


Abstract
Background/Aim: In chronic lymphocytic leukemia (CLL) the absolute neutrophil count (ANC) has generally been reported to be within normal limits and leukocytosis is due to absolute lymphocytosis. However, other cell types such as neutrophils and monocytes may also exceed the normal range in this disorder. The aim of this retrospective study was to evaluate the frequency and prognostic value of neutrophilia defined as an ANC>7×109/l and monocytosis- an absolute monocyte count (AMC)>1×109/l in 113 patients with chronic lymphocytic leukemia (CLL). Materials and Methods: We analyzed clinical and laboratory data from the records of patients with CLL followed in the Hematology unit of a tertiary hospital in Israel. Patients were categorized according to their ANC and AMC before treatment and their data compared. Results: In 24 (21%) patients, neutrophilia was present at diagnosis while 40 (35%) had monocytosis. We identified that 9% of cases had neutrophilia with normal AMC. This subgroup of patients had a better prognosis with lower mortality rate, longer time-to-treatment interval and a higher rate of complete or partial response to treatment compared to patients without neutrophilia or monocytosis. Conclusion: The presence of neutrophilia without monocytosis before treatment appears to be associated with a more favorable prognosis in CLL. These observations still need to be confirmed and validated in a larger cohort of patients.
Chronic lymphocytic leukemia (CLL) is the most frequent leukemia in the western world. The diagnosis is established when at least 5×109/L clonal B–lymphocytes bearing the CD5 antigen and other characteristic B cell markers are present in the peripheral blood for a period of at least three months (1, 2). In recent years major advances have been made in the identification of prognostic factors to stratify patients based on molecular and genetic parameters (3, 4).
In general, neutrophil counts in CLL patients have been reported to be normal or slightly reduced (5-8), while an elevated absolute monocyte count (AMC) >1×109/L, seems to be more frequently encountered (9) and associated with negative prognosis (10). In this respect most reported studies relate to neutrophil and monocyte dysfunction in CLL and not their absolute number.
In CLL, the neutrophil dysfunction described include enzyme deficiencies of lysozyme, myeloperoxidase, or β-glucuronidase, which can resolve when complete response (CR) is achieved (5, 6, 9, 11). Monocyte dysfunction also occurs and includes low cytokine production, endotoxin tolerance and impaired inflammatory response to pathogens (8), but this does not impair differentiation to macrophages (5). Some controversial data on the role of neutrophils has been reported on the pathogenesis of CLL (8, 12, 13), however neutropenia has mostly been considered as an expression of more advanced disease related either to the extent of bone marrow infiltration by CLL, or to myelosuppressive therapy administered (8, 13).
In this respect, it should be noted that neither the frequency of neutrophilia nor its prognostic significance have been dealt with in any detail until now. Because of this, the data were examined to determine the frequency and prognostic implications of elevated neutrophil and monocyte counts in our patients with CLL.
Materials and Methods
This retrospective study included all patients diagnosed with CLL/SLL followed at the Hematology unit of Bnai-Zion Medical Center, a tertiary hospital in Haifa, Israel.
The following epidemiological and clinical data were extracted from the patients' charts: gender, ethnicity, age at diagnosis, date of diagnosis, first treatment and last follow-up, as well as details of different treatment regimens given and date of death, when relevant. Laboratory data included: complete blood count with an obligatory report of the peripheral smear performed by an expert technician using a manual count of the different white blood cells sub-populations; serum biochemistry and β2-microglobulin levels before initiation of treatment. Patients were grouped according to their absolute neutrophil count (ANC) and AMC before treatment. Neutrophilia was defined as ANC>7×109/l, relevant neutropenia as ANC<1×109/l and monocytosis as AMC>1×109/l (13).
All the above data were included in an excel table and statistical analysis was performed with SPSS software (version 21). The results were recorded as mean with standard deviation for continuous data, and as frequency and percentage for categorical data. The Pearson χ2 test and Fisher exact test were used to detect differences in the prevalence of categorical variables, while a t-test was conducted to determine if there were any differences in the continuous variables between the two groups. Survival analysis was performed using a Kaplan Meier survival analysis: Cox proportional hazards regression model was used to calculate hazard ratio (HR) with a log-rank test. The level of significance was reported at p<0.05.
