response using RECIST were possible in five patients from the low MLH1 group and 12 patients from the high MLH1 group. Although there was no statistically significant difference in tumour response between the two groups, all patients in the low MLH1 group showed responses to platinum- and taxane-based chemotherapy (Table II, p=0.51). Next, we assessed tumour response between the two groups by measuring the CA125 level. CA125 is well validated as an accurate and reliable means of monitoring response to chemotherapy in ovarian cancer and a CA125 level <35 IU/ml is generally considered normal (37, 38). As mentioned above, two patients from the low MLH1 group were excluded from this evaluation. The mean CA125 level before treatment was 2697 in the low MLH1 group and 2265 in the high MLH1 group (p=0.72, Table III). A normalisation of CA125 level after platinum- and taxane-based chemotherapy occurred significantly more frequently in the low MLH1 group than in the high MLH1 group (p=0.035, Table III).
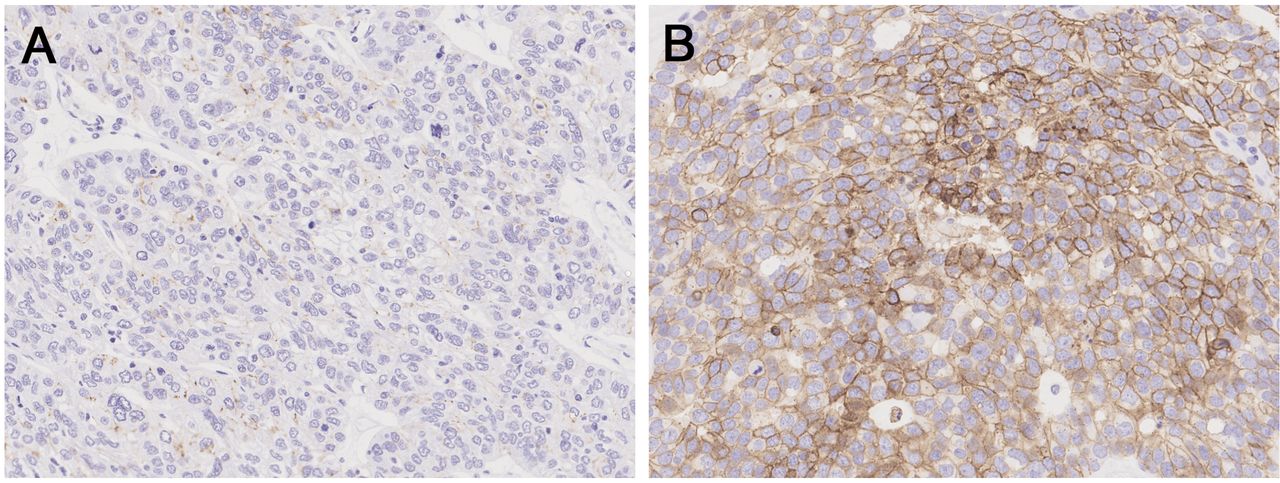
Analysis of the association between claudin-4 and MLH1 expression. Immunoreactivity for claudin-4 was observed in the cytoplasm and cell membrane of ovarian cancer cells. Figure 3A and B show examples of low and high claudin-4 expression, respectively. Among the low MLH1 group, 82% of cases had low claudin-4 expression in contrast with only 47% of the high MLH1 group (Figure 4). Although the rate of low claudin-4 expression was higher in the group with low MLH1 expression, the difference was not statistically significant (p=0.066).
Discussion
In this study, we investigated the clinical associations of MLH1 protein expression with survival and chemotherapy response in advanced serous ovarian cancer treated with platinum- and taxane-based chemotherapy. This revealed two important findings. Firstly, we found that patients with ovarian cancer with low MLH1 expression had better prognoses compared with those with high MLH1 expression. We also found that the CA125 level normalized after platinum- and taxane-based chemotherapy significantly more frequently in patients with low MLH1 expression compared with those with high MLH1 expression. Secondly, we found that low claudin-4 expression was more common in ovarian cancer with low MLH1 expression, compared with cancer with high MLH1 expression.
