


Abstract
Background/Aim: Only 30-50% of patients with sentinel lymph node (SLN) metastases present with further axillary lymph node metastases. Therefore, up to 70% of patients with positive SLN are overtreated by axillary dissection (AD) and may suffer from complications such as sensory disturbances or lymphedema. According to the current S3 guidelines, AD can be avoided in patients with a T1/T2 tumor if breast-conserving surgery with subsequent tangential irradiation is performed and no more than two SLNs are affected. Additionally, use of nomograms, that predict the probability of non-sentinel lymph node (NSLN) metastases, is recommended. Therefore, models for the prediction of NSLN metastases in our defined population were constructed and compared with the published nomograms. Patients and Methods: In a retrospective study, 2,146 primary breast cancer patients, who underwent SLN biopsy at the University Women's Hospital in Tuebingen, were evaluated by dividing the patient group in a training and validation collective (TC or VC). Using the SLN-positive TC patients, three models for the prediction of the likelihood of NSLN metastases were adapted and were then validated using the SLN-positive VC patients. In addition, the predictive power of nomograms from Memorial Sloan Kettering Cancer Center (MSKCC), Stanford, and the Cambridge model were compared with regard to our patient collective. Results: A total of 2,146 patients were included in the study. Of these, 470 patients had positive SLN, 295 consisted the training collective and 175 consisted the validation collective. In a regression model, three variants – with 11, 6 and 2 variables – were developed for the prediction of NSLN metastases in our defined population and compared to the most frequently used nomograms. Our variants with 11 and with 6 variables were proven to be a particularly suitable model and showed similarly good results as the published MSKCC nomogram. Conclusion: Our developed nomograms may be used as a prediction tool for NSLN metastases after positive SLN.
- Breast cancer
- sentinel lymph node metastases
- nomogram
- prediction tool
- non-sentinel lymph node metastases
Breast cancer is one of the primary lymphatic metastasizing tumors. Twenty percent to 47% of breast cancer patients have regional lymph node metastases at initial diagnosis (1-9). According to current guidelines, nodal status of patients with clinically node-negative primary breast cancer should be determined using sentinel lymph node biopsy. If the sentinel lymph nodes are affected, axillary dissection usually follows, which is associated with higher morbidity. It can lead to sensory disturbances, pain, lymphedema and limitations in mobility and strength (10-13). However, 50-70% of SLN-positive patients have no further metastases in non-sentinel lymph nodes (6, 14-20). In these cases, axillary dissection is over-treatment with increased patient morbidity. The Z0011 study (21) showed that in a defined patient group with positive sentinel lymph nodes, no statistically significant difference in locoregional recurrence is observed between patients with sole sentinel lymph node biopsy and patients with sentinel lymph node biopsy followed by axillary dissection. Other studies also found that axillary dissection has no further survival benefit in defined patient groups (22-27). Thus, axillary dissection can be avoided in patients with T1 or T2 tumor and no more than two affected sentinel lymph nodes if breast-conservation surgery with subsequent tangential irradiation is performed. However, this patient group may not be sufficiently defined and other criteria for decision making are warranted.
Various nomograms are described in the literature that calculate the likelihood of further non-sentinel lymph node involvement if lymph node biopsy is positive (6, 15, 17, 19, 20, 26-32). However, the predictive power of nomograms may differ within different patient collectives. For this reason, we compared the power of nomograms from Memorial Sloan Kettering Cancer Center (MSKCC), Stanford, and Cambridge University in a patient collective from a large German breast center. We moreover developed a regression model for predicting non-sentinel lymph node metastases and compared our model with the earlier nomograms.
Patients and Methods
Data from 3,005 patients with primary breast cancer and clinically unremarkable axilla were analyzed in this retrospective study. These patients underwent sentinel lymph node biopsy at the University of Tuebingen Women's Hospital between 2005 and 2012 as part of their primary surgery. A total of 859 patients were excluded due to exclusion criteria such as bilateral breast cancer, distant metastases, relapse, neoadjuvant chemotherapy and carcinoma in situ. The 2146 remaining patients were divided into a training collective (2005-2009) and validation collective (2010-2012), depending on the date of surgery. Breast cancer was histologically confirmed preoperatively in all patients. Of the 2,146 patients enrolled, 470 patients (22%) had positive sentinel lymph nodes, 295 (23%) included in the training group and 175 (20%) included in the validation group (Figure 1). The data from these SLN-positive patients were used for training and validation; the histology result from the non-sentinel lymph node biopsy served as the gold standard.