Results
A total of 135 patients with CLL/SLL were followed at the Bnai Zion Medical Center in Haifa during 1992-2018. Of these, 113 (84%) had a complete blood count with manual differential count before treatment. Median follow-up for the entire cohort was 92 months (range=1-315 months).
In this cohort, absolute lymphocyte counts (ALC) ranged from 0.84-359×109/l; ANC varied from 0.31-18×109/l, including 24 (21%) patients with neutrophilia, 82 (73%) with normal neutrophil counts and 7 (6%) with neutropenia; AMC ranged from 0-7.7-×109/l, including 40 (35%) with monocytosis.
We analyzed overall survival (OS) based on ANC at diagnosis, dividing patients into 3 groups: ANC<1×109/l, 1-7×109/l and above 7×109/l. Indeed, patients who presented with neutropenia (ANC<1×109/l) had median OS of only 60 months, while those who presented with ANC=1-7×109/l and >7×109/l had median OS of 88 and 101 months respectively. These differences were statistically significant with p=0.031 (Figure 1A).
We also performed survival analysis based on AMC at diagnosis; and observed a trend for worse prognosis for patients diagnosed with AMC>1×109/l. Because of this finding, the analysis was repeated only on the 73 patients without monocytosis and the data from patients with different neutrophil counts were compared, but only in this subgroup. Of these, 10 had neutrophilia and 63 had normal or low neutrophil counts. When comparing all patients' characteristics with or without neutrophilia (Table I), no differences were found in gender, ethnicity or age at diagnosis. Serum β2-microglobulin levels and AMC were also similar in these two groups, however ALC was significantly higher among patients with neutrophilia. Furthermore, the mortality rate was lower in patients with neutrophilia (Figure 1B). In relation to therapy, the same average number of treatment courses were used in both groups but the time to first treatment was longer for patients with neutrophilia who needed treatment, than for those without neutrophilia; no differences were found for untreated patients (Table I). Finally, a higher rate of complete or partial response (CR/PR) was found in the group of treated patients who had neutrophilia without monocytosis, compared to treated patients without neutrophilia or monocytosis (Table I). In terms of median OS, when examining patients without monocytosis who had ANC<1×109/l, 1-7×109/l and >7×109/l we were again able to divide our cohort into 3 groups with different median OS of 60, 107 and 133 months (Figure 1B) with statistical significance (p=0.003).
Discussion
In this retrospective study, neutrophilia was evident in 21% of patients with CLL before treatment and is a positive prognostic factor in cases without associated monocytosis. This CLL subgroup had a lower mortality rate, longer time to first treatment after diagnosis and a higher rate of CR/PR after treatment.
While the ALC in itself does not seem to be of prognostic value in CLL (14), different and sometimes conflicting data have been reported regarding the role of neutrophils in this disease. On the one hand, neutrophils have been shown to favor leukemic B cell proliferation via the release of extracellular traps (NETs), which may delay spontaneous apoptosis and increase the expression of B-CLL cell activation markers (12); or alternatively via production of reactive oxygen species (ROS) or various cytokines that may induce “tolerance” (8). On the other hand, the presence of more neutrophils has been linked more frequently with inactive (vs. active) and untreated (vs. treated) disease as well as with IgHV mutated (vs. unmutated) status (8). All this provides indirect support for our findings, which show that an increasing neutrophil count may be associated with a better prognosis in CLL.
Other possible explanations for the above findings include the presence of a more inflammatory microenvironment generated by neutrophils (7), which appears to improve innate immunity in patients with CLL. This hypothesis was not checked in preceding studies but does sounds sensible, particularly since CLL-associated mortality has clearly been associated with infections due to accompanying immunodeficiency, resulting from both hypogammaglo-bulinemia and neutropenia - mostly present in advanced disease (5-7). In this respect, neutrophilia may perhaps represent a positive reflection of a functional “reactive” bone marrow even in the presence of extensive CLL infiltration, providing better defenses against infection. This may partially explain why patients with CLL and neutrophilia (but without the adverse influence of monocytosis) (9, 10) may require treatment less frequently and have the lowest mortality rates.