Our study demonstrated that patients with advanced serous ovarian cancer with low MLH1 protein expression had significantly better PFS and OS than those with high expression. To date, only a few studies have investigated the association of MLH1 expression with survival in ovarian cancer, and previous results have generated inconclusive results. Scartozzi et al. suggested that loss of MLH1 protein expression correlated with improved OS in advanced ovarian cancer (39). However, their study failed to find a relationship between MLH1 expression and time to progression. Furthermore, there were certain differences in patient characteristics compared with our study. The patients in their study were treated with the cisplatin, epirubicin and cyclophosphamide regimen and included several histological types, whereas the patients in our study were treated with platinum- and taxane-based chemotherapy and included only those with serous histology.
Clinicopathological parameters according to mutL homolog 1 (MLH1) expression.
Response to chemotherapy according to mutL homolog 1 (MLH1) expression in evaluable cases.

Representative mutL homolog 1 (MLH1) immunostaining in the nuclei of ovarian cancer cells. A: Low MLH1 expression. B: High MLH1expression. Original magnification: 200×.

Kaplan–Meier curves of progression-free (A) and overall (B) survival. Patients with ovarian cancer with low mutL homolog 1 (MLH1) expression had significantly longer progression-free and overall survival compared with those with high MLH1 expression.
In contrast, Ding et al. showed that high MLH1 expression correlated with better survival outcomes in patients with advanced serous ovarian cancer who received platinum-based chemotherapy (21). They investigated the correlation between MLH1 mRNA expression analysed by microarray and survival duration (shorter than 3 years or longer than 7 years after diagnosis), which differed from our study, wherein associations of MLH1 protein expression with PFS and OS were evaluated. Additionally, Zhao et al. reported that low MLH1 mRNA level correlated with unfavourable OS in patients with ovarian cancer treated with platinum-based chemotherapy (40). However, they did not find any association between MLH1 mRNA expression and OS when limited to serous histology. Thus, the prognostic value of MLH1 expression in ovarian cancer is controversial (41). To derive an accurate conclusion, it will be necessary to assess patients with the same clinicopathological factors, such as histological subtype, type of chemotherapy, and type of MLH1 expression (protein or mRNA). To the best of our knowledge, this study is the first report to elucidate an association of MLH1 protein expression with survival in advanced serous ovarian cancer treated with platinum- and taxane-based chemotherapy.
Although all patients with evaluable disease in the low MLH1 expression group showed good responses to platinum- and taxane-based chemotherapy, differences in tumour response rates as evaluated by RECIST were not statistically significant between the low and high MLH1 expression groups. It was difficult to assess the response by RECIST because of the low number of patients who had an evaluable disease. CA125 is well validated as an accurate and reliable means for monitoring the response to chemotherapy in ovarian cancer (37, 38); therefore, we evaluated the association between MLH1 expression and normalisation of CA125 level after platinum- and taxane-based chemotherapy. This analysis showed that the rate of normalisation after platinum- and taxane-based chemotherapy was significantly higher in patients with low MLH1 expression than in those with high MLH1 expression. These results suggest that low MLH1 protein expression may be associated with favourable response to platinum- and taxane-based chemotherapy in advanced serous ovarian cancer.

Representative claudin-4 immunostaining in the cytoplasm and cell membrane of ovarian cancer cells. A: Low claudin-4 expression. B: High claudin-4 expression. Original magnification: 200×.
