


Abstract
Background: Static magnetic fields (SMF) exhibit antitumoral activity and enhance the efficacy of chemotherapy by opening the tumor–blood barrier. This study aimed to analyze different SMF-exposure protocols on epidermal growth factor receptor (EGFR)-overexpressing tumors, as well as their combination with cetuximab. Materials and Methods: Experiments were performed in skinfold chamber preparations of C57Bl/6-and CD-1nu/nu mice bearing LLC-1 tumors. Animals were exposed to 587 mT magnetic field following different exposure protocols. A subgroup received additional cetuximab injections. Using in vivo-fluorescence microscopy and planimetry, tumor angiogenesis, growth and microcirculation were repeatedly analyzed for 13 days. Results: In contrast to daily short SMF exposure, three-fold SMF exposure for 2 h led to a significant 46% reduction of tumor growth. Adding cetuximab to SMF exposure did not yield any benefit, although cetuximab monotherapy was highly effective (53% reduction of tumor growth), indicating a potential interference of SMF and EGFR signaling. No effects on microcirculation, angiogenesis or leukocyte–endothelium interactions were documented. Conclusion: The use of SMF is promising in the treatment of solid tumors; however, it appears to interfere with EGFR-targeted therapy.
In the past two decades, research on magnetic fields and their effects on tumors has gained growing interest. Various studies confirmed that static magnetic fields (SMF) affect tumor cell biology in vitro (1) as well as in vivo (2, 3). However, the influence of various SMF exposure durations has not yet been studied in detail. Furthermore, there is little evidence of the effect of SMF on squamous cell carcinoma growth in vivo. Especially in recurrent squamous cell carcinoma of the head and neck (HNSCC), new treatment strategies are needed, when all curative treatment options – surgery and radio(chemo)therapy – might have failed (4). The clinical application of magnetic fields to the head and neck region appears feasible by using specially designed head coils which have been in use for MRI diagnostics since the early 1980s (5).
Recent studies highlight the epidermal growth factor receptor (EGFR) as a potential primary target of magnetic fields (6-8). EGFR is overexpressed in over 90% of HNSCC cells (9), which is associated with an extraordinary aggressive behavior (10) and a worse prognosis and reduced survival (11, 12). Furthermore, enhanced resistance to chemotherapy and radiation therapy has been shown in patients with EGFR-overexpressing tumors (13, 14). Therefore, antibody-mediated blockage of EGFR signals has become proof-of-principle in favor of novel targeted therapy regimen's in HNSCC. Added to conventional chemotherapy, the first clinically-approved EGFR inhibitor, cetuximab, was found to significantly prolong the overall survival in patients with therapy-refractory HNSCCs (15).
For ligand-induced activation of the intracellular signal cascade, the dimerization of EGFR is crucial (16). However, SMFs induce clustering of EGFR in vitro (6, 7). Consequently, SMF exposure might interact with anti-EGFR therapy in vivo.
The combination of SMF exposure with conventional chemotherapy was shown to be synergistic in vitro (17) as well as in vivo (18, 19). However, combination therapy using SMF exposure and targeted therapy, e.g. cetuximab, to our knowledge has not been addressed experimentally. Therefore, the present study aimed to analyze the effects of different SMF-exposure protocols in combination with EGFR-targeted therapy on HNSCC growth.
Study treatment groups: The different study groups including their respective treatment schedules and controls are displayed.
Materials and Methods
Animals. All animal experiments were in accordance with German legislation for the protection of animals and approved by the local government (Regierung von Oberbayern, Munich, Germany, Reference number 55.2-1-54-2531-97-10).
Experiments were carried out using male C57Bl/6 mice and male CD-1nu/nu nude mice (11-13 weeks old, 27±2 g body weight; Charles River, Sulzbach, Germany). The treatment study comprised six groups of C57Bl/6-mice (n=6 each) and two groups of nude mice (n=6 each). The animals were housed in single cages and had free access to tap water and standard laboratory food (ssniff; Spezialdiaeten GmbH, Soest, Germany).
