


Abstract
Immunotherapy with monoclonal antibodies against programmed cell death (PD-1), such as nivolumab and pembrolizumab, has significantly improved the survival of patients with metastatic non-small cell lung cancer (NSCLC). In order to determine the subset of patients that can benefit most from these therapies, biomarkers such as programmed death ligand-1 (PD-L1) have been proposed. However, the predictive and prognostic role of the use of PD-L1 is controversial. Anti-PD-L1 immunohistochemistry may not represent the actual status of the tumour because of individual variability and tumour heterogeneity. Additionally, there may be analytical variability due to the use of different assays and antibodies to detect PD-L1. Moreover PD-L1 expression is also regulated by oncogenic drivers in NSCLC, such as epidermal growth factor receptor (EGFR), echinoderm microtubule-associated protein-like 4 (EML4) fusion with anaplastic lymphoma kinase (ALK), and Kirsten rat sarcoma viral oncogene homolog (KRAS). Preclinical studies have shown the potential role of targeted therapy in immune escape mechanisms in NSCLC cells. This review summarizes current literature data on the heterogeneity of PD-L1 expression and the relationship with such factors and with clinicopathological features of NSCLC.
- Programmed death ligand-1 (PD-L1) expression
- programmed cell death (PD-1)
- lung cancer
- immunotherapies
- NSCLC
- review
Lung cancer is the second most common tumour in both men and women, while it is by far the leading cause of cancer-related deaths in both genders in Europe. This tumour is classified into two major clinicopathological groups: small cell lung carcinoma and non-small cell lung carcinoma (NSCLC). Approximately 80% of lung cancers are NSCLC and more than 70% of patients with NSCLC are diagnosed with locally advanced or metastatic disease. Although platinum-based combination chemotherapies have been the first-line standard treatment for many years, molecular advances have brought new therapy options, such as epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) and anaplastic lymphoma kinase (ALK)-directed therapies for specific subset of patients with tumours that carry specific alterations (EGFR mutations or ALK translocations). Despite all the progress in drug development, the 5-year survival rate of patients at all stages is still considered relatively low (17.4%) (1). Therefore, there is great interest in new treatment strategies. Thus, immunotherapy is considered a new and very promising therapeutic option. Some of these new therapies are based on monoclonal antibodies that are designed to target immune-checkpoint molecules such as programmed cell death protein 1 (PD-1) or its ligand (PD-L1).
PD-1, a member of the CD28 family, is a key immune-checkpoint receptor expressed on the surface of activated T-, B-, and natural killer (NK) cells and plays a crucial role in tumour immunoescape. Its ligand PD-L1 is up-regulated in different types of tumours and binds PD-1 to reduce immunoresponses. PD-L1 is expressed in 19.6% to 65.3% of cases of NSCLC and positivity rates range from 13% to 70% (2, 3). The expression of PD-L1 assessed by immunohistochemistry (IHC) has been correlated with response and overall survival of patient treated with immune-checkpoint inhibitor therapies in NSCLC, such as nivolumab and pembrolizumab, two antibodies targeting PD-1 (4-7). However, its significance remains unclear and controversial (8). IHC using antibody to PD-L1 may not represent the true status of the tumour because of heterogeneity of expression (9, 10) due to various factors, such as stage of disease, prior chemotherapy (11, 12) or targeted therapy (13), prior radiotherapy (14, 15), gender, associated concomitant medications e.g. steroids, viral infection (16, 17), mutation status of NSCLC, tumour differentiation, histology, the presence of CD8+ tumour-infiltrating lymphocytes (TILs) (18-21), differences in diagnostic sample type (e.g. cytology, large tumour tissue, small biopsy sample) and different assay methods (22, 24) used to detect PD-L1 level, subsequently with inter-assay variability or discordance (25-31) (Table I).
PD-L1 Expression and Prognostic Value in Lung Cancer
Pan et al. showed the association between high PD-L1 expression in NSCLC and poor tumour differentiation [well-/moderately vs. poorly differentiated, odds ratio (OR)=0.53, 95% confidence interval (CI)=0.39-0.72, p<0.0001]. This meta-analysis concluded PD-L1 expression to be a poor prognostic factor for overall survival (OS) [positive vs. negative PD-L1 expression, hazard ratio (HR)=1.47, 95% confidence interval (CI)=1.19-1.83, p=0.0004] (32). Mu et al. studied the association of expression level of PD-L1 in lung cancer with histology and OS. The rate of expression of PD-L1 in adenocarcinoma was higher than in the squamous cell variant (65.2% vs. 44.4%, p=0.032) and PD-L1-positive NSCLC cells were associated with a poor prognosis. Patients with survival time after surgery of less than 3 years had a higher PD-L1 expression rate (p=0.034) (33).