Histopathological evaluation. In a frozen section biopsy, the tissue was cut in 2 mm slices perpendicular to the longest axis, frozen in OCT freezing medium at −20°C and cut in the cryostat. A section was taken, the tissue cut into 200-μm layers and applied to coated specimen slides. The sections were then stained with hematoxylin/eosin (HE) and examined straight away. The result was immediately transmitted by telephone to the operating theatre. The tissue was subsequently fixed in formalin for at least 24 h. To increase the detection rate of metastases, from March 2008 complete processing was carried out in layered sections at 500 μm intervals. Each layered section was stained with HE and viewed using conventional light microscopy. In addition, one unstained slide was saved for every level, for potential immunohistochemistry. Suspicious areas were examined using immunohistochemical detection of cytokeratin-positive cells (antibodies AE1/AE3). Up to March 2008, two layered sections were produced which were 200μm apart. These were stained with HE and viewed using conventional light microscopy. If the metastasis test was negative, an immunohistochemical study was carried out with anti-cytokeratin antibodies (AE1/AE3) and two successive layered sections were prepared for HE examination.
Data analysis. Data was collected in SPSS Version 15.0 (SPSS Inc. Released 2006. SPSS for Windows, Version 15.0. Chicago, SPSS Inc.). Statistical analysis was performed using R Version 3.0.0 (R Foundation for Statistical Computing, Vienna, Austria, 2013). Demographic and cancer characteristic data are presented as numbers and percentages, respectively, and means with standard devi¬ations. To compare groups, Wilcoxon rank and Fisher exact tests were used, respectively. A significance level of 5% was chosen.
Using the training samples, a multiple logistic regression model for NSLN status was formulated for NSLN positivity. Candidate variables are the univariate significant ones and factors of medical interest. Variables were chosen by backward and forward selection (F-to-enter=0.1).
The probabilities of positive NSLN predicted by MSKCC (20) and Stanford nomograms (6) are available via online forms. To obtain them for our data, we implemented a Java program (JDK version 5, Apache httpclient version 4.1.1 and jdom version 1.1) to generate http posts and extract the returned values. The parameters of the Cambridge regression model (19) were also applied to our data.
For all models resp. nomograms and area-under-the-curve (AUC) values are given with 95% confidence intervals for the training and validation samples. In all cases, the gold standard is the result of auxiliary dissection of NSLN.
Results
Univariate analysis. The training collective showed a statistically significant association between non-sentinel lymph node metastases and tumor size in cm (p<0.001), number of tumor-affected SLN (p=0.004) or proportion of positive SLN (p<0.001), micro- vs. macrometastases (p=0.001) or size of lymph node metastases in cm (p=0.004), lymphangitis carcinomatosa (p=0.004), multicentricity (p=0.015), and capsular invasion (p=0.003). In addition to these variables, the tumor characteristics, histological tumor type, grading, ER-status, PR-status and Her2 status established in clinical practice were analyzed, none of which showed a significant correlation (Table I). All SLNs were examined using frozen section biopsy stained with hematoxylin/eosin and additional immunohistochemical detection of cytokeratin-positive cells (antibodies AE1/AE3) was performed in 76 (26%) SLN-positive patients
Logistic regression model. In order to estimate the maximum prognostic potential, a logistic regression model for NSLN positivity was started with all the selected characteristics. Since the characteristic micro-/macrometastasis is only the categorization of the lymph node metastasis size in cm, these two are highly correlated and to avoid multicollinearity, only one of them should be included in the model. Similarly, either the number of SLNs removed and the number of tumor-affected SLNs, or the proportion of tumor-affected SLNs amongst all the removed SLNs can be taken into account. After various preliminary studies, model C was selected as the starting point (Table II), with the eleven characteristics of tumor size, proportion of positive SLNs, SLN-metastasis size, tumor type, grading, ER-status, PR-status, Her2 status, lymphangitis carcinomatosa, multicentricity and capsule infiltration (see Figure 2 for overview). Forward selection (F-to-Enter=0.1) resulted in a reduced model variant A with the 6 features of tumor size, proportion of positive SLNs, SLN metastasis size, lymphangitis carcinomatosa, multicentricity and capsule infiltration. This model variant also results from backward selection (F-to-leave=0.1). For comparison, a model variant B with the two strongest predictors of tumor size and proportion of positive SLNs was considered.
