


Abstract
Triple-negative breast cancer (TNBC) is characterized by a lack of expression of estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER2) and unfortunately is not associated with good prognosis. Treatment of breast cancer mainly depends on chemotherapy, due to the lack of specifically approved targeted therapies for TNBC. It is of paramount importance to find new therapeutic approaches, as resistance to chemotherapy frequently occurs. Herein, we present clinical studies published within the last five years, in order to reveal possible targeted therapies against TNBC. We aimed to discuss factors against TNBC, such as tyrosine kinase inhibitors, anti-androgens, poly ADP-ribose polymerase-1 (PARP-1) inhibitors, anti-angiogenic factors, immune checkpoints and histone deacetylase inhibitors (HDACI). Furthermore, the PI3K/AKT/mTOR pathway seems to be a promising field for the development of new anti-TNBC targeted therapies. Data from 18 clinical trials with patients suffering from TNBC were summarized and presented descriptively.
Breast cancer is one of the most common cancers in females, comprising heterogeneous tumors with a variety of biological features, clinical course, prognosis and response to therapy (1, 2). In 2017, triple-negative breast cancer (TNBC) accounted for about 15% of all the new cases of breast cancer in the United States (3-7). Many different epidemiological studies have revealed that TNBC was more likely to arise among females characterized by early menarche, higher waist to hip ratio, higher parity, shorter duration of breast feeding, higher body mass index, and was more common among pre-menopausal patients (8). TNBC is a disease defined by the absence of human epidermal growth factor receptor 2 (HER2) and hormone receptors (HR), specifically the progesterone (PR) and the estrogen receptor (ER) (9) (Figure 1). There are at least 6 different subtypes, which demonstrate different biological behavior, including the basal-like 1 and 2 (BL-1 and BL-2), mesenchymal (M), mesenchymal stem-like (MSL), immunomodulatory (IM), luminal androgen receptor (LAR) and unstable subtype (7, 10).
TNBC is characterized by poorer diagnosis compared to the other types of breast cancer, with a more aggressive clinical behavior (11-14). Central nervous system and visceral metastases appear at higher incidence and in shorter period of time in this specific type of cancer (15-17). In addition, cerebral, hepatic and pulmonary metastases are more frequent in TNBC, than in other luminal subtypes (18, 19). The greatest risk of recurrent disease occurs in the first 2-3 years after diagnosis and is at minimal after 8 years (4, 20, 21). Cytotoxic chemotherapy still remains the main treatment for TNBC disease, along with surgery and/or radiotherapy, although 60% of TNBC patients show minimal or no response to the aforementioned treatment (22-24). Thus, various studies and clinical trials are being conducted, in order to provide new targets and improve prognosis. Androgen targeted therapy, anti-angiogenetic factors, histone deacetylase inhibitors, immune checkpoint inhibitors, PARP inhibitors and the PI3K/AMT/TOR pathway have been proposed as possible targets for the treatment of TNBC (25-34).
The present study provides an up-to-date review which focuses on the progress made in the field of targeted therapies for TNBC in the last five years.
