


Abstract
Background/Aim: There is no definite consensus regarding management of hepatocellular carcinoma (HCC) with portal vein tumor thrombosis (PVTT). This study aimed to compare clinical outcomes according to initial treatment modality for treatment of naïve HCC combined with subsegmental (Vp1)/ segmental (Vp2) PVTT with liver resection (LR) versus trans-arterial chemoembolization (TACE) followed by radiotherapy (RT). Materials and Methods: From our institutional registry, we enrolled 78 patients diagnosed with HCC combined with Vp1 or Vp2 PVTT and treated with LR or TACE followed by RT (TACE-RT) as a primary treatment. Results: LR was more frequently applied for younger, nodular tumor morphology, or solitary tumor. Overall, LR yielded significantly better progression-free survival (PFS) (p=0.02, 41.9% vs. 15.7% at 2-years), and marginally higher overall survival (OS) (p=0.09, 75.8% vs. 61.5% at 2-years). There was an interaction effect between primary treatment and tumor morphology, and a significantly higher PFS was observed after LR in nodular morphology, in contrast with the lower PFS that was achieved after LR in infiltrative or massive morphology. Conclusion: Although LR yielded higher PFS than TACE-RT in HCC with Vp1 or Vp2 PVTT with similar acute complications, the difference in PFS between the LR and TACE-RT groups was significantly affected by tumor morphology.
As the second most common cause of cancer-related death worldwide (1), hepatocellular carcinoma (HCC) is an important unresolved health problem. A considerable portion of patients are still diagnosed as unresectable and treated palliatively (2-4). Portal vein tumor thrombosis (PVTT) is one of the most important obstacles to successful curative local treatments (5).
There is no definite consensus regarding management of HCC with PVTT, especially in patients with minimal vascular invasion on subsegmental (Vp1) and/or segmental (Vp2) portal vein. Although the Barcelona Clinic for Liver Cancer's (BCLC) staging system recommends sorafenib based on two randomized clinical trials (5), superior outcomes have been reported from local modalities like surgery, trans-arterial chemoembolization (TACE), or a combination of TACE and radiotherapy (RT) (6-9). There is also growing evidence that TACE plus RT (TACE-RT) offers superior outcomes for unresectable HCC compared with TACE alone (10). A large cohort study from Japan found that liver resection (LR) yielded excellent survival outcomes in patients with HCC and PVTT (11). The clinical outcomes of these local modalities are affected by PVTT location and superior outcomes usually occur in patients with Vp1-2 PVTT.
Because PVTT can weaken liver function by prohibiting blood flow and can act as a source of intrahepatic and extrahepatic metastasis, early eradication is important for improving clinical outcomes for HCC combined with PVTT (12). At the same time, however, considering the unfavorable survival outcomes and frequent recurrence of HCC combined with PVTT, unnecessary aggressive management should be avoided.
This retrospective registry study was conducted to compare clinical outcomes from local modalities, LR and TACE-RT, for treatment-naïve HCC patients with Vp1-2 PVTT and investigated which subgroup received the most benefit by LR.
Patients and Methods
The HCC registry of the Samsung Medical Center includes newly diagnosed HCC patients who received primary care at Samsung Medical Center; our institution has been prospectively collecting patient data since January 2005. Detailed information about the registry has been described previously (13).
This study comparing clinical outcomes from LR and TACE-RT in HCC patients with Vp1-2 PVTT was approved and received an exemption from written consent by the Samsung Medical Center Institutional Review Board. Our study subjects were patients who received care between January 2010, after the set-up of the current scheduled TACE-RT protocol, and July 2014 (14).
All liver resections were performed by four highly experienced liver surgeons (J.W.J., C.H.K., G.S.C and J.M.K). Among the HCC patients with combined Vp1-2 PVTT, those with the following characteristics were considered for LR rather than other local modalities: 1) Child-Pugh class A, 2) serum total bilirubin <1.5 mg/dl, 3) indocyanine green retention test at 15 min (ICG-R15) <20%, 4) no ascites, or 5) patent portal flow in expected remaining liver lobe. Other operative procedures practiced by our institution have been previously detailed (15).