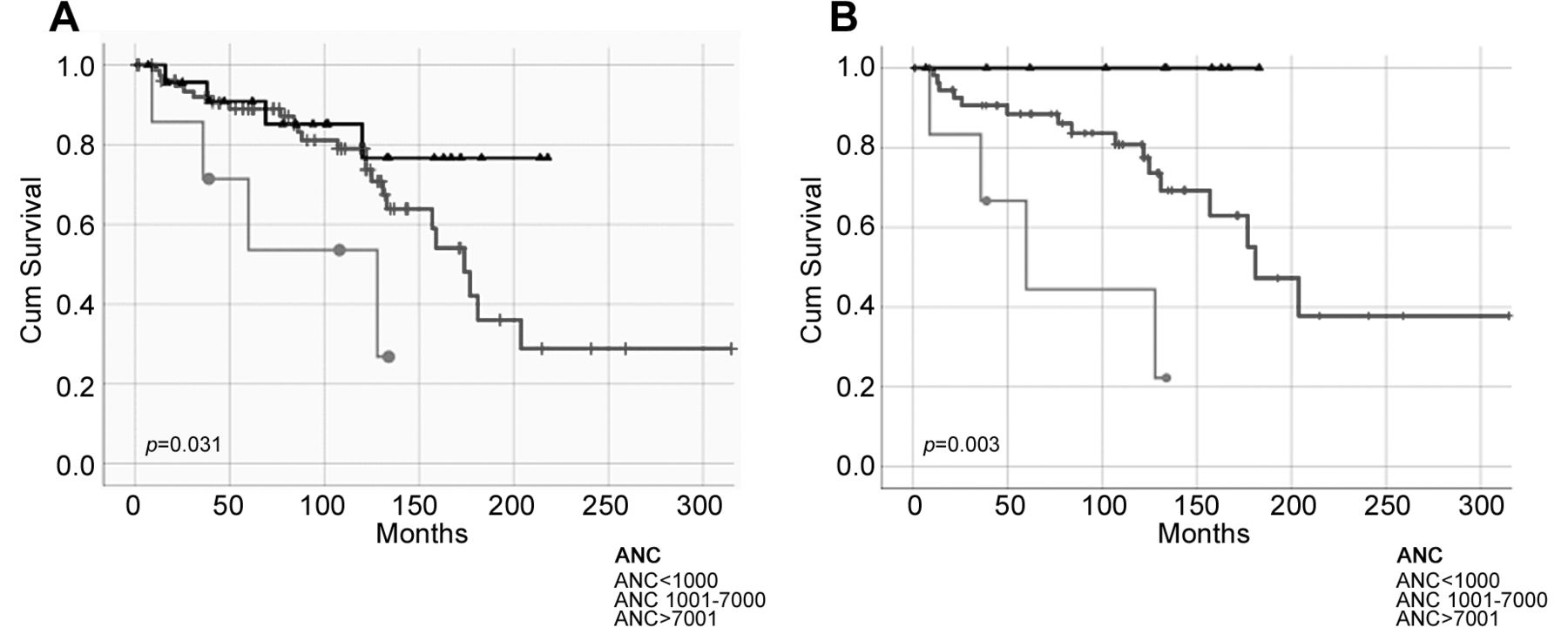
Kaplan–Meier survival analysis of the whole cohort based on absolute neutrophil count (ANC) (A) and of patients based on ANC after exclusion of cases with monocytosis (B).
Characteristics of CLL patients with/without neutrophilia and without monocytosis.
Finally, another factor could also relate to observations of recent studies showing that neutrophils also have an anti-CLL role in the mediation of trogocytosis of anti-CD20 opsonized B cells, after the therapeutic use of the monoclonal antibodies rituximab or obinutuzumab (13). This may also help to explain the higher rates of CR/PR seen in our CLL cohort following treatment in patients with neutrophilia.
Further research investigations clearly still need to be performed in order to determine the basis for the observations reported in this study. Larger prospective clinical trials are required to confirm and validate our findings or exclude any unexpected association with other recognized clinical, laboratory and genetic prognostic factors. This could indeed establish whether high ANC with normal AMC is in fact a useful positive prognostic factor in clinical practice.
Footnotes
Conflicts of Interest
The Authors have no conflicts of interest to declare.
- Received May 19, 2018.
- Revision received June 10, 2018.
- Accepted June 11, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.