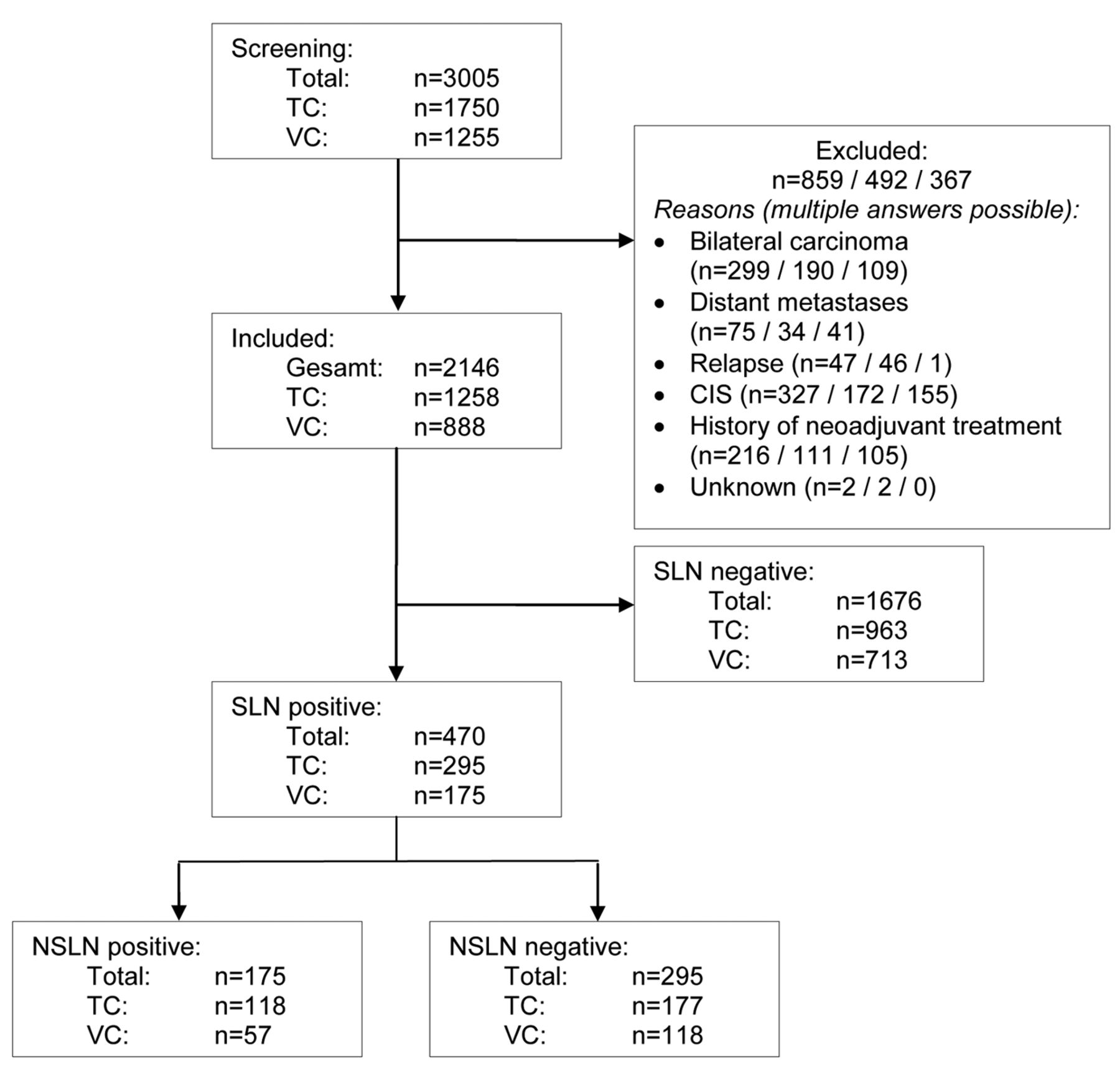
Representation of the patient collective. SLN: Sentinel lymph node; NSLN: non-sentinel lymph node; TC: training collective; CV: validation collective.
Figure 3 shows that the Receiver-Operating-Characteristic (ROC)-curves of variants A and C, i.e. with eleven or six variables differ surprisingly little in the training collective with “area under curve” (AUC) values of 0.78 [0.72, 0.83] and 0.75 [0.70, 0.81] (Table III). As expected, the AUC values are lower in the validation collective and they are virtually the same at 0.73 [0.65, 0.81] and 0.73 [0.65, 0.81] (Table III). Model B, with only two characteristics, leads to recognizably lower AUC values of 0.70 [0.64, 0.75] in the training collective or 0.64 [0.56, 0.72] in the validation collective. Table IV shows the estimated parameter values of model A with 6 variables.