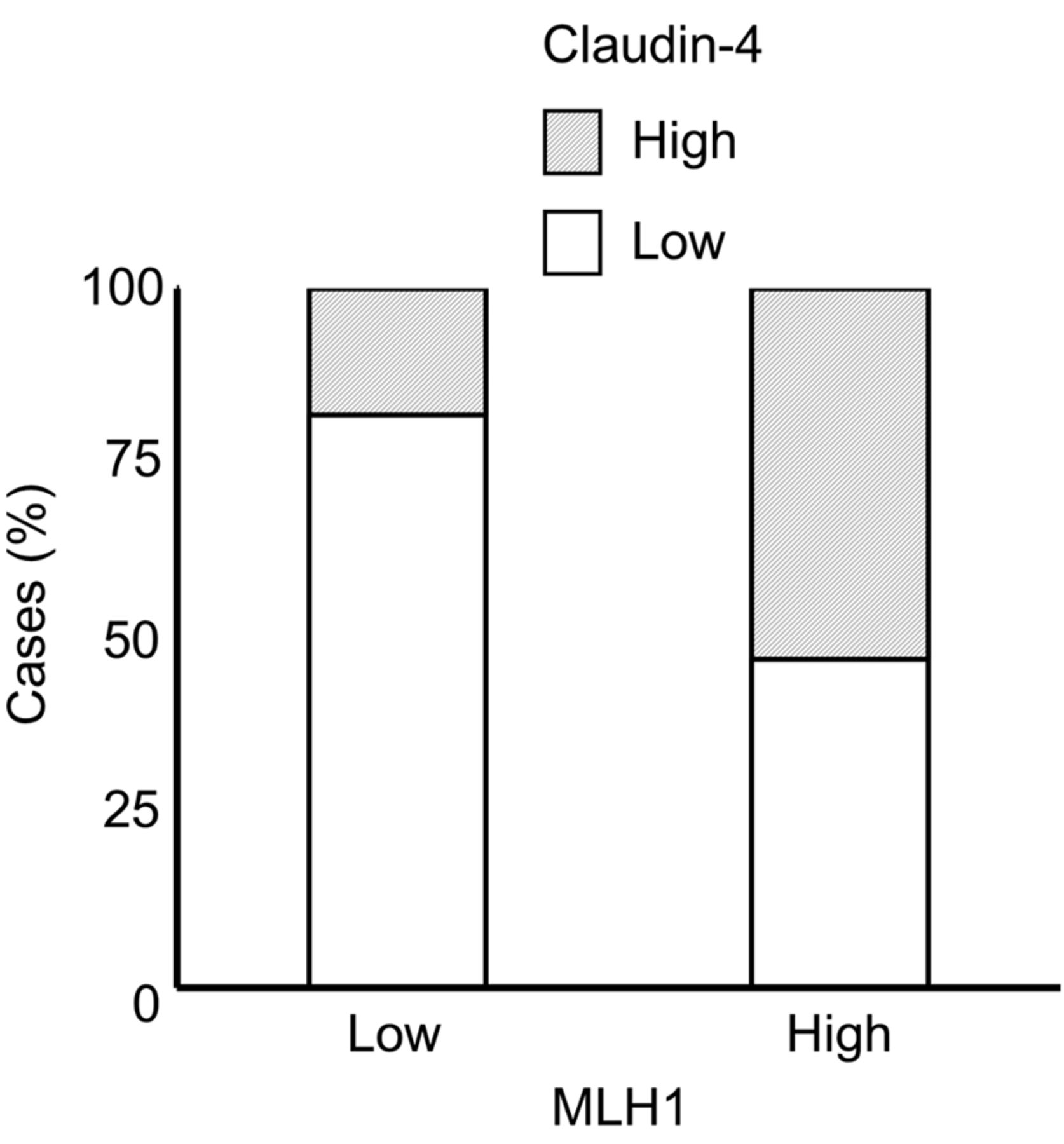
Immunohistochemical determination of the proportion of cases with high/low claudin-4 expression in relation to mutL homolog 1 (MLH1) status. Grey area represents high claudin-4 expression; white area represents low claudin-4 expression. Low claudin-4 expression was found in 82% of cases from the low MLH1 group and 47% of cases from the high MLH1 group (p=0.066).
Only a limited number of studies have investigated the correlation between MLH1 and response to chemotherapy in ovarian cancer. Some previous reports have shown that resistance to platinum-based chemotherapy was associated with loss of MLH1 expression (42-44). However, most of these reports were in vitro studies that evaluated the sensitivity of ovarian cancer cell lines to platinum agents and were not performed using ovarian cancer tissue resected from patients. The relationship between MLH1 expression and response to platinum-based chemotherapy has been evaluated in only a few in vivo studies. Several studies have reported that tumoral MLH1 expression does not predict the response of ovarian cancer to platinum-based chemotherapy (39, 41, 45). Although there are several conflicting reports, MLH1 is expected to be a potential candidate biomarker for predicting chemotherapy response in ovarian cancer. Thus, further studies should be performed with patients who have the same clinicopathological features of ovarian cancer in order to elucidate the correlation between MLH1 expression and chemotherapy sensitivity.