Dorsal skinfold chamber preparation and tumor cell implantation. For quantitative fluorescence analysis of tumor microcirculation in vivo, a dorsal skinfold chamber consisting of two symmetrical titanium frames was surgically implanted into the dorsal skin of all mice as described in detail elsewhere (20, 21). The surgical procedure was carried under intraperitoneal anesthesia with ketamine (100 mg/kg b.w., Ketavet; Parke-Davis, Berlin, Germany) and xylazine (10 mg/kg b.w., Rompun; Bayer, Leverkusen, Germany). The mice were allowed to recover from anesthesia and microsurgery for a period of 48 h. The chambers were well tolerated and the animals did not show any signs of discomfort. Chamber preparations fulfilling the criteria of an intact microcirculation and lacking sings of inflammation were inoculated with 1 μl of dense tumor cell suspension (~1×105 cells) of syngeneic Lewis lung cancer cells (LLC-1; maintained in house) onto the striated skin muscle layer. High EGFR expression in Lewis lung cancer cells was proven by immunohistochemistry (22), and confirmed by fluorescence-activated cell scanning analysis.
Static magnetic field. SMFs were generated by a cylindrical permanent magnet providing a magnetic flux density of 587 mT, as described elsewhere (23). In order to avoid direct contact between the magnet and the chamber, a minimal distance between the two was always kept.
Experimental protocol. Trans-and epi-illuminated images of the whole tumor–hosting chamber preparations were taken by a digital camera to evaluate tumor growth by planimetry on days 3, 6, 9 and 13 after tumor cell implantation. On days 7 and 13, when tumor microcirculation was well established, in vivo fluorescence microscopy was performed. The acquisition as well as the analysis of all data was performed blindly by an investigator (U.S.).
In sum, three series of experiments were performed with two or three groups of six animals each. Table I summarizes the different treatment groups.
In a first set of experiments, two different SMF exposure protocols were evaluated. Therefore, the C57Bl/6 mice were randomly assigned to three groups (n=6 each) 3 days after tumor inoculation on days 3, 6 and 9 after tumor cell implantation, one group of animals was exposed to 587 mT for 120 min (group A). Another group of animals was exposed to 587 mT for 35 min daily on days 3 to 11 (group B). As a control group, six mice were sham-exposed outside the SMF (control). In all three groups, 0.2 ml of 0.9% NaCl was injected intraperitoneally prior to a SMF exposure or sham exposure on days 3, 6 and 9. In a second set of experiments, the combination of SMF exposure with cetuximab treatment was evaluated. Therefore, C57/Bl6 mice were randomly assigned to three additional groups (n=6, each). The animals were treated with 1 mg cetuximab (0.2 ml; Merck KGaA; Darmstadt, Germany) injected intraperitoneally prior to exposure to 587 mT for 120 min (group A+Cet). Another six animals received the same cetuximab treatment, but were exposed to 587 mT for 35 min daily on days 3 to 11 (group B+Cet). Finally, six animals were treated with cetuximab and sham-exposed to SMF (Cet control group). Figure 1 shows the protocol of the two first series of experiments.
A separate series of experiments was performed to detect relevant immunological effects, as cetuximab is a chimeric (human-murine) antibody applied to immunocompetent mice. One group of six nude mice was treated with cetuximab alone as described for the immunocompetent C57Bl/6 mice. As a control group, a second group of six immunodeficient animals was immobilized for 120 min outside the magnetic field after having received 0.2 ml of 0.9% NaCl intraperitoneally.
In vivo fluorescence microscopy. For intravital microscopy, the awake animals were immobilized in a Perspex tube on a custom-designed stage (Effenberger, Munich, Germany) under a modified Zeiss microscope (Axiotech vario; Zeiss, Oberkochen, Germany). To visualize tumor microcirculation, fluorescein isothiocyanate-labeled dextran (MW 500,000; 0.05-0.1 ml of a 5% solution in 0.9% NaCl; Sigma, Deisenhofen, Germany) was injected intravenously into the lateral tail vein as a plasma marker. Rhodamine 6G (Sigma; 0.04 ml of a 0.05% solution in 0.9% NaCl) was injected intravenously for visualization of leukocyte–endothelial cell interactions. Selective observation of both fluorescent markers was achieved by means of epi-illumination with a 100 W mercury vapor lamp (FluoArc; Zeiss) and the use of different specific fluorescence filter sets (Set 10 and 14, Zeiss).

Experimental protocol for C57BL/6 mice: On day 3 after tumor inoculation (d3), animals were randomly assigned to six different treatment groups differing in static magnetic field (SMF) exposure and injected medication. The treatment options are symbolized by black arrows, whereas grey arrows indicate measured parameters. Cet: Cetuximab.
