


Abstract
Background/Aim: To identify the clinical and dosimetric predictors of severe acute radiation esophagitis (RE) in patients with non-small cell lung cancer (NSCLC) treated with accelerated hyperfractionated concurrent chemoradiotherapy (AH-CCRT) with concomitant boost technique. Patients and Methods: A total of 159 patients who underwent AH-CCRT (64 Gy in 40 fractions twice daily) were retrospectively identified. Severe RE was designated as grade 3 or higher according to the Common Terminology Criteria for Adverse Events, version 4.0. Results: The incidence rate of grade 3 RE was 15.1% (24/159). The multivariate analysis that incorporated the Eastern Cooperative Oncology Group performance status (ECOG PS, ≥1 vs. 0) and the relative esophagus volume irradiated with at least 60 Gy (V60) was optimal. Patients with a V60 of ≥15% had a 37.8% risk of grade 3 RE compared to a 6.1% risk among those with a V60 of <15%. Conclusion: ECOG PS (≥1 vs. 0) and the V60 were found to be significant risk factors for severe RE in NSCLC patients who underwent AH-CCRT.
- Radiation esophagitis
- non-small cell lung cancer
- chemoradiation
- accelerated hyperfractionation
- concomitant boost technique
Non-small cell lung cancer (NSCLC) is a major cause of death worldwide. The standard of care for patients with locally advanced NSCLC is definitive concurrent chemoradiotherapy (CCRT); however, the local control rate following this therapy remains poor (1). Although the efficacy of dose escalation is unclear, treatment using accelerated hyperfractionated radiotherapy (AHRT) was previously shown to improve local control and overall survival (OS) (2-4). A phase 2 study and a propensity matched analysis showed that accelerated hyperfractionated concurrent chemoradiotherapy (AH-CCRT) (64 Gy in 40 fractions twice daily) resulted in an excellent response rate and OS (5, 6).
Approximately 10-20% of patients undergoing CCRT will experience severe radiation esophagitis (RE) (1, 7, 8). The symptoms include retrosternal pain, dysphagia and odynophagia. Assessing the risk of severe RE is a critical step in choosing treatment intensification strategy using AH-CCRT, as severe RE often leads to the interruption of treatment (9), which spoils the advantage of shortened radiation treatment time (RTT) of AH-CCRT regimens. Clinical and dosimetric risk factors for RE reported from standard once-daily regimens cannot necessarily be applied to twice-daily regimens. In this study, we sought to identify clinical and dosimetric factors for severe RE in a cohort of patients with NSCLC treated with a twice-daily AH-CCRT regimen.
Materials and Methods
Patient population and pretreatment evaluation. After institutional review board approval (No.1606309044) was obtained, a retrospective review was performed. A total of 159 patients with NSCLC treated with AH-CCRT were identified between 2004 and 2017. Clinical factors included sex, age, Eastern Cooperative Oncology Group performance status (ECOG PS), body mass index (BMI), treatment period, N classification and chemotherapy status (including chemotherapy cycle upon concurrent RT commencement, consolidation chemotherapy use and the concurrent chemotherapy regimen). The clinical stage was not included because the edition (the 6th or 7th) of the Union for International Cancer Control (UICC) that was used for staging could not be determined in some patients. The N classification was included because it did not change between the 6th and 7th editions of the UICC. BMI was defined as weight in kilograms divided by the square of height in meters. Patient characteristics are presented in Table I.
RT technique. All patients were treated with 3-dimensional conformal RT. The planning technique was based on the International Commission on Radiation Units and Measurements, report 62 (10). The gross tumor volume (GTV) was defined as the primary tumor and metastatic nodes. The clinical target volume (CTV) consisted of the high-risk CTV (CTV1: GTV plus a 5-mm margin) and elective CTV (CTV2: CTV1 plus elective nodal areas of the mediastinum). The CTV1 and CTV2 were expanded by 5 mm to define the planning target volumes (PTV1 and PTV2). Organs at risk were contoured on the expiratory scan. Typical field arrangements consisted of 4 beams, usually anterior-posterior opposed fields for PTV2 and oblique opposed fields for PTV1. The concomitant boost was defined as the boost irradiation for PTV1, which in standard once-daily RT is typically started after the end of irradiation for PTV2, but was instead started at the beginning of the treatment. The prescribed dose was 64 Gy over 4 weeks with the concomitant boost technique (phase 1: 40 Gy/20 fractions for PTV2; phase 2: 24 Gy/20 fractions as a second daily fraction after a 6 hours gap for PTV1) (5). Radiation was delivered between Monday and Friday. Holiday- and machine maintenance-associated days off were considered treatment breaks.