Patients who did not indicate a preference for LR or whose physicians did not prefer LR for them underwent TACE followed by RT (TACE-RT) at a two-week interval. The detailed TACE-RT protocol was described in a previous study (14). Other details about RT including target definition, dose determination, and verification using image guidance were described in previous reports (16).
Patients who underwent LR were evaluated postoperatively every 2-3 months, and the patients who received TACE-RT were evaluated 1 month after RT completion and at 2-3-month intervals thereafter. Treatment responses and disease progression were assessed by CT and/or MRI using the modified Response Evaluation Criteria in Solid Tumors (mRECIST) (17). Local recurrence was defined as an increase of 20% in diameter of the viable tumor encompassed by a PTV in the follow-up CT or MRI at least. The other recurrence developed in the liver outside of the PTV was defined as intrahepatic elsewhere recurrence.
To compare the difference between the groups, the chi-square test or Fisher's exact test and the Mann-Whitney U-test were used. Overall survival (OS) and progression-free survival (PFS) were calculated as the duration from the starting date of primary treatment to the date when a new event was first detected or, to the date of the last follow-up visit; survival rates were estimated using the Kaplan–Meier method.
For each prognostic factor, main effects and interaction effects of primary treatment were investigated. AFP was log-transformed due to highly-skewness before the analysis. Cox proportional hazards models were used, and assumption from this model was checked with the Kolmogorov supremum test. Multicollinearity was examined using the variance inflation factor (VIF) and lack of multicollinearity was confirmed when VIF was <4. All statistical analyses were executed using SAS version 9.4 (SAS Institute, Cary, NC, USA) and R 3.3.2 (Vienna, Austria; http://www.R-project.org/). A p<0.05 was considered statistically significant and all statistical tests were evaluated as two-sided.
Results
Patients. During the study period of January 2010 to July 2014, 249 patients were enrolled in the Samsung Medical Center's HCC Registry as having HCC with either Vp1 or Vp2 PVTT. Among the 140 treatment-naïve HCC patients with Vp1 or Vp2 PVTT, 78 who were treated with LR (n=31) or TACE-RT (n=47) as their primary treatment were analyzed. The baseline characteristics of enrolled patients according to primary treatment are displayed in Table I.
Adverse events according to primary treatment. There was no treatment related death within 30 days after treatment in both groups. Assessment of other treatment related toxicities proceeded in terms of toxicity-grade elevation according to the Common Terminology Criteria for Adverse Events version 4.0 (CTCAE V4.0), to evaluate treatment complications as objectively and accurately as possible to reduce bias from the initial differences in characteristics. There was one patient (3.2%) who needed to be readmitted for wound repair because of an operation-site infection. Hematologic toxicities developed more frequently in patients who received TACE-RT (6-30% in LR vs. 30-40% in TACE RT), but other laboratory results were not significantly different according to treatment modalities. Aggravation due to anorexia, nausea, and vomiting developed more frequently after TACE-RT than LR, but these toxicities were generally manageable and resolved by the first post-treatment follow-up.
Patterns of recurrence and salvage treatment. Among the 31 patients who received LR, 20 (64.5%) experienced their first recurrence intrahepatically (15, 48.4%) or extrahepatically (5, 16.1%), and seven patients died (22.6%) from recurrence. TACE was mainly used for palliative treatment either alone (9, 29.0%) or in combination with RT (4, 12.9%) after intrahepatic recurrence. One patient received a combination of TACE and radiofrequency ablation (RFA), and the last one received RT. Among the five patients who experienced extrahepatic recurrence, three were treated with systemic therapy (sorafenib in two patients and cytotoxic chemotherapy in one patient). Of two other patients who were managed with supportive care only, one received RT for bone metastasis.