Materials and Methods
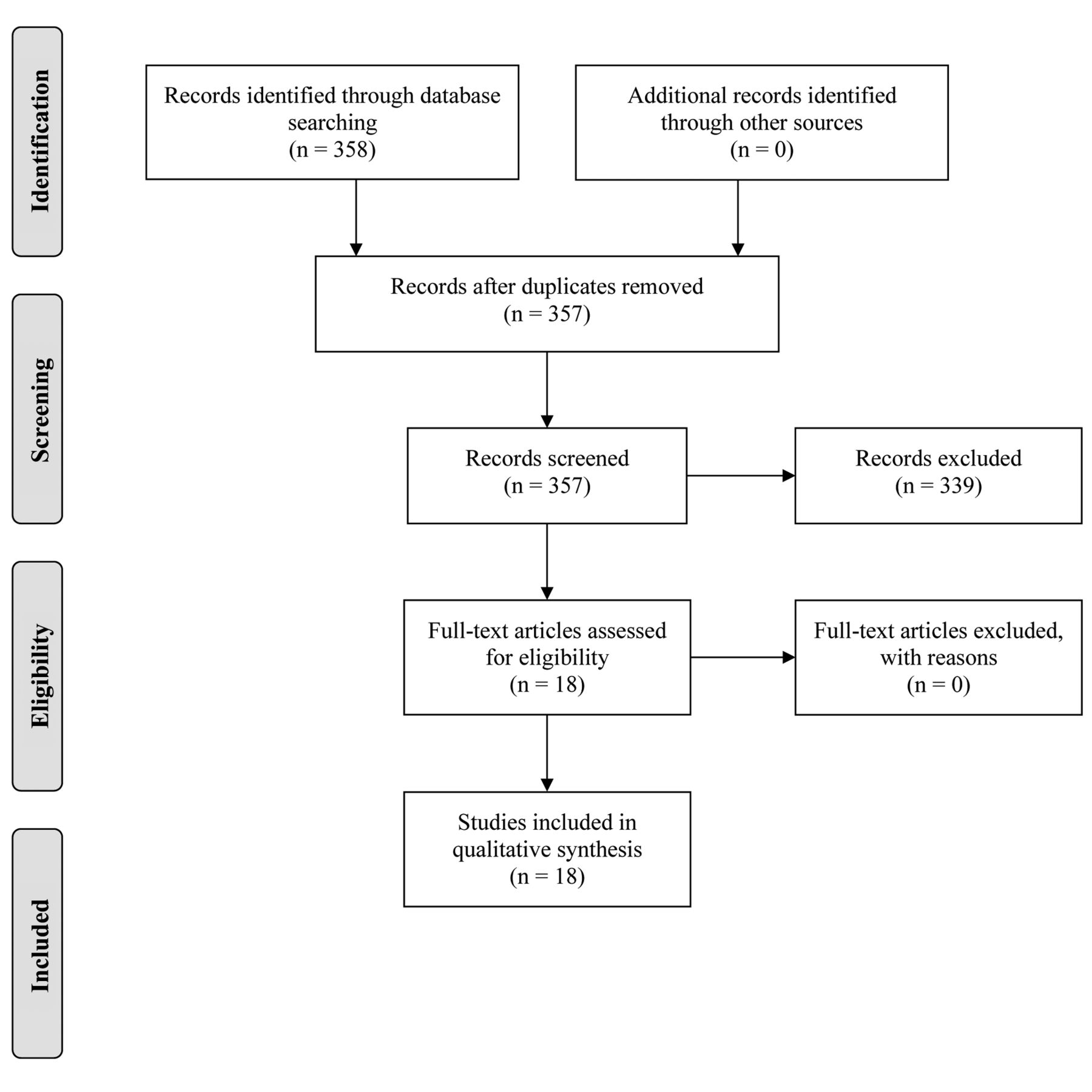
A literature search was conducted in MEDLINE (via PubMed) and COCHRAINE library in order to retrieve articles published during the period between 2015-2019. The search strategy was based on the use of keywords such as triple-negative breast cancer, targeted therapies, clinical trials and metastases. The PRISMA approach was used for the selection of the publications included in the review. A total of 358 records were identified. Following removal of the duplicates 357 records remained. These were screened and 339 were excluded because they were only abstracts or did not include clinical trials. Furthermore, articles were excluded because TNBC patients were neither the only group included, nor were analyzed separately in the clinical study. The full-text articles assessed for eligibility were 18 and none of them was excluded. The inclusion process is presented in Figure 2.
Results
Anti-angiogenic factors. High expression of VEGF has been reported in TNBC (35, 36). VEGF has been shown to induce high tumor cell proliferation in mice models of breast cancer (37). As demonstrated in various clinical and experimental studies, the most significant angiogenic factor for breast cancer is VEGF (35). In human breast cancer, the combination of mutant p53 with high labels of VEGF, is associated with poor clinical outcome (38).
In 2016, Ferrero et al., reported a single-arm multicenter phase II study which included 64 patients with advanced TNBC (Table I, Entry 1). Patients received treatment with 4-week cycles with capecitabine (800 mg/m2 twice on days 1-5, 8-12, 15-19), paclitaxel (80 mg/m2 on days 1, 8 and 15 for maximum of 6 cycles) and bevacizumab (10 mg/kg on days 1 and 14) every 4 weeks until unacceptable toxicity or disease progression. It was shown that this triple regimen had efficient antitumor activity with acceptable levels of toxicity (39).