For each implanted tumor, six regions of interest (ROI) with a standardized size of 0.458 mm2 were randomly selected. The images were acquired by a CCD-camera (Sony XC-77CE; Sony; Cologne, Germany) and recorded on digital video tape (Sony DVCAM DSV 45P; Sony) for subsequent offline analysis (Cap Image; Zeintl, Heidelberg, Germany). The offline image analysis was described in detail by Zeintl et al. (24) and Klyscz et al. (25). The following parameters were determined in each of the six ROIs investigated per animal: Capillary red blood cell velocity (vRBC given in mm/s), capillary diameter (D given in μm) and functional vessel density (FVD given in mm/mm2). To improve the reliability, vessel diameters and red blood cell velocity were measured in three vessels per ROI.
Leukocyte–endothelial cell interactions were characterized as numbers of flowing leukocytes and rolling cells (at <50% of vRBC) crossing a given line in 30 s and firmly adherent cells (for >30 s) at the vessel wall.
Statistical analysis. All results are presented as the mean±standard deviation. Statistical evaluation was performed using SigmaStat software (SigmaStat for Windows, Jandel Scientific, Erkrath, Germany). ANOVA on ranks test followed by the Dunnett test was used for the estimation of stochastic probability in intergroup comparisons. For intragroup comparisons, the Wilcoxon test was used. A p-value of less than 0.05 was considered significant.
Results
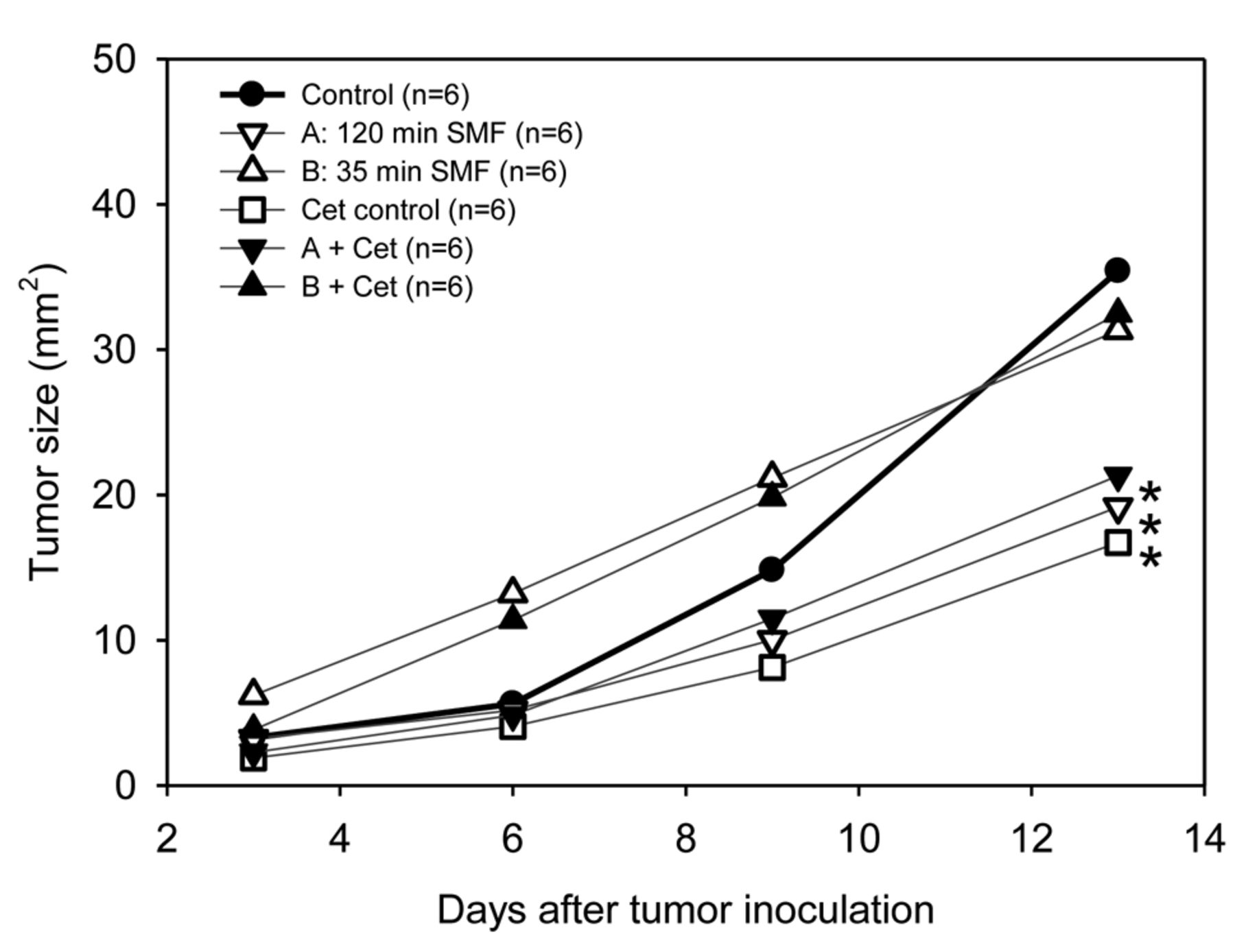
SMF exposure modulation. It was the aim of the first subset of experiments to clarify whether fractionation of SMF exposure affects antitumoral efficacy. Representative images of the growing tumors are presented in Figure 2. Figure 3 demonstrates that the tumor sizes of all groups were comparable in the beginning of the study (on average: 3.1±1.5 mm2). However, at the end of the observation period, tumors exposed to SMF for 120 min on 3 days were significantly smaller (19.2±4.8 mm2) than controls (35.4±12.4 mm2), yielding a relative reduction of tumor growth by 46% compared to