


Abstract
Background/Aim: To verify perfusion differences in white matter adjacent to glioblastomas and metastatic tumors in dynamic contrast-enhanced (DCE) 3T-magnetic resonance imaging (MRI) using gradient echo (GRE) T1 techniques. Materials and Methods: A retrospective comparative study was carried out on adults with glioblastoma (n=67) and brain metastases (n=31). In each patient, conventional 3T-MRI and DCE-MRI with 25 acquisitions of GRE-T1 were performed. The initial area under the contrast-uptake curve (iAUC) and transfer constant (Ktrans) in peritumoral regions of the white matter were evaluated using T1 pharmacodynamic modeling software. Results: Statistically significantly higher relative iAUC (p<0.001) and Ktrans (p<0.01) values were recorded for peritumoral white matter near glioblastomas compared to that near metastases: 2.29 (SD=1.11) and 2.12 (SD=1.05) vs. 0.96 (SD=0.31) and 1.18 (SD=0.35), respectively. Conclusion: In comparison to Ktrans, the iAUC obtained by DCE-MRI is more suitable for assessing glioblastomas because it better reflects pharmacokinetic peritumoral changes. Increased iAUC in white matter near to tumor generally indicates glioblastoma, however, a low level does not exclude it.
- Glioblastoma
- brain metastases
- dynamic contrast-enhanced
- perfusion
- white matter infiltration
- magnetic resonance
Brain metastases are the most common brain tumors detected in adults. An increase of their incidence has been reported, probably as a consequence of improvement of treatment for primary tumors and detection and diagnosis of brain metastases (1). Lung, breast, colorectal and renal cancer, and malignant melanoma are the most typical sources of brain metastases (2, 3). The most frequent primary brain tumor is glioblastoma multiforme (GBM), the most malignant subtype of neuroepithelial tumor according to the World Health Organization (WHO) classification of tumors (4), with a reported incidence of 3.2/100,000 per year in adults and 5-year overall survival up to 5% (5,6). Early diagnosis and differentiation of GBM and brain metastases contributes to early and very important decision-making processes for further diagnostic and therapeutic options, mostly comprising surgery resection and radiation therapy, and leads to more effective healthcare.
The aim of the study was to verify perfusion differences in white matter adjacent to glioblastomas and metastatic tumors in dynamic contrast-enhanced (DCE) 3T magnetic resonance imaging (MRI) using gradient echo (GRE) T1 techniques.
Materials and Methods
Patients. A retrospective comparable single-center study was carried out of 98 adults (40 men, 58 women) with median age of 65 (35-84) years and with histopathologically confirmed glioblastomas (n=67) or brain metastases (n=31) of lung cancer (n=12), melanoma (n=9), breast cancer (n=5), colorectal cancer (n=2), renal cancer (n=2) or leiomyosarcoma (n=1). Prior to surgical intervention, each patient underwent MRI of the brain at our center within 2012-2017. Patients without clear contrast-enhanced lesions and with acute hemorrhage in the lesion were not included in the study.
Equipment and data acquisition. All examinations were performed on 3T-MRI system (Skyra, Siemens, Erlangen, Germany) by using 20-channel phased-array head coil. Routine examination protocol included transverse fast spin echo T2-weighted imaging (T2 TSE), transverse fluid attenuated inversion recovery T2-weighted imaging (T2 TIRM), transverse and sagittal spin echo T1 weighted imaging (T1 SE), transverse diffusion weighted imaging (DWI). Dynamic contrast enhanced (DCE) was performed after intravenous administration of the contrast agent gadoterate meglumine (Dotarem; Guerbet, Roissy, France) at a dose of 0.1 mmol/kg (=0.2 ml/kg) and flow rate of 2 ml/s. DCE comprised continuous 25 acquisitions of gradient echo (GRE) T1-weighted volumetric-interpolated breath-hold examination imaging (T1 VIBE) with these parameters: TR/TE 5.1/1.9 ms, field of view 199×220 mm, matrix 232×256, in-plane resolution 0.86×0.86 mm, slice thickness 3 mm, time resolution 6.3 s. The DCE was followed by transverse gradient echo 3D T1-weighted imaging (T1 MP-RAGE).
Data processing and statistics. Quantitative perfusion analysis was performed using Tissue 4D syngo (Siemens Healthcare, Erlangen, Germany) software. Values of the vascularization parameter initial area under the contrast-uptake curve (iAUC) and the permeability parameter transfer constant (Ktrans) were measured in a circle-shaped region of interest (ROI) with 10 mm radius, localized in peritumoral white matter and with a distance of 5 mm between the border of the ROI and the border of the contrast-enhanced lesion (see Figure 1). ROIs were selected not to include the gray matter and not to include any visible blood vessels. The measured values for ROIs were divided (normalized) by the values measured on the same image slice in the area of contralateral non-affected healthy white matter ROI (see Figure 1) and thus the relative (normalized) iAUC and Ktrans values were obtained and then statistically analyzed. Normal non-affected healthy appearance of contralateral white matter was verified by means of all the MRI protocol sequences. Statistical analyses were performed using GraphPad InStat (GraphPad Software, San Diego, CA, USA) with unpaired t-test and values p<0.05 were considered as indicating statistically significant differences.