Comparison with established nomograms. In the ROC curves of the established nomograms (Figure 2), it becomes clear that the MSKCC nomogram provides the best predictions, both for the training and the validation collective. This becomes even clearer for the AUC values: The AUC values of the MSKCC nomogram are virtually identical and highest for the training and validation collectives at 0.73 [0.68, 0.77] and 0.73 [0.66, 0.80] respectively, and lower and differing for the Stanford nomogram at 70 [0.65, 0.74] (TC) and 0.66 [0.58, 0.73] (VC) respectively. Finally, the AUC values are lowest in the Cambridge model, at 0.63 [0.57, 0.69] (TC) and 0.64 [0.52, 0.76] (VC) respectively.
Characterization of the patients.
Although the AUC values of our regression model are higher in the training collective than in the MSKCC nomogram, at least for the variants with 11 and with 6 characteristics, this is not demonstrated in the validation collective where they are the same.
Discussion
Sentinel lymph node biopsy is an established procedure for the determination of nodal status in patients with primary breast cancer and clinically unremarkable axilla. If the sentinel lymph nodes are tumor-free, axillary dissection can be avoided. This method results in a significant reduction in morbidity and improved quality of life. However, the question of the optimal procedure in the case of positive sentinel lymph nodes arises. More than half of the patients with positive sentinel lymph nodes do not benefit from the currently recommended axillary dissection, since 50-70% of SLN-positive patients have histologically-negative non-sentinel lymph nodes. In order to predict which patients do not benefit from axillary dissection, we developed three models which are valid for the German population to predict non-sentinel lymph node metastases. These were validated using a further patient collective and compared with already published nomograms with regard to their predictive power.
In some studies, an increase in the predictive power could be achieved by including other characteristics which were not statistically significant in this study group (20, 33). Therefore, the model with 11 characteristics also contains variables which are not significantly associated with non-sentinel lymph node metastases in our study collective, but which are important tumor characteristics in clinical practice. This model has the highest AUC value (0.78) in the training collective. The model variant B with 2 variables has the lowest predictive power (AUC value 0.70), but this value is remarkably high considering that it only has two features.
The AUC values of our model in the validation collective were lower, as expected. Interestingly, the AUC values of the model variants with 11 and 6 variables in the validation collective are very close together with a value of 0.73. Thus, the model with 6 variables requires less information; However, it provides a similarly good predictive value.
The correlation of the tumor characteristics selected with non-sentinel lymph node metastases has been investigated in many studies. The most common feature of the primary tumor which was used is the tumor size. This feature was included in both the MSKCC (20) and the Stanford nomogram (6). We also observed that the tumor size was significantly associated with the occurrence of non-sentinel lymph node metastases (p<0.001) in our study population. This relationship is confirmed by numerous other publications (1, 15, 17, 32, 34-37) and the local tumor load appears to have a relevant influence on the development of axillary lymph node metastases. Lymphangitis carcinomatosa is also one of the most important influencing factors. If the tumor is able to infiltrate the lymphatic vessels, the probability for non-sentinel lymph node metastases increases. This important feature has also been included in the MSKCC (20) and the Stanford nomograms (6). Several papers have been referenced in the literature showing the influence of lymphangitis carcinomatosa on lymphatic spread (17, 30, 32, 36-37). Our study confirmed this relationship. Nevertheless, lymphangitis carcinomatosa is not taken into account in the Cambridge model (19).