control tumors. On the other hand, daily short SMF exposure did not result in significant inhibition of tumor growth (31.3±7.9 mm2), although the total magnetic flux density was almost equal. Therefore, the total exposure time and the total magnetic flux density applied appeared not to be relevant for treatment effects in contrast to exposure duration and frequency.
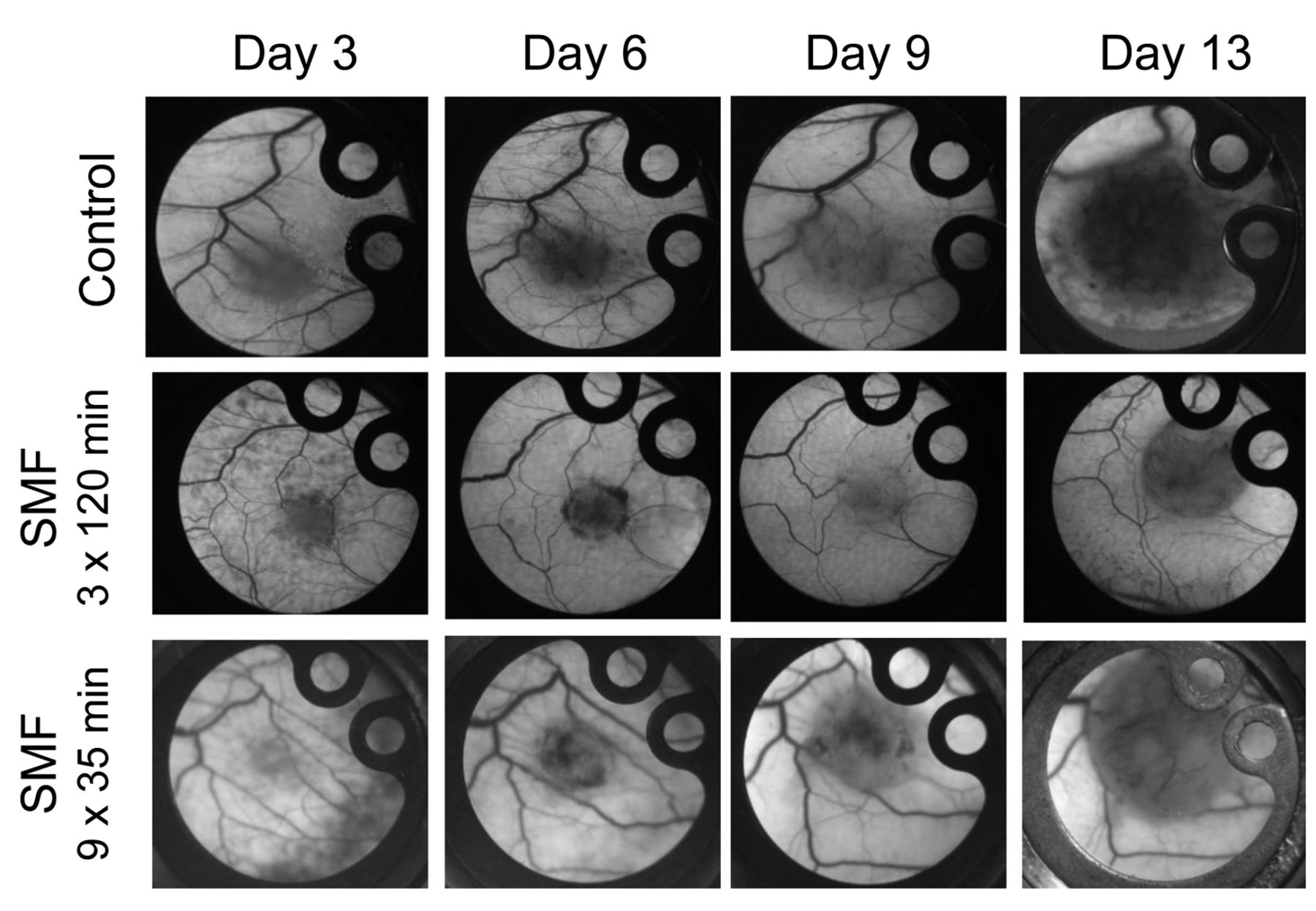
Tumor growth in the dorsal skinfold chamber. Time-lapse sequences clearly show a delay in tumor growth only after three-fold static magnetic field (SMF) exposure for 120 min. Animals exposed daily to SMF for 35 min showed similar tumor growth to that of control animals.
SMF and targeted therapy. SMF exposure was combined with cetuximab treatment. The combination of SMF and cetuximab did not act in an additive manner. Instead, the extent of tumor growth inhibition by different SMF exposure intervals was unaffected by the additional application of cetuximab (Day 13: A vs. A+Cet: 19.2±4.8 mm2 vs. 21.3±5.0 mm2; B vs. B+Cet: 31.3±7.9 mm2 vs. 32.5±7.1 mm2) (Figure 3). However, cetuximab as monotherapy yielded a strong inhibition of tumor growth (16.7±4.6 mm2), reflecting a relative reduction of tumor growth by 53% compared to controls. Hence, SMF appeared to interfere with the effects of cetuximab.
SMF and tumor microcirculation. In order to study the effect of SMF exposure in addition to cetuximab treatment on functional tumor microcirculation, several microcirculatory parameters were measured using in vivo fluorescence microscopy (Table II). On day 7 after tumor cell implantation, all tumors exhibited a chaotic microvascular architecture formed by young microvessels with various diameters and loop formation characteristic of tumor microcirculation. Except for the animals treated with repeated SMF exposure of 120 min, all groups showed a relative increase in functional vessel density from day 7 to day 13 (A: −5%, control +17%, B: +28%, Cet control: +5%, A+Cet: +20%, B+Cet: +14%). Quantitative analysis revealed no significant differences.