Among the 47 patients treated with TACE-RT as their primary treatment, 41 (87.2%) experienced either an intrahepatic local recurrence (six patients: isolated in two, combined with intrahepatic elsewhere in three, combined with intrahepatic elsewhere and extrahepatic metastasis in one), an intrahepatic non-local recurrence (19 patients; isolated in 15, combined with extrahepatic metastasis in four), or extrahepatic recurrence (16 patients); 21 patients (22.6%) died after recurrence. Additional local treatments were used in 18 out of 20 patients who had recurrences that were local and/or intrahepatic or elsewhere, including LR in one, RFA in one, RT in two, and TACE in 14. Systemic therapy was used for 12 of 21 patients (sorafenib in 10, cytotoxic chemotherapy in one, and clinical trial in one) who had extrahepatic recurrence with or without intrahepatic/local recurrence; local modalities were attempted first in five of these patients. The remaining six patients received supportive care only.
Baseline characteristics of patients treated with LR or TACE-RT.

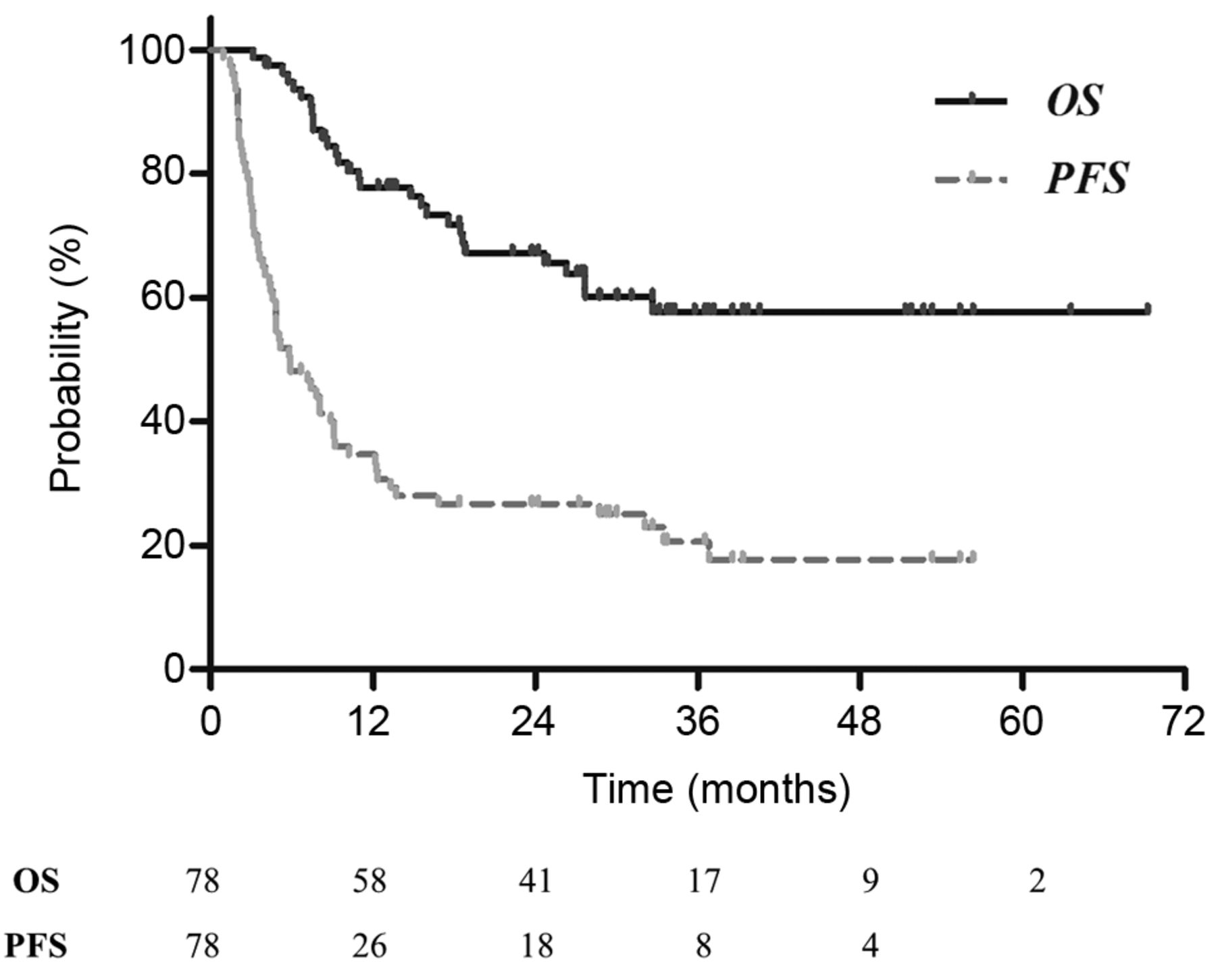
Kaplan–Meier curves for progression-free survival (PFS) and overall survival (OS) for all 78 enrolled patients. The PFS and OS were 26.4% and 67.2% at 2 years, respectively.