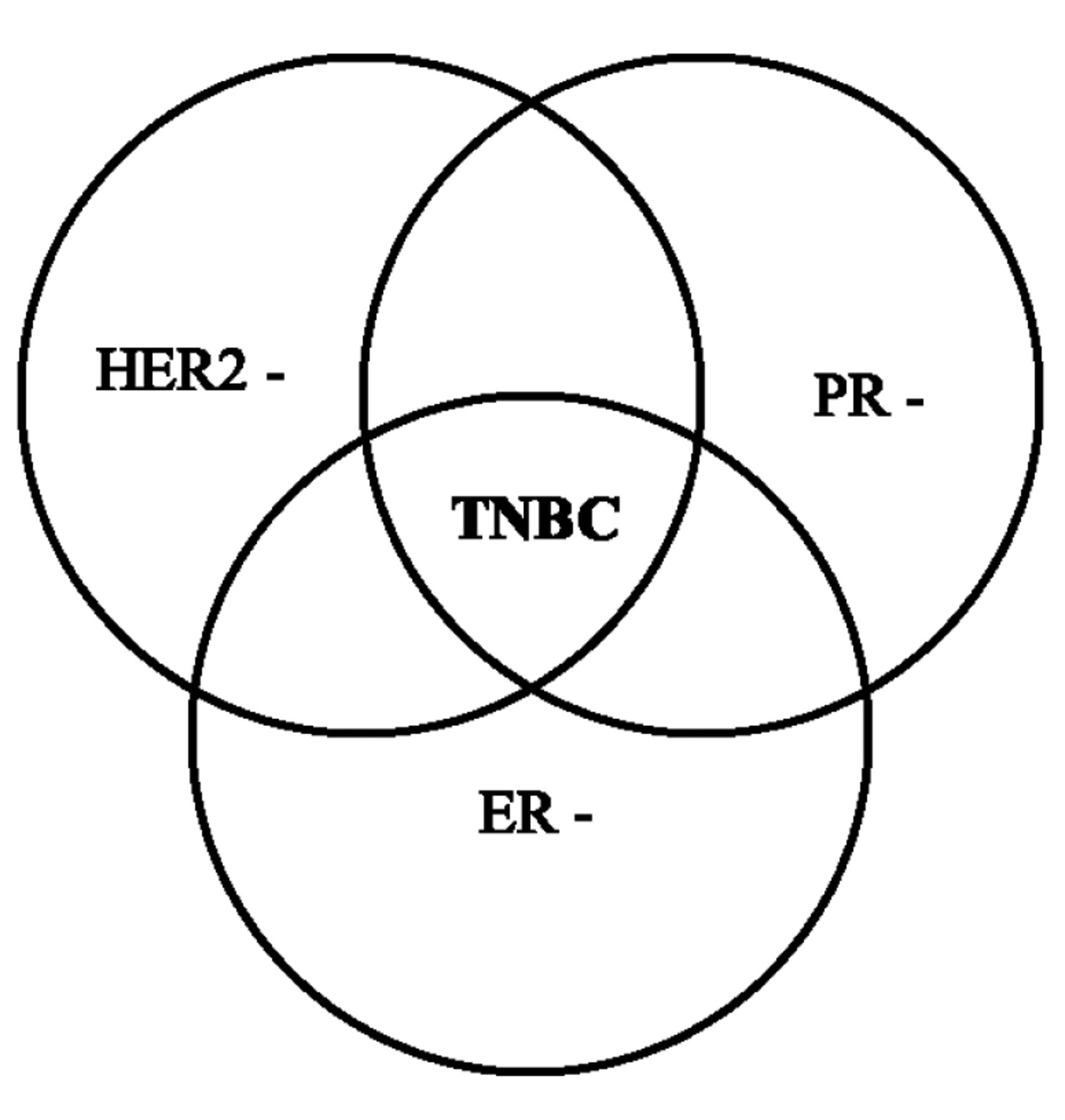
Triple-negative breast cancer. HER2: Human epidermal growth factor receptor 2; PR: progesterone receptor; ER: estrogen receptor; TNBC: triple-negative breast cancer.