Results
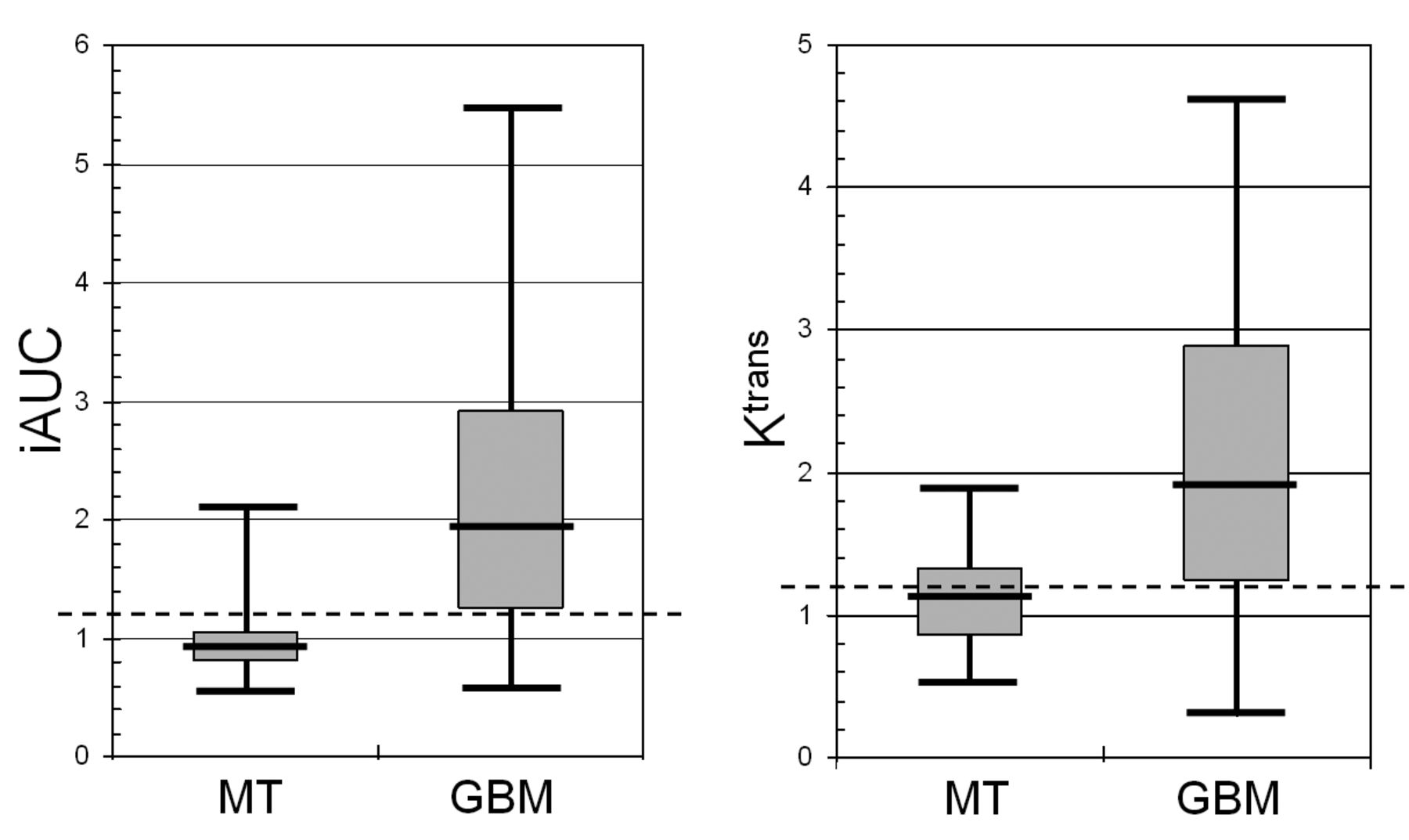
Absolute iAUC and Ktrans values were generally increased in the peritumoral area of GBM. In metastases, the absolute iAUC and Ktrans values were slightly lower or were similar to those measured in the contralateral unaffected healthy white matter (see Figures 1 and 2 for more details). Mean relative iAUC and Ktrans values were statistically significantly higher for peritumoral white matter near GBM compared with metastases: 2.29 (SD=1.11) and 2.12 (SD=1.05) vs. 0.96 (SD=0.31) and 1.18 (SD=0.35), p<0.001 and p<0.01, respectively.