The molecular mechanisms underlying the association of MLH1 expression with survival and chemotherapy response in ovarian cancer have not been identified. MLH1 plays an important role in the repair of various genetic mutations and has been shown to interact with cancer-associated pathways such as apoptosis and other DNA repair molecules (19-21). Ding et al. showed that MLH1 protein expression correlated with X-linked apoptosis protein and regulated the chemotherapy response of ovarian cancer (21). Another study suggested that MLH1 binds to the tumour suppressor BRCA1 and that this interaction is necessary for the cellular response to doxorubicin (19, 46). Additionally, MLH1 protein has been shown to interact with several cytoskeletal scaffolding proteins, such as non-erythrocytic alpha-II-spectrin (SPTAN1) (47-49). Ackermann et al. showed a strong correlation of MLH1 and SPTAN1, and the interaction between MLH1 and SPTAN1 regulates tumour progression (29). Because SPTAN1 is an important factor for cell–cell adhesion and tight junction integrity (28, 50-54), the strong correlation between MLH1 and SPTAN1 suggests a potential role for MLH1 in regulating a tight junction protein. There have also been studies to suggest that MLH1 is correlated with epidermal growth factor receptor (EGFR) mutations (31, 33), and that the expression of the tight junction protein claudin is mediated through EGFR signalling (30, 32). These results also suggest a potential role for MLH1 protein in the regulation of tight junction proteins.
CA125 levels according to mutL homolog 1 (MLH1) expression in evaluable cases.
Claudin is the primary component of tight junctions, and several studies have suggested that claudin-4 is associated with survival and chemosensitivity in ovarian cancer (24-27). Therefore, we evaluated the relationship between MLH1 and claudin-4 expression. In our cohort, claudin-4 protein expression was lower in the group with low MLH1 expression compared to the high MLH1 expression group. Although the difference failed to reach statistical significance, this was most likely related to the low number of patients. In our previous study, we showed that loss of claudin-4 expression was associated with improved response to platinum-based chemotherapy and better prognoses in patients with ovarian cancer (24). These results suggest that claudin-4 may play an important role in the molecular mechanisms through which MLH1 affects survival and chemotherapy response in ovarian cancer. However, this hypothesis must be investigated in detail through further clinical research with more patients and in vitro studies.
A limitation of this study is that it was a retrospective study that included a small number of patients. The low number of patients is assumed to be the cause of failure to reach statistical significance in the comparison of chemosensitivity evaluated by RECIST and claudin-4 expression between those with low and those with high MLH1 expression. Thus, additional studies with more patients are required.
In conclusion, our study confirmed that MLH1 protein expression might be a prognostic marker in patients with advanced serous ovarian cancer who were treated with platinum- and taxane-based chemotherapy. Understanding the associations between MMR status and tumour biology will become increasingly important because of the recent approval of an immunotherapy-based PD-1 inhibitor by the US Food and Drug Administration for patients with MMR-deficient solid tumours. Further research is warranted to validate our observations and identify the molecular mechanisms underlying the associations between MLH1 and the survival and chemotherapy response of patients with ovarian cancer.
Acknowledgements
The Authors thank James P. Mahaffey, Ph.D., from Edanz Group (www.edanzediting.com/ac) for editing a draft of this article.
Footnotes
Authors' Contributions
Study concepts and design: NK and HY. Acquisition of data: NK and MM. Conducting the study: NK and HY. Data analysis and interpretation: NK and HY. Writing, review, and revision of the article: NK, HY and KF. Study supervision: KF. All Authors have read and approved the final article.
Conflicts of Interest
The Authors declare that they have no conflicts of interests.
- Received August 19, 2019.
- Revision received September 3, 2019.
- Accepted September 10, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}