Esophageal contouring and dosimetric parameters. For consistency, the esophagus was re-delineated in all patients by the same radiation oncologist (K.W.). The esophageal contour extended from the inferior margin of the cricoid cartilage superiorly to the gastroesophageal junction inferiorly. The esophageal contour was not expanded to account for setup variability. Dosimetric analyses included reporting the maximal esophageal dose (Dmax), mean esophageal dose (Dmean), esophageal volume (in cm3), and the relative volume of the esophagus receiving at least × Gy (V10-60). Based on the hypothesis that length is important when predicting severe RE, the lengths of the esophageal sections receiving at least the mean dose of × Gy (L10-60) were also calculated.
Chemotherapy. Cisplatin (80 mg/m2) on day 1 combined with vinorelbine (25 mg/m2) on days 1 and 8 in 3- to 4-weeks intervals were delivered as concurrent chemotherapy in 114 patients, and carboplatin plus paclitaxel were administered to 36 patients with comorbidities. Six patients received both cisplatin and carboplatin with varying cycles, 1 received cisplatin plus docetaxel, and 2 received cisplatin plus S-1. RT commenced with the first chemotherapy cycle in 52.8% of the patients and with the second or third cycle in 47.2%. Consolidation chemotherapy was administered to 77.4% of the patients.
Esophagitis scoring and follow-up. RE was retrospectively graded according to National Cancer Institute's Common Terminology Criteria for Adverse Events version 4.0 from the start of RT until 3 months afterward. Severe acute RE was designated grade 3 or above. Evaluation for acute toxicity during the treatment course was performed once a week or more frequently when interventions were indicated. The first follow-up clinical evaluation was performed 1-2 weeks after completion of RT and every 1-3 months thereafter.
Patient characteristics.
Statistical analysis. Clinical and dosimetric factors were analyzed to determine the risk factors associated with the development of grade ≥3 RE. First, univariate analyses were performed to identify any significant risk factors from among the following: sex, age, ECOG PS, BMI, treatment period, N classification, chemotherapy status, and dosimetric parameters (including Dmax, Dmean, the relative volumetric variables [V10, V20, V30, V40, V45, V50, V55, and V60] and the absolute length variables [L10, L20, L30, L40, L50, and L60]). The chi-square test was used to confirm independence among clinical factors. Pearson's analysis was performed to calculate the correlation between dosimetric factors. Secondly, multivariate analyses of significant (p<0.05) and marginally significant (p<0.1) factors were performed using a multiple logistic regression model. The Akaike information criterion (AIC), which balances the goodness of fit with the complexity of the model, was used for backward model selection of the dosimetric parameters. The preferred model was that exhibiting the lowest AIC value. Additionally, receiver operating characteristic (ROC) curves were used to identify cutoff values for dosimetric predictors. All statistical tests were 2-sided. JMP Pro version 10 (SAS Institute Inc., Cary, NC, USA) was used for the statistical analysis.
Univariate analysis of clinical and dosimetric factors associated with radiation esophagitis.
Results
Of the 159 patients included in this study, 81.8% were men and 18.2% were women; their median age was 63 years (range=34-79 years). Of these patients, 151 were receiving their first treatment while 8 were receiving salvage RT for regional lymph node recurrence after surgery. The incidence rate of grade 3 RE was 15.1% (24/159); no grade 4 or 5 RE was observed. The median time to RE onset upon commencing RT and the median duration of RE were 26 (range=16-52 days) and 11 days (range=3-23 days), respectively. Furthermore, 26 of 135 patients with RE grade <3 (19.3%) experienced treatment delays of over 5 days during RT, whereas 13 of 24 patients with RE grade 3 (54.2%) experienced such delays. Patients who were ≥70 years tended to commence RT with the first chemotherapy cycle (p=0.04); moreover, a weekly carboplatin + paclitaxel regimen was more prevalent (p=0.035). No other associations were detected among the clinical factors.