Intratumoral leukocyte–endothelial cell interactions. The analysis of leukocyte–endothelial cell interactions revealed no significant differences between the different groups or between different time points for the same group. Even in animals treated with the chimeric antibody cetuximab, there was no increase in leukocyte–endothelial cell interactions.
Immunological effects. To analyze xenogeneic treatment effects of the chimeric antibody cetuximab, experiments in immunodeficient mice were added. In immunodeficient mice, tumor sizes were initially comparable to those in immunocompetent mice. However, tumors grew faster in all immunodeficient mice, independently of the kind of treatment. In immunocompromised mice, the antitumoral activity of cetuximab was less effective, yielding an 18% reduction of tumor growth compared to 53% in immunocompetent mice. Again, cetuximab treatment did not provoke relevant changes in leukocyte–endothelial cell interactions in immunodeficient animals compared with immunocompetent animals.
Microcirculatory parameters of the different treatment groups: No statistically significant differences were found after intergroup or intragroup testing. Values are given as the mean±SD. Study groups are fully defined in Table I.
Discussion
The antitumor, activity of exposure to SMF has already been shown for several cancer entities in vitro (1) as well as in vivo (3, 26). However, to our knowledge, there are no data on this subject concerning HNSCC currently treated with targeted therapy (4). The present study demonstrated that SMF exposure reduces tumor growth of squamous cell carcinoma in vivo by up to 46% compared to sham-exposed tumors. However, this treatment effect was registered after repetitive exposure of 120 min whereas a shorter more frequent exposure affected tumor growth less. As both fractionation protocols yielded different antitumoral effects despite a comparable net magnetic flux density, the modulation of SMF exposure by frequency and duration appears to be a relevant factor for antitumoral treatment efficacy of SMF.