A threshold of 1.2 or more for relative iAUC and Ktrans was arbitrarily assigned to define GBM, and indicated 20% higher values of these parameters compared to those for healthy white matter. Using relative iUAC and Ktrans values in detecting glioblastomas, there were 52/67 and 53/67 true-positive cases, sensitivity of 77.6% and 79.1%, specificity of 83.9% and 48.4%, positive predictive value of 91.2% and 76.8%, and negative predictive values of 63.4% and 51.7%, respectively.
Discussion
Brain metastases usually have very well-defined and clearly circumscribed margins, regardless of the large heterogeneity of their primary solid tumors. The maximum depth of brain tissue infiltration with malignant metastatic cells is observed in small-cell lung cancer and melanoma, however, the distances do not exceed approximately 1 mm from the anatomically defined margins of metastases (7, 8). Usually, there is also vasogenic edema present in the area surrounding metastases and this leads to restriction of blood perfusion according to the level of edema (9). For GBM on the other hand, very aggressive infiltrative growth is typical (10). Malignant cells invade mostly individually or in small groups alongside tracks of myelinated fibers in white matter, in perivascular, perineuronal and subpial spaces, and these malignant cells can histopathologically be found even several centimeters from the anatomically defined tumor (11, 12). Very often in GBM, there is also high expression of vascular endothelial growth factor, which is the main cause of vasodilatation, neovascularization and high microvascular permeability of tumor (13, 14). The extent of neovascularization determines the biological aggressiveness of the tumor.
In brain tumors, conventional non-dynamic MRI with administration of contrast agent uses the effect of blood–brain barrier disruption, and that is why contrast enhancement is not present in the whole tumor mass, but only in areas with preserved vascular circulation together with those with blood–brain barrier disruption. In GBM, this phenomenon is usually in the form of an irregular ring-like rim around central necrosis. Diffuse infiltration with tumor cells near the rim, not yet causing blood–brain barrier disruption and contrast leakage into the cerebral interstitial tissue, combined with vasogenic edema, is not visible in conventional MRI. However, the presence of tumor cell infiltration in this phase leads to vascular changes that are apparent as increased vessel caliber and neovascularization, with increased perfusion in surrounding areas (15, 16). The changes of perfusion parameters in areas surrounding GBM, and thus the indirect detection of its infiltrative growth, can be distinguished by dynamic post-contrast imaging. Results of our analysis correlate well with GBM-related circulatory and vascularization characteristics and parameters. The white matter peritumoral changes were better represented by iAUC values, which reflect the inflow of contrast agent into the region of interest within 60 seconds of its i.v. administration, and represent vascular perfusion. In contrast, Ktrans is a calculated parameter obtained from a two-compartment exchange model, and reflects the combined characteristics of blood flow, vascular space volume and permeability (blood–brain barrier disruption) (17, 18). Increased blood perfusion in the area of GBM has also been described in several smaller groups of patients who were examined by dynamic susceptibility-weighted contrast-enhanced (DSC) MRI (19, 20). Mathematic models used in DSC methods presume full integrity of the blood–brain barrier, and cannot be used to investigate capillary leakage, which is why permeability (blood–brain barrier disruption) is not taken into consideration in this situation. In comparison, DCE MRI has an advantage in its capability to quantify microvascular permeability and characterize the tumor tissue. Quantitative measurement of microvascular permeability in human brain tumors achieved using DCE MRI correlates with histological grade (21) and helps find the most suitable location for targeted biopsy.
