


Abstract
Background/Aim: Quality of life (QOL) is becoming increasingly important to appraise the value of a particular oncologic intervention. This was a prespecified secondary analysis of a randomized trial (NCT02832830) of intensity-modulated radiotherapy (IMRT) versus conventional three-dimensional conformal radiotherapy (3DCRT) as part of palliative management of symptomatic spinal metastases. This study examined QOL, fatigue, emotional distress, and late toxicities between patients having received IMRT versus 3DCRT. Materials and Methods: Sixty patients were enrolled in this single-institutional randomized exploratory trial in which all patients received 30 Gy in 10 fractions. The EORTC QLQ-BM22, EORTC QLQ-FA13, and QSC-R10 questionnaires were utilized to evaluate QOL, fatigue, and emotional distress, respectively; endpoints were evaluated at baseline, and at 3, and 6 months. Late (6 months) toxicities were assessed according to the LENT-SOMA criteria. Results: Mean follow-up was 192 days (IQR=77-285). Although QOL was similar between groups, patients in the IMRT arm experienced lower physical (p=0.011) and emotional (p=0.017) fatigue at 6 months. Emotional distress was also lower in IMRT-treated patients after six months (p=0.039). Cohen's effect size confirmed the clinically significant improvement of these findings. Late toxicities occurred infrequently and were similar between arms. Conclusion: This is the first randomized study evaluating QOL between IMRT and 3DCRT to palliate vertebral metastases. IMRT resulted in reduced physical and emotional fatigue as well as emotional distress. IMRT should be further studied for these patients given these outcomes.
Spinal metastases occur in up to 40% of advanced-stage cancer patients and can be a major cause of quality of life (QOL) and symptomatic deterioration (1). These include pain, immobility, neurological deficits, and pathological fractures; additionally, fatigue (associated with disease and therapy) occurs in over two-thirds of patients and has a major QOL impact (2-4).
Historically, three-dimensional conformal radiotherapy (3DCRT) has been the technique of choice for palliation (5, 6). However, advanced technologies such as intensity-modulated radiation therapy (IMRT), often implemented with image guidance, are more conformal and result in lower doses to nearby organs-at-risk (OARs). A number of studies have demonstrated the advantages of IMRT in both curative and palliative settings for various cancers (7-11). A prospective non-randomized study of patients with head and neck cancer found improved QOL in IMRT patients compared to patients treated with 3DCRT (12). However, the impact of multi-fraction IMRT on QOL in patients with spine metastases has not been investigated in prospective randomized studies to date. This is important to perform, as QOL is becoming increasingly important to appraise the value of a particular intervention (13-15).
This was a prespecified secondary analysis of a randomized trial of IMRT versus conventional 3DCRT as part of palliative management of symptomatic spinal metastases. This study examined QOL, fatigue, emotional distress, and late toxicity between patients having received IMRT versus 3DCRT.
Materials and Methods
Trial design and participants. The randomized trial, registered on Clinicaltrials.gov (NCT02832830), was approved by the Heidelberg University Independent Ethics Committee (Number S-238/2016). Details of the study design have been published previously (16). Briefly, a block randomization approach (block size of 6) was used to ensure that both groups were balanced. The primary endpoint of this randomized, single-institutional, pilot trial was 3-month RT-induced toxicity following delivery of 30 Gy in 10 fractions of image-guided IMRT versus conventional 3DCRT in patients with previously untreated spinal metastases. All patients had an established indication for RT, including pain and/or neurological deficits. The present investigation was a prespecified secondary analysis regarding QOL, emotional distress and late toxicity at 6 months after RT.
Inclusion criteria were ages 18-85, a Karnofsky performance score ≥50 (ECOG ≤2), and ability to provide written informed consent. Exclusion criteria were significant neurological or psychiatric disorders precluding informed consent, receipt of prior RT to the same site, or radiosensitive (multiple myeloma or lymphoma) histologies. Number or location of metastases were not specific inclusion or exclusion criteria, nor was the presence of spinal cord compression.
Assessment of endpoints. Per protocol, QOL, fatigue, and emotional distress were assessed at baseline and at 3 and 6 months after RT. These comprised of the documentation of patient-specific data and the following questionnaires: EORTC QLQ-BM22, EORTC QLQ-FA13, and QSC-R10.
The QOL endpoint was quantified using the well-validated EORTC QLQ BM22 questionnaire, which is specifically designed for patients with bone metastases. This questionnaire (range=0-100) comprises 22 items and four scales for the measurement of pain in various body areas (painful sites), pain characteristics (persistent pain, recurrent pain), functional impairment (pain when performing various activities, interference with everyday activities), and psychosocial aspects (family, worries, hope) (17, 18).