The underlying mechanism of SMF-induced impairment of tumor cell biology is far from being understood in detail. With regard to the molecular pathways, many potential targets of SMF in tumors have been identified: influence on calcium signaling (27, 28), deterioration of antioxidative responses (29, 30) and inhibition of angiogenesis (3, 31) are well known effects of SMF on tumor biology. In contrast to earlier findings in a different tumor model showing reduced tumor vessel density under SMF exposure, microcirculatory parameters were not significantly affected in our study. At least regarding cell proliferation under SMF exposure, it was recently reported that not only different cell lines, but even different cell densities contribute to the extent of biological effects of SMF (32). Furthermore, tumor angiogenesis is a very complex process and varies not only among different tumor types, but also temporally and spatially within a single tumor (33). In addition, as reported for other anti-vascular therapies, net microvascular density may increase or decrease – sometimes depending on the tumor model. Whereas the first concept of anti-angiogenic drug therapy aimed to destroy the tumor vasculature, it was recently shown that anti-angiogenic therapy in fact often leads to normalization of tumor vasculature (34). Instead of inducing regression of tumors by starvation, normalization of the tumor vasculature towards a mature phenotype has recently become a major goal of antiangiogenic therapy in order to alleviate tumor hypoxia and slow tumor progression (33, 35). This might also explain why FVD was not reduced in tumors treated with cetuximab in our study, although cetuximab is known to have anti-angiogenic activity (36, 37).
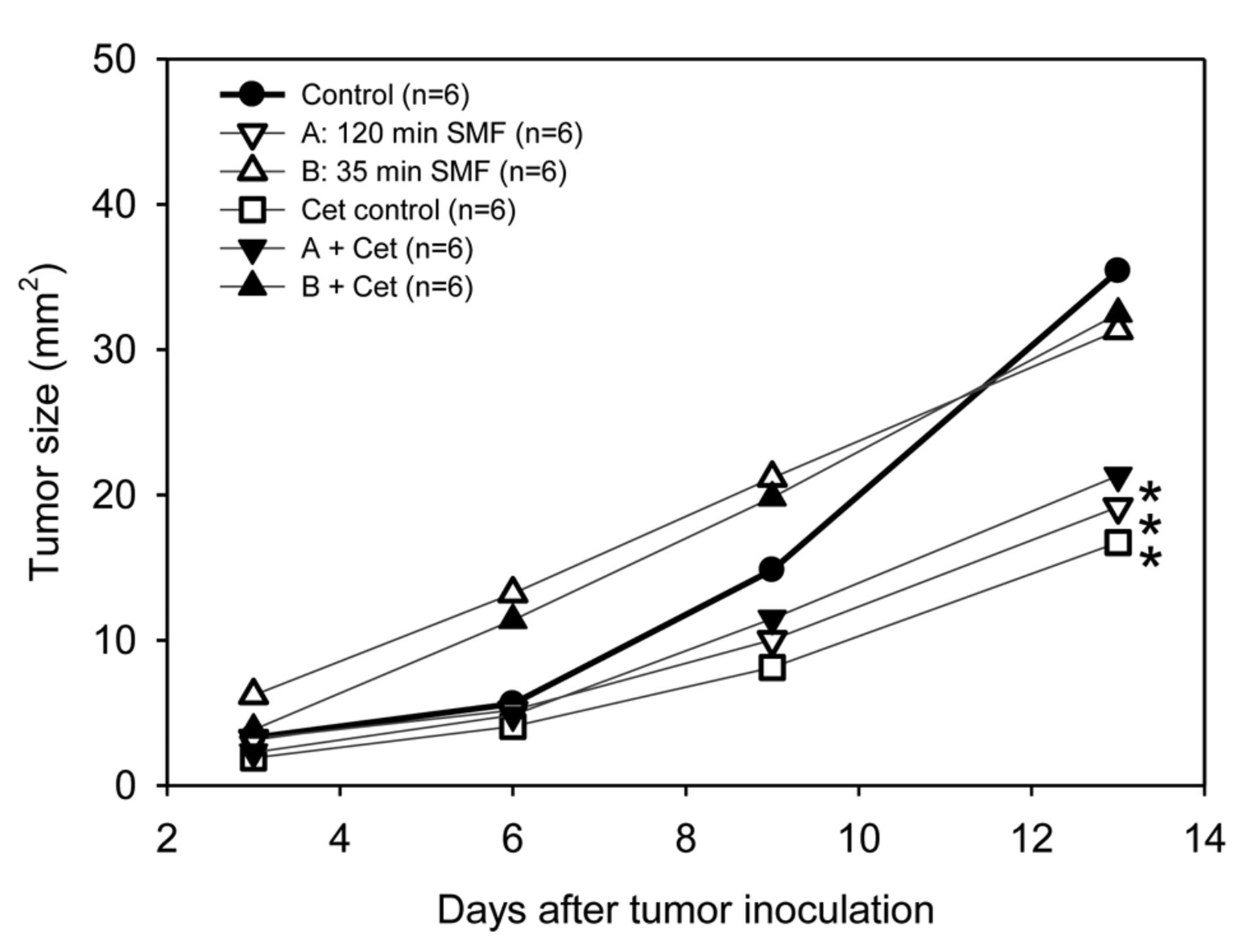
Tumor growth in different treatment groups. At the end of the observation period, the largest tumors were found in control animals, the smallest after cetuximab (Cet) monotherapy. Three-fold static magnetic field (SMF) exposure for 120 min also led to a significant inhibition of tumor growth, however, the addition of cetuximab conferred no further treatment benefit. *Significantly different at p<0.05 vs. control.
Earlier, we clearly demonstrated that changes in microvascular permeability is observed under SMF exposure (19). SMF may be used to open the blood–tumor barrier for concomitant chemotherapy. In the present study, we focused on the effects of a combination of SMF with targeted therapy. Both monotherapies, cetuximab and SMF exposure, resulted in strong tumor growth inhibition. However, the concomitant administration of cetuximab and exposure to SMF revealed interference of both treatment concepts. There is evidence from several in vitro studies that SMF affects the molecular conformation of