In 2016, the results of an international randomized phase III trial of 2,591 female patients with centrally operable primary invasive TNBC was published (Table I, Entry 2). Chemotherapy alone or combined with bevacizumab at a dose equivalent to 5 mg/kg weekly was administrated to patients. Bell's study compared the two treatments and suggested that there is no significant benefit from the addition of bevacizumab in non-advanced TNBC (40).
One year later, a phase II study with 46 patients examined the efficacy of paclitaxel, carboplatin and bevacizumab 10mg/kg intravenous on day 1 and 15 of a 28-day cycle against metastatic TNBC (Table I, Entry 3). It was shown that this regimen offered clinical response without the serious adverse events associated to bevacizumab (24).
In 2018, a phase II clinical trial including 55 female patients, aged between 33 to 83 years old, with invasive TNBC was conducted (Table I, Entry 4). Nabpaclitaxel and 10 mg/kg IV bevacizumab at days 1 and 15, along with maintenance therapy with the same dose of bevacizumab with erlotinib was administered to patients. According to Symonds et al., the combination treatment described above did not increase progression-free survival, as expected, but the maintenance therapy offered a break from chemotherapy (41).

Prisma flow diagram for the current literature review.
Next year, Mery et al., treated 45 female TNBC patients with a median age of 62 years, with paclitaxel plus 10 mg/kg bevacizumab on days 1 and 15 (Table I, Entry 5). According to the results, bevacizumab proved to be beneficial to patients by prolonging median progression-free survival with limited toxicity (42).
Immune checkpoint inhibitors. PD-1 receptor is expressed on the surface of T-reg cells. Both lymphocytes and cancer cells bind to PD-1 via its ligand named PD-L1. PD-L1 is not found in normal epithelial cells (43, 44). Their binding leads to inhibition of T killer cell action against cancer cells and decreased production of inflammatory cytokines. Thus, T killer and cancer cells interact. The inhibitors of PD-1 and PD-L1 inhibit the immune checkpoints mentioned above and improve immune response induced by T killer cells (44).
TNBC expresses relatively high levels of PD-L1, mostly on immune [tumor infiltrating lymphocytes (TILs)] cells and less frequently on cancer cells (45). Thus, TNBC is a perfect candidate for trials with anti-PD-1/PD-L1 agents (46).
Clinical trials with targeted therapies conducted in patients with Triple-Negative Breast Cancer.
In 2016, Nanda et al., conducted a multicohort, nonrandomized, phase Ib study, in which 32 women with positive PD-L1 TNBC, aging between 29 to 72 years old, were enrolled (Table I, Entry 6). Intravenous administration of pembrolizumab at a dose of 10 mg/kg every 2 weeks was found to be clinically efficacious against cancer cells and to have a tolerable safety profile with limited toxicity (47).
One year later, a phase 1 trial evaluated the clinical response of 168 patients with metastatic breast cancer, including 58 patients with TNBC (Table I, Entry 7). Patients received pembrolizumab at a dose of 10 mg/kg every 2 weeks. It was pointed out that, especially in the TNBC population there was a greater antitumor activity without serious adverse events (48).
Next year, a group of 170 female individuals between 28 to 85 years old with metastatic TNBC, who had already received previous chemotherapy treatment, received 200 mg of pembrolizumab intravenously over 30 min every 3 weeks for maximum 2 years (Table I, Entry 8). Patients treated with pembrolizumab, showed significant clinical response with acceptable adverse events (49).
In addition, another phase II study aimed to examine the efficacy and the safety profile of pembrolizumab, as a first-line treatment in 84 individuals diagnosed with PD-L1 positive mTNBC (Table I, Entry 9). According to Adams's study, there was significant evidence that pembrolizumab led to a low incident rate of severe adverse events, with durable and effective antitumor activity (50).