Fatigue was assessed using the EORTC QLQ FA13 (range=0-100) questionnaire. This includes 13 items and five scales for measuring cancer-related fatigue (19), with subscales covering physical, emotional, and cognitive fatigue, along with interference with daily life, and social sequelae.
Emotional distress was evaluated using the QSC-R10 (range=0-50) questionnaire (20). This module is a valid and reliable questionnaire for determining emotional distress and anxiety in cancer patients (21). The questionnaires were filled out by the patients at the study site.
Lastly, late side-effects were captured according to the Late Effects of Normal Tissue – Subjective, Objective, Management and Analytic (LENT-SOMA) criteria.
Radiotherapy. CT simulation was performed with custom immobilization using Aquaplast® (Aquaplast Corporation, Wyckoff, NJ, USA) head masks for cervical spine cases and Wingstep/ Prostep® (Elekta, Stockholm, Sweden) devices for thoracolumbar cases. In addition to OARs (dose constraints for which were per QUANTEC recommendations), the clinical target volume (CTV) was delineated on the planning CT and encompassed the affected vertebral body or the whole sacrum for sacral lesions (22). The planning target volume (PTV) was an isotropic 1 cm expansion of the CTV and was to be covered by the 90% isodose line. The prescription dose for both cohorts was 30 Gy in 10 fractions.
The IMRT group received image-guided (mega- or kilo-voltage cone beam computed tomography) RT by means of step-and-shoot IMRT, VMAT (Elekta Versa HD accelerator), or helical TomoTherapy (Accuray Inc., Madison, WI, USA). The 3DCRT cohort was most commonly delivered with two or three anteroposterior 6 MV individually-formed beams. Position verification was applied by weekly kilo-voltage CT and before each fraction by comparing orthogonal portal images with digitally reconstructed radiographs from the planning CT.
Statistical analyses. On account of the explorative character of this study it was not possible to estimate the total number of cases; however, with 30 patients per group, it was possible to detect a standardized effect (Cohen's d) of about 0.8 with 80% power and a significance level (α) of 5%.
All variables were analyzed descriptively by tabulation of the measures of the empirical distributions. According to the scale level of the variables, means, standard deviations, medians, as well as minimum and maximum (or absolute and relative frequencies) were reported. Additionally, for variables with longitudinal measurements, the time courses of individual patients are summarized by treatment groups. Descriptive p-values of the corresponding statistical tests comparing treatment groups were given. The Wilcoxon signed rank test was used to compare differences. Cohen's effect size (ES) was assessed for clinically relevant changes in questionnaire measures (<0.3 low, 0.3-0.7 moderate, >0.7 strong differences).
Finally, we compared the groups regarding overall and bone survival using Kaplan–Meier estimates and log-rank tests. All statistical analyses were performed with SAS software v 9.4 (SAS Institute, Cary, NC, USA).
Results
From November 2016 to May 2017, 60 patients were randomized. No patients were excluded post randomization. Baseline characteristics were balanced between the two treatment arms (Table I, as previously published (23).
Although all but one surviving patients completed all assessments, not all patients survived by the three and six-month time periods. Within the first 3 months, 10 patients (33.3%) in the IMRT group had died, along with 11 patients (36.7%) in the 3DCRT arm. Between 3 and 6 months, another 2 patients (10%) died due to tumor progression in the IMRT cohort, along with a further 7 patients (36.8%) in the 3DCRT arm (Figure 1). The mean follow-up was 192 days (IQR 77-285) for both groups.
Baseline characteristics of randomly assigned participants. Explanation: Others: carcinoma of unknown primary (CUP), gastrointestinal stromal tumor (GIST), melanoma, mesothelioma, pancreatic cancer, renal cancer.
QOL was evaluated by means of the EORTC QLQ-BM22 module. Therein, there were no significant differences between cohorts in terms of painful sites, pain characteristics, psychosocial aspects or functional impairment (Table II).
Evaluation of fatigue using the EORTC QLQ FA13 module revealed no differences between groups (at either 3 or 6 months) with regard to interference with daily life and social sequelae (Table III). However, after six months, patients in the IMRT arm had significantly lower physical (p=0.011) and emotional fatigue (p=0.017). Cohen's ES confirmed the clinically significant improvement in these parameters (ES 1.08) and (ES 1.03), respectively.