the EGFR (6, 8). Hence, under SMF exposure, cetuximab may be hindered in blocking the receptor effectively. In the same way that this study provides new evidence for interference between SMF exposure and anti-EGFR therapy, one may speculate that the antitumoral effects of SMF exposure as monotherapy might be the result of SMF-mediated functional blockage of EGFR signaling. Zhang et al. indeed reported that a SMF-induced conformation change of the EGFR hindered receptor dimerization, which is critical for ligand-induced activation of the signaling cascade (8). The underlying molecular mechanism may be an SMF-induced conformational and functional deterioration of the target receptor in tumor cell membranes. Whole cell re-orientations were observed under SMF exposure by Higashi et al. (38); spatial and conformational effects on cells and molecules were also reported elsewhere (39, 40).
Most studies on cetuximab are carried out on human tumor xenografts in immunodeficient mice. In the present study, we used LLC-1, a murine tumor model, in immunocompetent mice. The fact that cetuximab as single agent displayed significant inhibition of LLC-1-growth might be regarded as the proof of concept that the chimeric antibody also acts on murine tumors. However, further studies are necessary to investigate the exact mechanism of action. In addition, the analysis of leukocyte–endothelial cell interactions provided further evidence that the chimeric antibody does not provoke immunological responses in immunocompetent mice: the leukocyte–endothelial cell interactions in immunocompetent animals treated with cetuximab did not differ remarkably compared to immunocompetent controls. Although there are reports on cetuximab increasing cytokine-driven leukocyte infiltration in vitro (41, 42), we were unable to confirm this from our tumor model.
The present study clearly shows how modulation of SMF exposure affects SMF-based carcinoma therapy. Interferences with targeted therapy using cetuximab have to be taken into account in upcoming clinical trials using SMF in EGFR-expressing carcinomas, as for example HNSCCs.
Acknowledgements
This study was supported by an undergraduate funding program (FöFoLe grant 16/2010) of the LMU medical center and by a grant of the foundation ‘Tumorforschung Kopf-Hals’, Wiesbaden. The sponsor had no influence on study design, on collection, analysis or interpretation of data, on the writing of the manuscript and its publication.
Footnotes
This study formed part of the research for the doctoral thesis of the Author Ursula Schmidtmayer.
Conflicts of Interest
The Authors declare no conflict of interest in regard to this study.
- Received May 24, 2018.
- Revision received June 8, 2018.
- Accepted June 11, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.