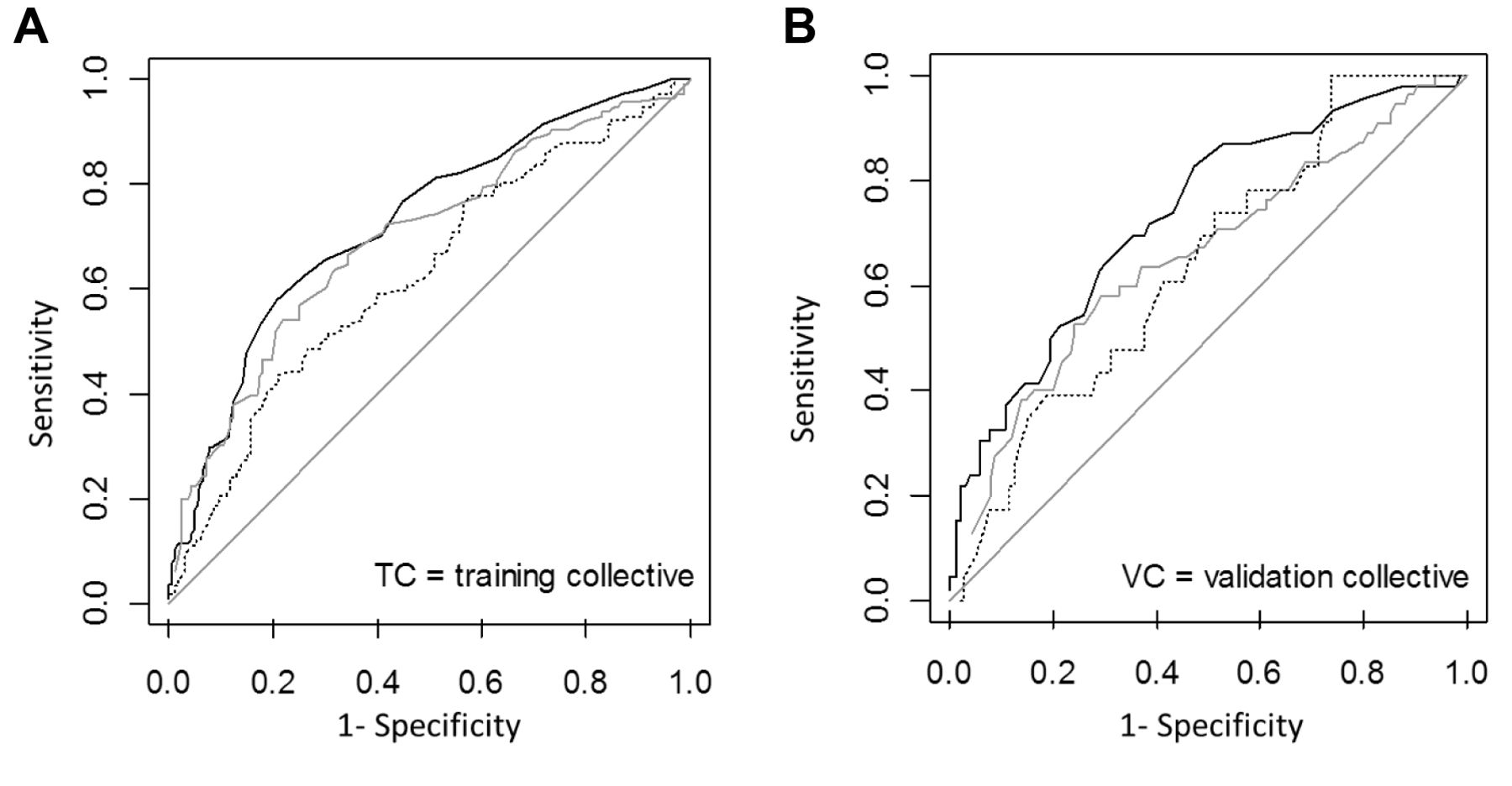
ROC curves for MSKCC (black), Stanford (grey) and Cambridge (dotted) nomograms for training (A) and validation collective (B).

ROC curves of the logistic regression model variant A (black), B (grey) and C (dotted) on the training (A) and validation collective (B).
Considering the influencing factors affecting sentinel lymph node metastases, it can be seen that the tumor load is decisive. Two features are important here. According to the above-mentioned size of the primary tumor, the size of the sentinel lymph node metastasis also increases the likelihood of further lymph node involvement (15-17, 19, 30, 32, 35); these are also taken into account in the Cambridge and Stanford nomograms. This characteristic was not included in the MSKCC nomogram because the criteria for the determination of the metastasis size were not standardized in the MSKCC at the time, especially in the case of several smaller cell clusters. This relationship was also confirmed in our study. The increasing proportion of tumor-affected sentinel lymph nodes also increases the tumor mass and therefore the probability of non-sentinel lymph node metastases. This tumor behavior was confirmed both in numerous studies (1, 15, 17, 30, 32, 34) and in our study. The feature is also taken into account in the MSKCC (20) and the Cambridge nomogram (19). In the Stanford nomogram (6), the proportion of tumor-affected sentinel lymph nodes was not analyzed, but the number of removed and the number of tumor-affected sentinel lymph nodes were differentiated. However, these characteristics were not included in the model. The ability of the tumor to infiltrate the lymph node capsule is associated with further lymph node metastases (15, 17, 32, 35, 37). In the Cambridge model, however, this feature was not taken into account. In publications on the Stanford and MSKCC nomogram, capsule infiltration was not investigated. In our study, a significant association was observed regarding non-sentinel lymph node metastases.