Histone deacetylase inhibitors. Both histone acetylation and deacetylation demonstrate a great effect on chromatin structure and remodeling. According to functional criteria, histone deacetylases (HDAC) can be classified in four classes, which can be divided into two groups, the NAD-dependent class III and the Zn2+-dependent classes of I, II and IV. These classes include a) hydroxamates, b) benzamides c) cyclic peptides and d) aliphatic acids (51). HDAC inhibitors (HDACI) affect a wider spectrum of cellular functions in cancer cells, such as cell proliferation, cell death, gene expression and cell migration (52). In addition, anti-angiogenesis and prevention of glycose metabolism are additional mechanisms of action against cancer cells (53). Importantly, normal cells seem to be relatively resistant to HDACI and be less affected by their actions, providing an opportunity to maximize results against cancer cells and minimize toxicity on healthy ones (52, 53). In 2016, a multicenter phase II study tested the objective response rate of entinostat and 5-azacitidine (AZA) in 40 patients with advanced breast cancer, including 13 with TNBC (Table 1, Entry 10). The clinical results showed that there was no response to treatment provided in women with TNBC (54).
PI3K/AKT/mTOR pathway inhibitors. The aberrations in the PI3K/AKT/mTOR pathway are considered to be common in various subtypes of breast cancer including TNBC (55). In TNBC, overexpression of regulators, such as epidermal growth factor receptor (EGFR), the loss of function of phosphatase and tension homolog (PTEN) or the presence of mutations, which activate the PI3K subunit a, can trigger oncogenic activation of this pathway (56-58). Downstream of PI3K is AKT, which is inhibited by ipatasertib (59). In 2017, Kim et al., conducted a phase II trial, in which 124 women suffering from metastatic or locally advanced TNBC with ECOG performance status <2 participated (Table I, Entry 11). Patients were randomized to paclitaxel plus 400 mg oral ipatasertib or placebo on days 1 and 21 on each cycle (28-days). The period of progression-free survival was longer in patients treated with ipatasertib, than in those treated with placebo. Furthermore, the risk of adverse events grade ≥3 was slightly higher in patients receiving ipatasertib compared to those receiving placebo (60).
Concerning the mTOR inhibitors, in 2016, 52 female patients with metaplastic TNBC participated in a phase I study (Table I, Entry 12). On the first day of every cycle (of 21 days duration) both bevacizumab and liposomal doxorubicin, combined with daily oral everolimus (DAE) or weekly intravenous temsirolimus (DAT), were administered to participants. Both combinations showed remarkable activity against metaplastic TNBC. Additionally, PI3K pathway aberrations were related to improved objective response rate (61).
Next year, investigators tested the use of Cisplatin weekly for 12 weeks, paclitaxel weekly for 11 weeks (administration started 1 week after cisplatin initiation) and everolimus 5 mg orally daily or placebo orally daily for 12 weeks in 145 patients with Stage II/III TNBC and ECOG performance status <2 (Table I, Entry 13). The results revealed that the triple combination therapy, compared to cisplatin/paclitaxel, failed to improve the clinical outcome of patients. In addition, more adverse events occurred (62).
Androgen-targeted therapy. The androgen receptor (AR) is found in both malignant and normal breast tissue and its prevalence varies according to the histological subtype of breast cancer. Approximately 10-15% of TNBC expressing AR show a more benign course (63, 64). In 2018, Traina et al. tested 175 individuals with AR positive, locally advanced or metastatic TNBC. Patients received 160 mg of enzalutamide once daily until disease progression (Table I, Entry 14). The outcome of the prospective phase II study indicated that there was a significant clinical benefit from the use of enzalatumide (65).
Next year, a group of scientists evaluated the efficacy of 1,000 mg of Abiraterone Acetate (four tablets of 250 mg, daily) and 5 mg prednisone twice every day in 34 patients with AR positive, locally advanced or metastatic triple-negative breast cancer (Table I, Entry 15). They showed that administration of abiraterone acetate demonstrated significant clinical benefit after 6 months of treatment. Additionally, the majority of the adverse events were characterized as grade 1 and 2 (66).
Poly-ADP ribose polymerase (PARP) inhibitors. Poly-ADP-ribose synthesis consists one of the primary responses to DNA strand breaks. PARP1, as a stable element of chromatin, accelerates DNA repair via various mechanisms, such as attraction of other repairing proteins and binding to DNA breaks (67-71). PARP inhibitors induce apoptosis, by causing accumulation of damaged cellular DNA. Thus, the inhibition of PARP-1 can cease the procedure or repairment in a single-stranded intermediate state (69, 70, 72).