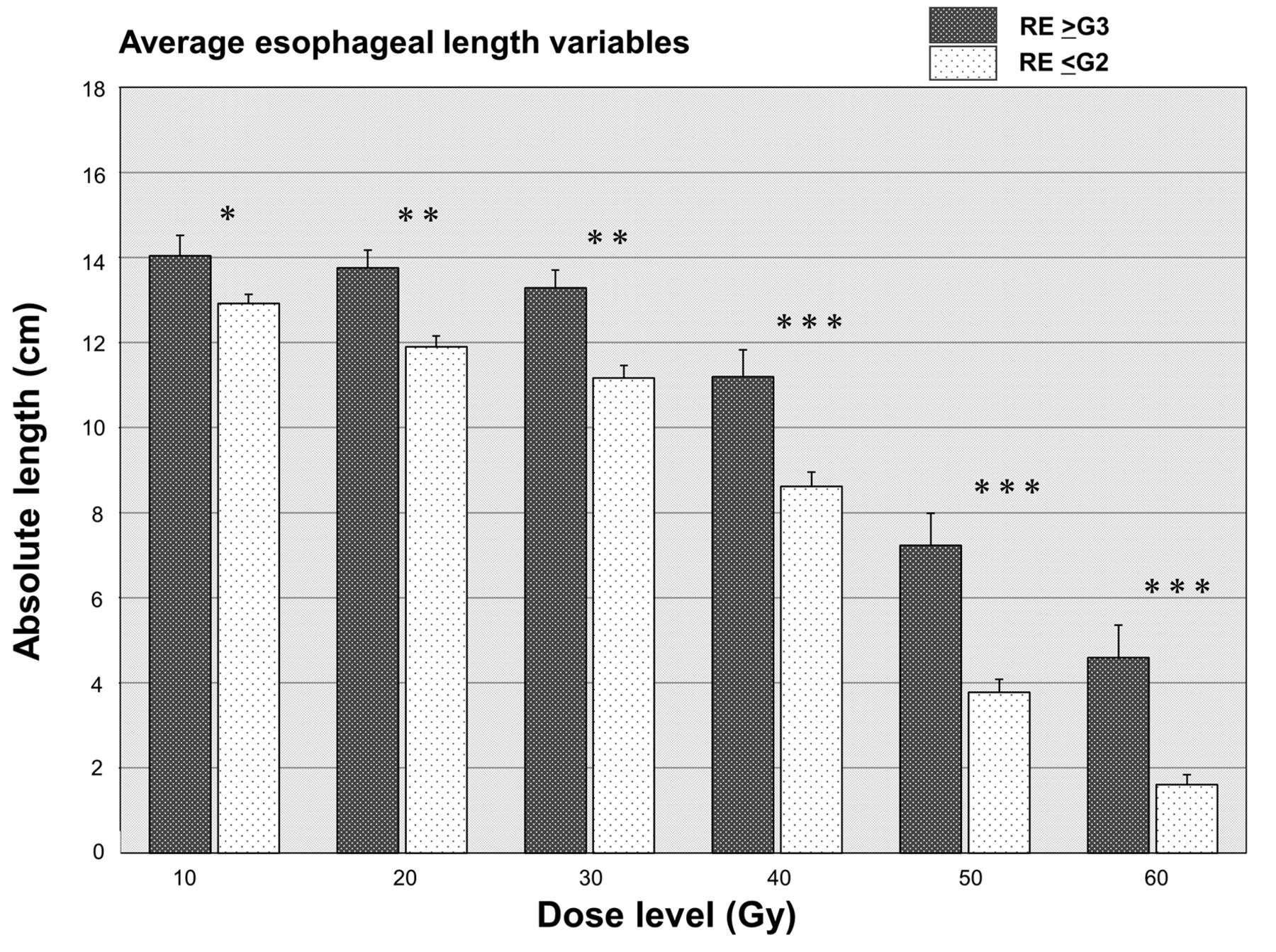
On univariate analysis, only ECOG PS (≥1 vs. 0) was a significant factor for grade 3 RE. Sex, age, BMI, treatment period, N classification and chemotherapy status were not significant factors. The dosimetric parameters, Dmax, Dmean, relative volumetric variables (V10-60) and absolute length variables (L10-60) were all significantly correlated with grade 3 RE. The average Dmean and Dmax of grade ≤2 RE and grade ≥3 RE were 22.7 Gy vs. 29.1 Gy (p<0.0001) and 61.2 Gy vs. 64.8 Gy (p=0.007), respectively. Associated odds ratios (ORs) are shown in Table II. The average esophageal volume variables are shown in Figure 1 and the average esophageal length variables are shown in Figure 2.