Survival outcomes according to primary treatment. Among the 78 patients treated with LR or TACE-RT, 61 experienced disease progression (78.2%) and 28 (35.9%) died during the follow-up period that ranged from 2.5-69.3 months (median, 24.6 months). The PFS and OS for all enrolled patients after 2 years were 26.4% and 67.2%, respectively; the Kaplan–Meier survival curves are as shown in Figure 1. The estimated PFS and OS rates were 41.9% and 75.8% in LR group, and 15.7% and 61.5% in TACE-RT group (Figure 2). Without controlling for differences in characteristics between the two groups, there was a significant difference in PFS (p=0.02, hazard ratio [HR]=0.53, 95% confidence interval [CI]=0.31-0.23), but a non-significant difference in OS (p=0.09, HR=0.44, 95%CI=0.19-1.05).
To determine the optimal primary treatment according to baseline characteristics, we conducted analyses comparing the clinical outcomes from the two groups that considered possible interaction effects among significant prognostic factors for PFS. The results of univariable analyses of probable prognostic factors with consideration of interaction effects of the primary treatment are displayed in Table II.
Tumor size was a significant prognostic factor for PFS after adjusting for primary treatment (p=0.03, HR=1.11, 95%CI=1.01-1.22), while primary treatment was also a significant prognostic factor for PFS after adjusting for tumor morphology (p=0.02, HR=0.45, 95%CI=0.23-0.88). There were also interaction effects between primary treatment and tumor morphology (p=0.002, HR=7.46, 95%CI=2.07-26.88). The significantly higher PFS was observed after LR in the subgroup with nodular morphology (p=0.03, 41.9% in LR vs. 15.7% in TACE-RT at 2-years). In contrast, lower PFS occurred after LR in the subgroup with diffuse or infiltrative morphology (p=0.02, not reached in LR vs. 15.3% in TACE-RT at 2-years). The Kaplan–Meier curves for PFS according to primary treatment and tumor morphology is provided in Figure 3.
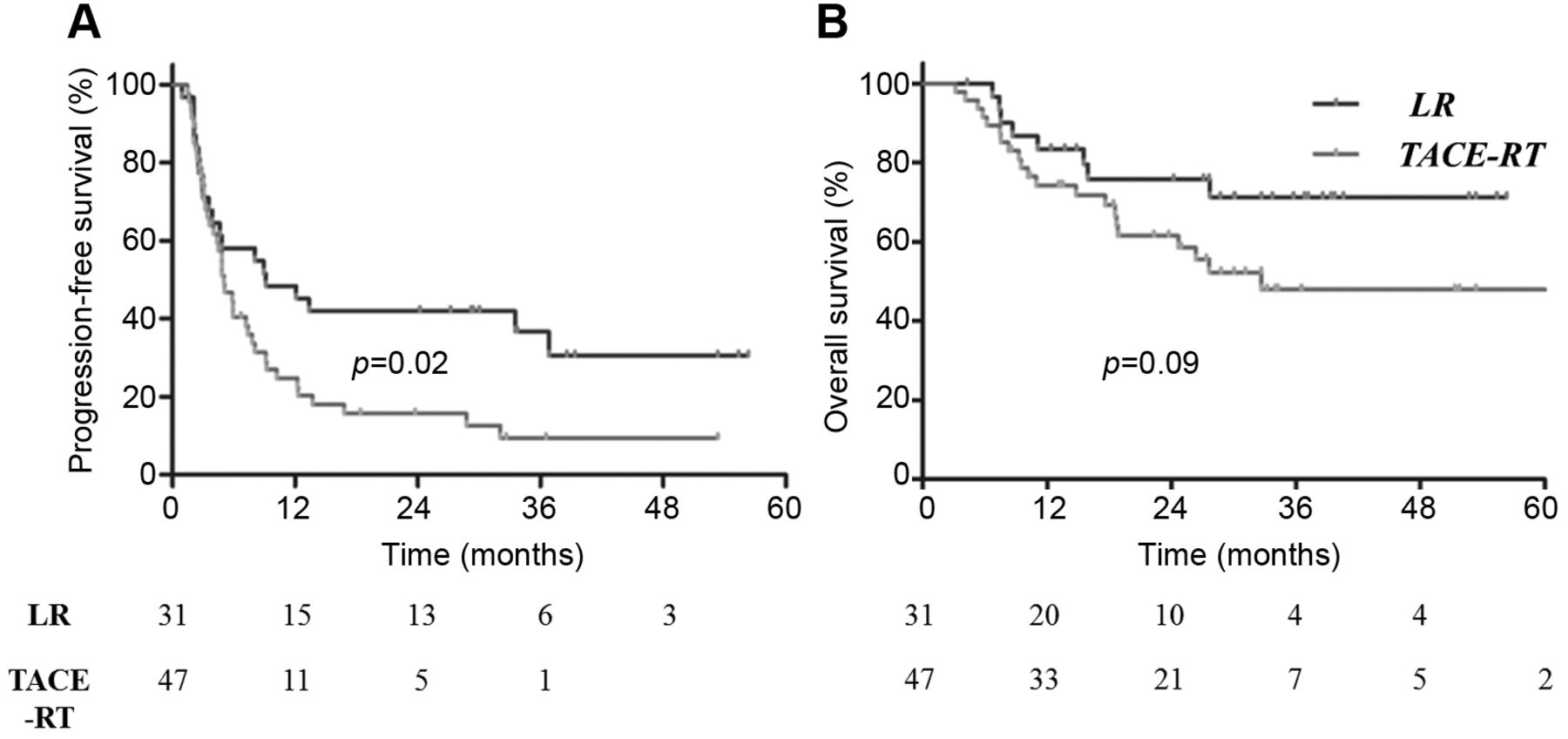