Overview of variables in nomograms and logistic regression models.
Multicentricity is controversially discussed in the literature. Some studies, such as the Helsinki nomogram (17), show that this feature significantly affects the presence of non-sentinel lymph node metastases; in others, multicentricity is referred to as a marginally significant characteristic (20). In other studies, such as the Cambridge (19) and MDA (32) nomograms, multicentricity is not rated as significant. The Stanford nomogram does not include this characteristic. The occurrence of the tumor was divided into unifocality, multifocality and multicentricity in our study. The difference between multicentric and unifocal tumors is statistically significant.
Grading is another established prognostic factor. It is included in the Cambridge model (19) and in the univariate analysis in the development of the Stanford nomogram (6), a significant influence of the grade on the non-sentinel lymph node metastases could be shown. However, other studies failed to confirm this link (17, 20, 32, 37). In our study, the grading does not appear to have any influence on non-sentinel lymph node metastases (p=0.483 or p=0.418).
AUC values of all analyzed nomograms and models in comparison.
As our data and the results of other studies have shown, ER, PR, and Her2 status appear to play a minor role in the development of non-sentinel lymph node metastases (6, 19, 20, 32, 37, 38). Therefore, tumor load rather than tumor biology appears to be important in the development of lymph node metastases.
Logistic regression model A (6 variables).
The following summary can be made. All the features included in the Stanford nomogram were also significant in our study. In the publication on the MSKCC nomogram, the size of the lymph node metastases and capsule infiltration were unfortunately not investigated. Grading, histological tumor type and estrogen receptor status showed no statistically significant effect on non-sentinel lymph node metastases here; however, they were used to increase the predictive power of the MSKCC nomogram. The results of the Cambridge model differ from the results of many other studies in several points. Basically, our results show many similarities, particularly with the Stanford and MSKCC nomograms, which indicates the stability of the results.
We compared our newly created models with the already published nomograms regarding prediction and clinical application. The best AUC values in the validation collective of AUC=0.73 came from our model variants with 11 and with 6 variables and the MSKCC nomogram. Our model variant with 11 variables is the most extensive. The highest possible predictive power should be achieved by including as many variables as possible. However, this model is the most complex in its application. By limiting the number of variables in the variant with 6 variables, the user-friendliness could be improved. As already mentioned, this reduction does not have a major effect on the predictive power of the model. Therefore, this model can be particularly highlighted. Nine variables must be specified when using the MSKCC nomogram. Thus, it is the second most extensive nomogram tested in our study. A disadvantage of using of the MSKCC nomogram is the restricted value range for the input of the variable values. The number of removed sentinel lymph nodes is limited to 7 in the MSKCC nomogram, for example. For this reason, the probability of NSLN metastases cannot be predicted for all patients. However, the online calculator is workable in everyday clinical practice and is, therefore, an advantage of this nomogram.
As expected, the AUC values of the validation collective in our regression model variants are somewhat lower than those of the training collective because the models have been adapted to this (Table III). Such an effect is not expected in the MSKCC and Stanford nomograms and the Cambridge model. For the MSKCC nomogram and the Cambridge model, the AUC values are virtually the same and are slightly different in the Stanford nomogram. The difference between the values of the training and validation collectives is smaller for the regression model variant with 6 characteristics than for the variant with 2 characteristics, which is also expected. The confidence intervals of the validation collective are larger in all cases, which is also expected due to the slightly smaller sample size.
Among the standard nomograms, the MSKCC nomogram had the highest AUC values and is also the nomogram with the best predictive power. The Stanford nomogram lays in the middle, the Cambridge model is the weakest.
When using the nomograms, it is important to note that the nomogram calculates the probability of non-sentinel lymph node metastases. The decision whether axillary dissection should be performed should take into account further clinical factors like age, accompanying diseases and the application of adjuvant systemic treatment (17, 20).
Conclusion
A model for the prediction of non-sentinel lymph node metastases in three variants was developed and compared to the most frequently used nomograms. The variants with 11 and with 6 variables are particularly suitable models. Among the published nomograms, the MSKCC nomogram shows similarly good results.
Footnotes
↵* These Authors contributed equally to this study.
Conflicts of Interest
The Authors declare that they have conflicts of interest regarding this study.
- Received May 14, 2018.
- Revision received June 5, 2018.
- Accepted June 6, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.