Multivariate analysis was performed on the dosimetric variables and ECOG PS (1≥ vs. 0). Spearman's correlation coefficient test did not show any associations between the dosimetric variables and ECOG PS. Because of the multicollinearity between dosimetric variables, which was confirmed by Pearson's analysis, the multivariate analysis was applied separately for each dosimetric parameter. The AIC values of the logistic models with ECOG PS and each dosimetric parameter are shown in Table III. All models demonstrated a significant correlation between grade 3 RE and the predictor variables. The length metrics (L10-L60) had higher AIC values than the corresponding value for Dmean and volume metrics. The model containing ECOG PS and V60 was optimal with the lowest AIC value of 105.9. An ECOG PS ≥1 (OR: 5.1, 95% confidence interval (CI)=1.78-14.6) and a larger V60 (OR for change of 10% relative volume: 2.45, 95%CI=1.64-3.64) significantly increased the risk of grade 3 RE. On the ROC curve analysis, the area under the ROC curve was 0.79 (95%CI=0.69-0.90). This curve and the corresponding AUC showed that the V60 had a moderate predictive ability for grade 3 RE; a V60 of <15% produced a 6.1% occurrence rate for grade 3 RE, which increased to 37.8% if the V60 was ≥15%.

Average esophageal volume variables for patients with radiation esophagitis of grades ≥3 (RE ≥G3) and patients with RE ≤G2. The error bars denote the 95% standard error. Both groups were compared at each dose level using a two-sided Student's t-test (*p<0.05, **p<0.01, ***p<0.001).
Akaike information criterion scores of the models.

Average esophageal length variables for patients with radiation esophagitis of grades ≥3 (RE ≥G3) and patients with RE ≤G2. The error bars denote the 95% standard error. Both groups were compared at each dose level using a two-sided Student's t-test (*p<0.05, **p<0.01, ***p<0.001).
Discussion
Both CCRT and AHRT are associated with a relatively high incidence rate of severe acute RE (1, 3, 7, 8, 11). From the biological viewpoint, the 2-Gy equivalent dose (EQD2) of the current AH-CCRT regimen (64 Gy/40 fractions/4 weeks) was 62.4 Gy, calculated by the linear-quadratic model with α/β=10 (12). However, the time factor was not considered in this calculation. Regarding esophagitis, the particular dose recovered per day was reported to be 0.8 Gy/day (13). The shortened RTT of 2 weeks (6 weeks to 4 weeks) can correspond to a 11.2 Gy dose escalation in EQD2 (α/β=10 Gy), and the calculated EQD2 add up to 73.6 Gy for the esophagus.
The incidence rate of grade ≥3 RE in our study was 15.1% (24/159), which was relatively low despite a higher daily radiation dose (3.2 Gy/day). Byhardt et al. reported a 34% incidence rate of severe acute RE following hyperfractionated RT (69.6 Gy for 6 weeks twice daily) compared to 6% for once-daily chemoradiotherapy, and 1.3% for standard once-daily RT alone (11). Nyman et al. reported the higher incidence rate of severe RE with a twice-daily AH-CCRT regimen (64.6 Gy for 4.5 weeks with one week treatment break) compared to a once-daily regimen (16.3% vs. 9.8%) (14). Possible explanations include the fact that all our patients were treated with a concomitant boost technique. Particularly because most of the esophagus was not exposed to the second fraction of 1.2 Gy (phase 2), an AH-CCRT protocol using a concomitant boost technique can be less toxic than the hyperfractionated or accelerated hyperfractionated radiotherapy protocols.