Kaplan–Meier curves for PFS and OS according to primary treatment. The PFS (A) was significantly better and OS (B) was marginally superior in the group treated with LR as a primary treatment when differences in characteristics between the two groups were not taken into consideration.
Univariable analysis for PFS and OS with interaction effects with primary treatment.
On the contrary, OS outcomes according to the primary treatment were not significantly affected by other baseline characteristics that were significant prognostic factors of OS without consideration of interaction effects, and there was no significant prognostic factor according to our analyses that included interaction effects.

Kaplan–Meier curves for PFS according to primary treatment and tumor morphology. A significantly higher PFS was noticed after LR in the subgroup with nodular morphology (A), in contrast to lower PFS that was observed after LR in the subgroup with diffuse or infiltrative morphology (B).
Discussion
In this study, we compared clinical outcomes according to local initial treatment modalities, LR and TACE-RT, in treatment-naïve HCC patients with Vp1-2 PVTT, the clinical outcomes from LR were superior to those from TACE-RT, and the OS of LR was marginally superior to that of TACE-RT. PFS, AFP level, tumor size, morphology, and multiplicity were all significant prognostic factors. Interestingly, the difference in PFS between the LR and TACE-RT groups was significantly affected by tumor morphology.
PVTT is one of the most reliable prognostic factors for HCC patients (18, 19). It causes liver function deterioration, portal pressure increment, interference of successful TACE, intrahepatic metastasis, and extrahepatic metastasis (20-23). Though sorafenib is the only recommended treatment by the BCLC guidelines (5), for patients with minor tumor thrombosis on Vp1 and/or Vp2, the usefulness of LR was consistently reported, mainly in Japan (24, 25). A recent survey study of the Liver Cancer Study Group of Japan reported cumulative survival rates of 48.2% in Vp1 and 29.2% in Vp2 after LR (25).