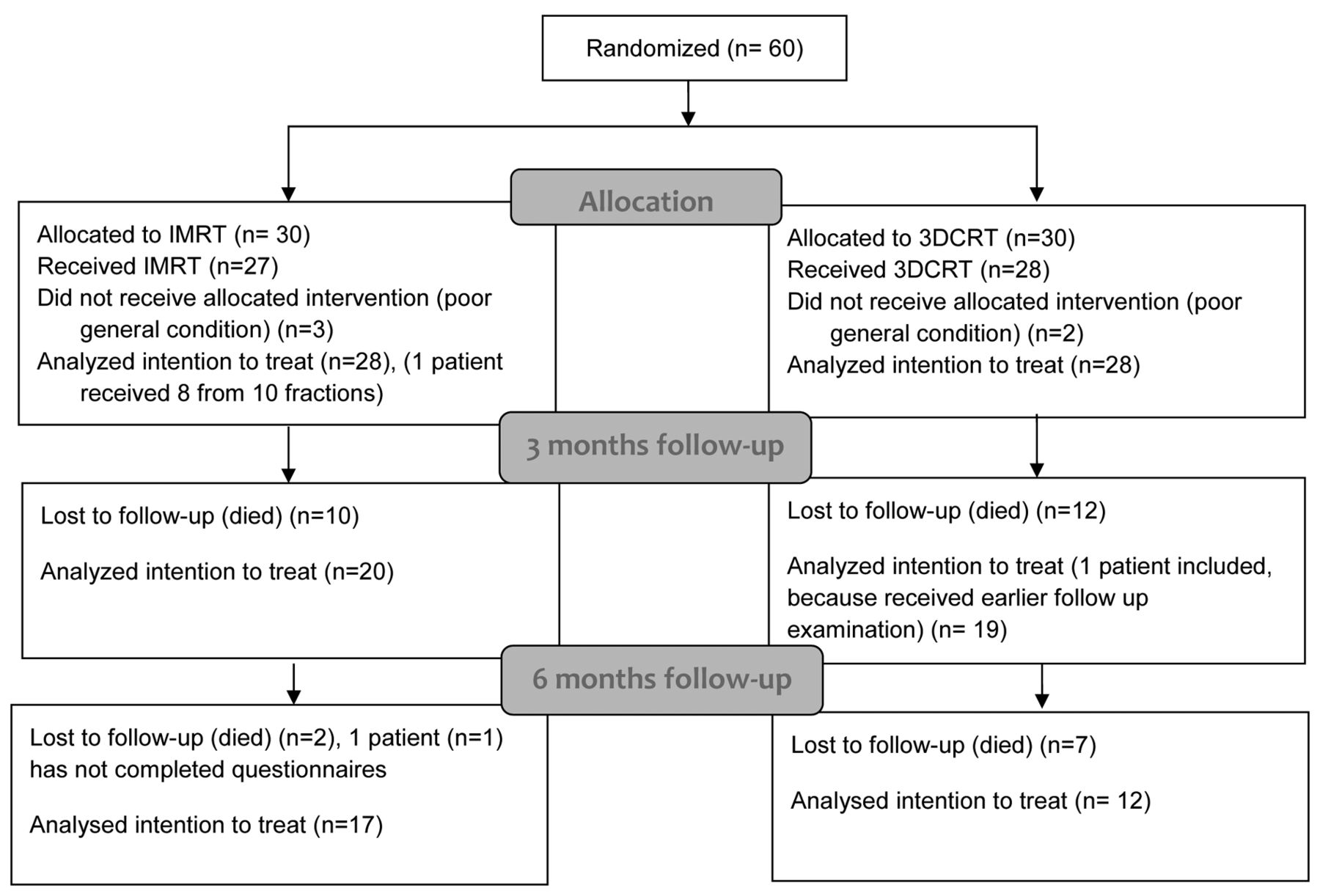
CONSORT diagram of the trial.
Emotional distress, as measured by the QSC-R10 module was similar at three months, but superior in the IMRT group at six months (p=0.039) (Table IV). Cohen's ES (0.93) confirmed these findings as well.
Additionally, late toxicity profiles at 6 months were examined according to LENT-SOMA criteria. The most frequent side-effects in the IMRT group were grades 1-2 such as dyspnea (n=3, 16.7%) and parasthesia (n=2, 11.1%). In contrast, the most frequent side-effects in the 3DCRT group were grades 1-2 esophagitis, diarrhea, radiculitis, myositis, and myalgia (n=2, 16.7% each) (Table V). In total only one participant (5.6%) in the IMRT arm reported grade 3 radiculopathy. No grade ≥4 adverse events occurred in either group. No significant differences in late toxicity were observed between groups.