Dose-volume histogram parameters that delineate cumulative dose over 40-50 Gy have been identified as being associated with severe RE in standard once-daily regimens (8, 15). An individual meta-analysis found that the V60 was the best predictor; a V60 of <0.07% was associated with a <5% risk of grade ≥3 RE, whereas a V60 of ≥17% conferred a 22% risk of grade ≥3 RE (8). Our results, which are consistent with these findings, suggest that the risk of developing grade ≥3 RE depends on the volume of the esophagus that is irradiated at a high dose (such as 60 Gy) even when the AH-CCRT regimen is used. The incident rate of 37.8% in the patients whose V60 was ≥15% in this study was relatively high compared to 22% of those with a V60 of ≥17% reported in the meta-analysis (8). This difference might depend on the shortened RTT. The value of V60 ≥15% in this study can correspond to a higher dose intensity in the conventional RT regimen. The AIC value for the Dmean was slightly worse than that for the V60, but was almost equivalent. The phase III intergroup Radiation Therapy Oncology Group 0617 trial recommended that the Dmean be maintained at <34 Gy and that the V60 be calculated separately for each patient enrolled in the trial (7). We concur that a single consensus dosimetric constraint is insufficient to limit the risk to the esophagus. The length and volume parameters are conceptually distinct about whether we must delineate the entire esophagus or not. The length of the irradiated esophagus, as well as that of the irradiation field, are reportedly predictors of RE (16, 17); however, there is no consensus regarding the method of measurement of these parameters. The volume parameters had a better AIC value than the length of the esophagus in our study, although their advantage over volume metrics is unclear.
Patient characteristics associated with higher rates of severe acute esophagitis include age ≥70 years (18), female sex (19), poor initial PS (19), low BMI (19) and (potentially) pretreatment dysphagia (19). In this study, only ECOG PS was significant. It seemed that the large impact of dose parameters on the occurrence of RE masked the potentially existing association between clinical characteristics and severe RE. In terms of ECOG PS, this result suggests that a good general condition renders the threshold of intervention for RE high. With respect to patient age, Soni et al. reported a lower incidence of RE in elderly patients undergoing definitive CCRT for NSCLC even after adjusting for chemotherapy administration (OR=0.93; 95%CI=0.88-0.98) (20); their results were similar to ours. Although the intensity of chemotherapy may affect the incidence of RE in elderly patients undergoing concurrent treatment, they nevertheless appear to tolerate the AH-CCRT regimen, and should be offered the same options as younger patients if they maintain a good PS. Our chemotherapy regimens normally comprise cisplatin plus vinorelbine and carboplatin plus paclitaxel. Different chemotherapy regimens such as cisplatin plus docetaxel are also frequently used; such differences may influence the incidence rates of RE.
A limitation of our study was its retrospective design, which may have introduced selection bias into the dataset. In addition, patterns of care for adverse events may have changed in the long observation period. Therefore, the incidence rate of RE could not be universally applicable. Despite this limitation, the advantages of our study include the relative homogeneity of the RT regimen compared to previous studies.
While the AH-CCRT with a concomitant boost technique is one of the reasonable ways to escalate treatment intensity for NSCLC patients, pretreatment risk assessment of severe RE is essential. ECOG PS (≥1 vs. 0) and the V60 were found to be significant risk factors for developing severe RE. Validation of our findings in a large independent patient cohort is warranted.
Footnotes
This study was presented in part as poster at the 59th Annual Meeting of the American Society for Radiation Oncology, San Diego, CA. September 2017.
Conflicts of Interest
The Authors declare no conflicts of interest regarding this study.
- Received November 21, 2018.
- Revision received November 28, 2018.
- Accepted November 29, 2018.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}