Based on its proven survival efficacy for unresectable HCC, TACE is one of the most widely used local modalities for HCC cases (26). However, the reported clinical outcomes from treatment with TACE alone were generally inferior to LR in HCC patients with PVTT (7).
With the rapid developments in technology and radiobiology, RT has recently become a frequently administered treatment for HCC (27-30). Because RT is less invasive than LR as a local modality, RT is often performed for cases of locally advanced HCC without distant metastasis, such as cases with combined PVTT. TACE is frequently combined with other treatments, mostly prior to RT, in order to maximize local control and obtain additional information for targeting the tumor using image guidance. According to a recent meta-analysis, adding RT to TACE yielded significantly better complete responses (odds ratio [OR]=1.57, 95%CI=1.26-1.96) and one-year OS rates (OR=1.38, 95%CI=1.16-1.65) (11).
There are no published randomized controlled trials that directly compared LR and TACE-RT in HCC patients with PVTT. Thus, the preference for localized treatment in these patients remains controversial because of reported conflicting results. Tang et al. reported significantly better cumulative survival outcomes from TACE-RT than LR in HCC patients with PVTT (18). Many other studies, including large cohort studies, however, reported outcomes that show that LR outperforms other treatment modalities, including TACE-RT, even after propensity score matching analysis (7, 19, 24, 25). These results, however, should be carefully interpreted because of selection biases that are an inevitable limitation of retrospective studies.
In this study, there was a significant PFS difference between LR and TACE-RT. As reported in other cohort studies, we reaffirmed that LR could provide the most promising oncologic outcome in selected HCC patients with Vp1 orVp2. The difference in PFS, however, is mostly recognized after six months of follow-up. The early progression within 6 months could represent aggressive biological characteristics of disease that are not different between the two groups, as shown in Figure 3A. It might be more appropriate to identify the patients with aggressive disease or an inferior outcome and apply TACE-RT to avoid a more invasive modality.
PFS was paradoxically affected by LR or TACE-RT according to tumor morphology. PFS was significantly worse in patients treated with LR, particularly if they had infiltrative or massive-type HCC combined with Vp1 or Vp2 PVTT. In contrast, significantly better survival outcomes were obtained by LR in patients with nodular-type HCC. LR should be preferentially considered in these patients.
This study has several limitations. First, a small number of cases was analyzed, which presented a serious obstacle to generalizing our findings before being validated by large-scale prospective studies. Second, the study is an inevitable selection bias between the two groups because the primary treatment of LR or TACE-RT was determined according to very strict selection criteria and it is a retrospective, single institution study. The difference in survival outcomes could be largely affected by these differences in characteristics.
Despite the above-mentioned major limitations, this study offers important and valuable findings. As far as we know, this is the only study to compare clinical outcomes between LR and TACE-RT as a primary treatment in treatment-naïve HCC with Vp1/2 PVTT. Our findings highlight important prognostic factors for PFS in treatment-naïve HCC with Vp1/2 PVTT, which include tumor multiplicity, AFP level, and tumor size. Additionally, PFS was significantly affected by choice of primary local modality, LR or TACE-RT. This study provides crucial decision-making information regarding the optimal primary treatment modality in these patients.
In treatment-naïve HCC with Vp1/2 PVTT, LR yielded significantly better PFS and marginally superior OS than TACE-RT. The superiority of LR for PFS, however, was inverted in the subgroup that had diffuse or infiltrative tumor morphology. Tumor morphology could be a valuable criterium for choosing a primary treatment in patients. Further large-scale studies on this topic are required.
Acknowledgements
This research was supported by a Basic Science Research Program through the National Research Foundation of Korea (NRF), which was funded by the Ministry of Education (NRF-2017R1D1A1B03031275), and a grant from the Marine Biotechnology Program (20150220), which was funded by the Ministry of Oceans and Fisheries, Korea.
Footnotes
↵* These Authors contributed equally to this study.
Conflicts of Interest
The Authors declare that they have no conflicts of interest to this work.
- Received May 23, 2018.
- Revision received June 14, 2018.
- Accepted June 15, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}