Discussion
Maintaining QOL in patients with advanced malignancies is of paramount importance. QOL impairment occurs not only by disease itself, but also by therapeutic interventions and their sequelae. For instance, patients with painful spinal metastases may suffer from not only neoplastic pain, but also from side effects of interventions and analgesics. Radiotherapy can reduce pain and thus reduce analgesic consumption, which can be reflected in increased QOL profiles (24). Thus, choosing optimal therapy modalities and techniques in the palliative situation is crucial (25).
This is the first randomized study to illustrate the effect of IMRT on reducing physical and emotional fatigue as well as emotional distress.
More than half of patients with advanced tumors suffer from moderate fatigue before commencing radiation therapy (24). To this extent, reduction of further treatment-related fatigue is essential. Herein, the substantial improvement in physical (p=0.011) and emotional fatigue (p=0.017) at 6 months is consistent with other data from our group showing similar improvements in physical fatigue after 6 months with training of paravertebral muscles during RT (26). Although it is theoretically possible that higher conformality decreases damage to normal tissues, which in turn would decrease fatigue, there are few prospective data to confirm this statement. However, dose-fractionation regimens have been shown to be more robustly associated with fatigue (27), and the fact that all patients received 30 Gy in 10 fractions would imply that fatigue may be more equivalent between cohorts than numeric/statistical values suggest.
Effects on QOL (EORTC QLQ-BM 22).
Furthermore, psychosocial distress, depression, and anxiety are particularly prevalent in advanced disease stages (28), with clinical depression and anxiety ranging from 20-39% (29). Oncological patients undergoing radiation therapy are at high risk for these mental health disorders; over half of patients may be on antidepressants or anxiolytics before the start of RT (30). To this extent, it is noteworthy that emotional distress was lower in the IMRT group at six months (p=0.039), which are in concord with results by Rief and colleagues (26).
There were no significant QOL differences between both groups, which are consistent with established data from our group (26). Nevertheless, it is intuitive that, with similar dose-fractionation schemes in both cohorts, the QOL corresponding to painful sites, pain characteristics, and functional interference would be statistically similar. As with several of the aforementioned measures, however, this parameter greatly depends on the precise nature of patient-physician communication as well as a host of several other factors that could confound conclusions in this and any other QOL or patient-reported outcome analysis (31).
Lastly, regarding the equipoise of late toxicities between arms (but with more significant differences in acute events (23) implies that even acute toxicities have lasting and measurable influences on QOL in these patients. These issues must be further probed, which also have implications on the increasing use of stereotactic radiotherapy for vertebral metastases.
Despite the prospective randomized nature of this study with a low drop-out rate, there are several limitations, in addition to those presented above such as the small sample size, diversity in primary disease (and degree of control thereof), and lack of formal power calculations owing to the explorative nature. Moreover, because all patients had advanced cancer, 60% of the IMRT patients and 40% of the 3DCRT group were lost to follow-up from progressive disease and/or death. Finally, as described elsewhere (15), it is imperative to mention that no study evaluating QOL or patient-reported outcomes can account for the innumerable factors that influence these variables, including prior therapy, baseline characteristics, social support, comorbidities, experience at the radiation facility, and nature of follow-up. As a result, further data are highly encouraged to validate the conclusion made herein.
Effects on fatigue according to EORTC QLQ-FA 13.
Effects on emotional distress according to the FBK-R10 questionnaire.
Conclusion
This is the first randomized study evaluating QOL between IMRT and 3DCRT to palliate vertebral metastases. IMRT results in reduced physical and emotional fatigue along with emotional distress. Although IMRT should be further studied for these patients given these outcomes, larger randomized trials are necessary to confirm these findings.
Toxicity profile at 6 months after radiotherapy in both groups.
Acknowledgements
The sponsors of the study had no role in study design, data analysis, data interpretation and wording of the report. The corresponding author (HR) had full access to the entire data of the study and had the final responsibility regarding the decision to submit for publication.
Footnotes
Conflicts of Interest
The Authors declare that they have no competing interests.
- Received May 31, 2018.
- Revision received July 5, 2018.
- Accepted July 9, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Independent Validation of a Risk Stratification Model Predicting Survival in Elderly Patients Irradiated for Bone Metastases
- Independent Validation of a Comprehensive Machine Learning Approach Predicting Survival After Radiotherapy for Bone Metastases
- Palliative Radiotherapy as a Treatment for Carcinoma Invasion of the Sacrum: An Observational Case Series Study