In 2015, 141 patients with TNBC Stage II-IIIa were evaluated in a phase II study (Table I, Entry 16). The patients were divided into three groups depending on the neoadjuvant regimen received. They were randomized to receive paclitaxel alone (PTX), paclitaxel plus iniparib weekly (PWI), and paclitaxel plus iniparib twice a week (PTI). The investigators demonstrated that pathologic complete response was similar in the three groups and the addition of iniparib increase neither antitumor activity nor toxicity (73).
One year later, a group of 45 patients with metastatic TNBC were enrolled in a randomized phase II study (Table I, Entry 17). They randomly received cyclophosphamide alone or co-administered with veliparib at 60 mg per day in 21-day cycles. According to the results, no improvement was observed to the response rate, after the combination of both drugs, compared to cyclophosphamide alone (74).
Tyrosine kinase inhibitors. MET is a tyrosine kinase receptor, which binds to its ligand hepatocyte growth factor (HGF) (75). Its activation leads to proliferation, survival and invasion of cancer cells and is associated with poor clinical outcome (76-81). Cabozantinib consists an inhibitor of various tyrosine kinases, such as MET and the vascular endothelial growth factor receptor 2 (VEGFR2) (82).
In 2016, Tolaney et al., conducted a phase II study, in which they tested 35 women of median age 50 years with metastatic TNBC (Table I, Entry 18). Cabozantinib 60 mg once per day for 3 weeks in each cycle was administered to participants. Via analysis of blood biomarkers during treatment, they showed that cabozantinib leads to immune system activation and prevents angiogenesis. Thus, cabozantinib showed clinical benefit without adverse events grade >3 even though it did not reach the objective response rate in pre-treated metastatic TNBC patients (83).
Conclusion
TNBC is characterized by great metastatic ability and is associated with poor clinical result. Patients with the TNBC do not benefit from hormonal treatment or treatment with anti-HER2 antibodies (trastuzumab), since their tumors do not express the ER, PR, and HER2 receptors. Surgery, radiation therapy, and chemotherapy, used alone or in various combinations, are currently the primary reliable therapeutic options for patients with TNBC. Thus, it is necessary to conduct studies with specifically selected patient populations, as the TNBC is so heterogeneous. As it is shown in this review, numerous new therapeutic targets have emerged, such as tyrosine kinase inhibitors, antiandrogens, poly ADP-ribose polymerase-1 (PARP-1) inhibitors, anti-angiogenic factors, immune checkpoints and HDACI. In addition, the PI3K/AKT/mTOR pathway is regarded as another evolving field, concerning treatment of TNBC.
In conclusion, as new opportunities emerge from the development of all these potential new targeted therapies against TNBC, more clinical trials should be conducted in order to examine the toxicity profile and the efficacy of the new agents.
Footnotes
↵* These Authors contributed equally to this study.
Authors' Contributions
CD and NG designed the study. CD, AG, KN and NG wrote the article. CD, AG, KN, MV, ED, AP, PF and NG collected the data. AN, DM, NN and KK offered scientific advice. DD, EAA and NG revised the manuscript. NG was the supervisor.
This article is freely accessible online.
Conflicts of Interest
All the Authors declare that there is no conflict of interest regarding this study.
- Received August 4, 2019.
- Revision received September 2, 2019.
- Accepted September 3, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- lncRNA SEMA3B-AS1 Inhibits miR-513c-5p to Regulate the Progression of Triple-negative Breast Cancer
- STAT3 Inactivation and Induction of Apoptosis Associate With Fluoxetine-inhibited Epithelial-mesenchymal Transition and Growth of Triple-negative Breast Cancer In Vivo
- Novel Imidazo[2,1-b]oxazole Derivatives Inhibit Epithelial Cell Transformation and Triple Negative Breast Cancer Tumorigenesis
- The INPP4B Tumor Suppressor Modulates EGFR Trafficking and Promotes Triple-Negative Breast Cancer
- Molecular Classification and Future Therapeutic Challenges of Triple-negative Breast Cancer
- Clinical Imaging of the Heterogeneous Group of Triple-negative Breast Cancer