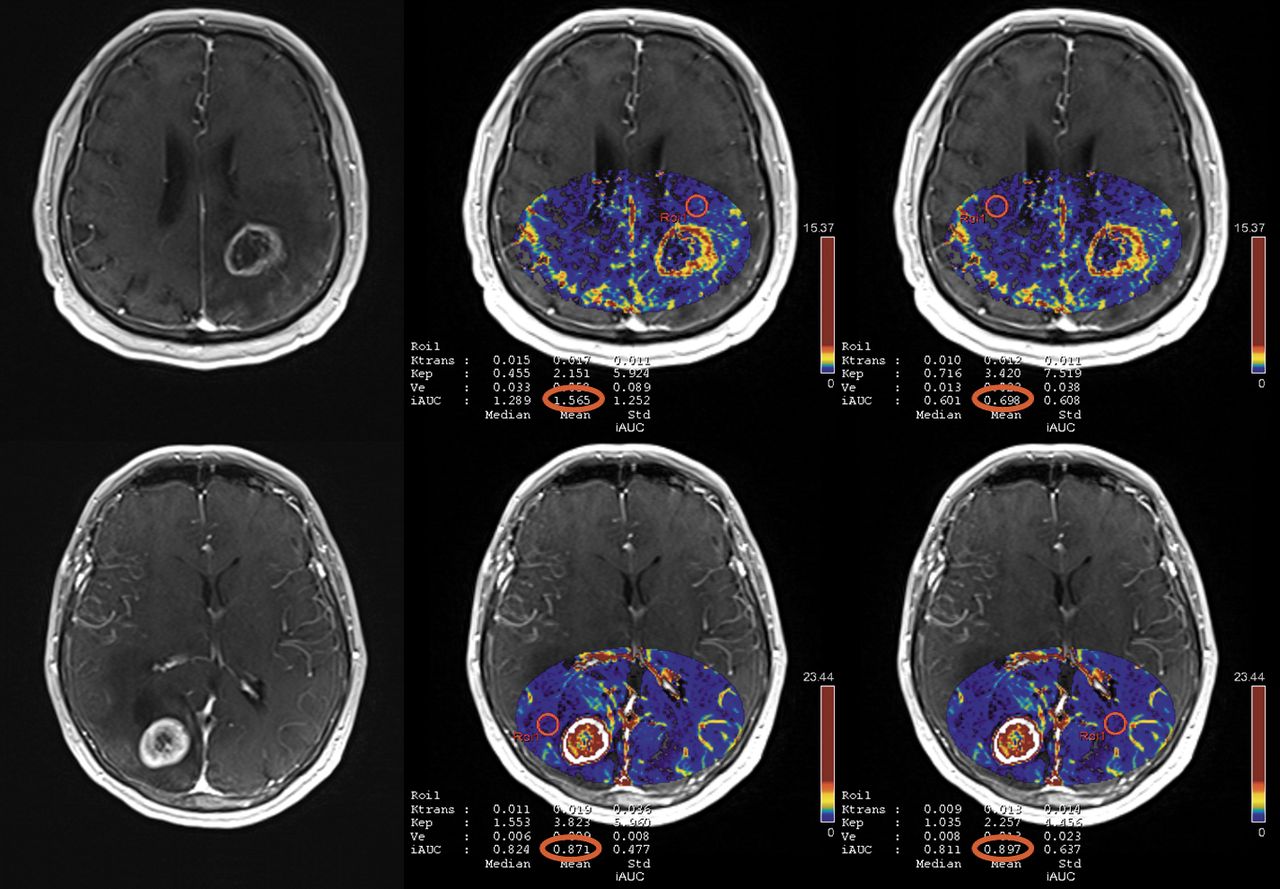
Imaging of glioblastoma (upper panel) and breast cancer metastasis (lower panel). T1 Volumetric interpolated breath-hold examination (VIBE) image with contrast-enhanced ring lesions (left hand images), T1 VIBE fusion with maps of initial area under the contrast-uptake curve with region of interest located in peritumoral (middle images) and contralateral healthy white matter area (right hand images).

Distribution of relative values of initial area under the contrast-uptake curve and transfer constant measured in the peritumoral area of brain metastases (MT) and glioblastoma multiforme (GBM).
In the case of treated brain tumors, DCE MRI differentiates pseudoprogression from recurrent GBM (22). DCE MRI allows better quantification of perfusion parameters using less volume of contrast agent (17, 23).
In order to minimize the influence of artefacts and to standardize measurement methods in our study, a rather large ROI was used to assess perfusion parameters. In some cases, it was rather difficult to find a standardized ROI fulfilling all the demands defined by the study protocol (i.e. diameter, distance, white matter not containing grey matter nor vessels). The low negative predictive value of the test was probably influenced by highly heterogeneous GBM growth, whereby various parts of the tumor may present various and different biological characteristics ranging between infiltrative and non-infiltrative tumor growth (12) and with variable changes in circulatory and vascularization. We can postulate that in daily practice, the finding of even a small peritumor area with a high iAUC value may lead to significant suspicion of GM.
Conclusion
Different perfusion characteristics in peritumoral matter in glioblastomas and brain metastases are detectable with post-contrast perfusion T1 MRI. The iAUC obtained by DCE-MRI is more suitable to assess glioblastoma because it better reflects its neovascularisation compared to Ktrans and can help better distinguish glioblastoma and metastases. Increased iAUC values measured in the area near by contrast enhanced tumor mostly indicate glioblastoma, however, low iAUC value does not exclude it. DCE-MRI and its analysis should always be a part of pre-surgical focal brain lesions examination protocol.
Acknowledgements
Supported by the Ministry of Health, Czech Republic for conceptual development of research organization 00669806 – Faculty Hospital in Pilsen, Czech Republic and Charles University Research Fund (project P36).
- Received April 18, 2018.
- Revision received May 14, 2018.
- Accepted May 16, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.