The analysis of four pivotal adjuvant chemotherapy trials (IALT, ANITA, JBR.10 and CALGB 9633) conducted by the LACE-Bio (Lung adjuvant Cisplatin Evaluation Biomarker) collaborative group showed that PD-L1 IHC is neither a prognostic factor nor a predictor of survival benefit from adjuvant chemotherapy in early-stage completely resected NSCLC (34). Whole-exome sequencing analysis of early-stage lung adenocarcinoma revealed that PD-L1 was the most elevated immune marker in smokers (p=0.006) and that PD-L1 expression level was positively correlated with somatic mutation burden (35).
Sheng et al. described the impact of neoadjuvant chemotherapy on PD-L1 expression of tumour cells and tumour-infiltrating immune cells (36). The rate of positive PD-L1 expression changed from 75% to 37.5% after neaoadjuvant treatment (p=0.003). A subgroup analysis showed that patients receiving TKIs (erlotinib, gefitinib or icotinib) (p=0.004) or taxane-based chemotherapy (p=0.006) tended to exhibit PD-L1 reduction, but those who received pemetrexed-based regimens did not. Patients who responded to chemotherapy presented reduced PD-L1 levels in tumour cells (p=0.004). The switch from negative to positive PD-L1 status was associated with inferior disease-free survival (DFS) when compared with the contrary change (median DFS=9.6 vs. 25.9 months, p=0.005).
McGranahan et al. showed that a higher somatic mutation burden was associated with improved objective response rate (ORR=63% vs. 0%, p=0.03), durable clinical benefit (p=0.02) and progression-free survival (PFS=14.5 vs. 3.7 months, p=0.01, HR=0.19, 95% CI=0.05-0.70) in patients with NSCLC treated with pembrolizumab. Molecular signature of smoking due to tobacco carcinogen-related mutagenesis (ORR=56% vs. 17%, p=0.03; durable clinical benefit=77% vs. 22%, p=0.004; median PFS not reached vs. 3.5 months; p=0.0001), higher neoantigen burden (median PFS=14.5 vs. 3.5 months, p=0.002) and DNA-repair pathway mutations [polymerase delta 1 (POLD1), polymerase ε (POLE), DNA mismatch-repair protein (MSH2), protein kinase DNA-activated catalytic polypeptide (PRKDC), and cell-cycle checkpoint protein RAD17) were associated with higher efficacy and mutation burden (37).
McGranahan et al. showed correlation between a high neoantigen burden and longer OS in lung adenocarcinoma (p=0.025). In early-stage NSCLC, the neoantigens were associated with an inflamed tumour microenvironment enriched with activated CD8+ T-cells, subsequently expressing high levels of PD-L1. Advanced NSCLCs treated with pembrolizumab with a high clonal neoantigen burden and low neoantigen intra-tumoural heterogeneity were associated with a higher PD-L1 expression, resulting in a longer PFS (38). Okita et al. found that PD-L1 overexpression was associated with male sex (p=0.004), smoking history (p=0.002), higher maximum standardized uptake value (SUVmax) on positron-emission tomography (p<0.001), squamous cell carcinoma histology (p=0.003), higher histological grade (p=0.003), node metastasis-positive status (p=0.015) and advanced pathological stage in resected NSCLC (p=0.014) (Table I) (45).
PD-L1 Expression and Oncogenic Drivers
Several studies showed that PD-L1 expression is also regulated by oncogenic drivers in NSCLC, such as EGFR, echinoderm microtubule-associated protein like 4 (EML4–ALK), proto-oncogene tyrosine-protein kinase ROS (ROS1), KRAS, tumour protein p53 (TP53), mesenchymal-to-epithelial transition (MET) and phoasphatidylinositol-4,5 bisphosphate 2-kinase catalytic subunit alpha (PIK3CA) (39).
EGFR Pathway
Several studies showed that EGFR pathway activation was associated with higher PD-L1 expression (40-43). It has been shown that EGFR-mutant NSCLC cell lines compared to EGFR wild-type (WT) cell lines have a significantly higher protein expression of PD-L1. EGFR activated by EGF stimulation, exon-19 deletion and L858R mutation induced PD-L1 expression, suggesting that constitutive oncogene pathway activation can up-regulate PD-L1. EGFR activation up-regulated PD-L1 through p-ERK1/2/p-c-JUN, which are involved in proliferation, anti-apoptosis and invasion of tumour cells. Inhibition of EGFR by EGFR TKIs can reduce D-L1 levels and can reverse the suppression of T-cells by enhancing the production of interferon-γ in EGFR-TKI-sensitive NSCLC. The expression of PD-L1 was highest in EGFR-TKI-resistant cells (EGFR -T790M mutation).
Clinicopathological features associated with high expression of programmed death ligand-1 according to literature review.
Zhang et al. demonstrated that activated EGFR up-regulated the expression of PD-L1 through the interleukin 6 (IL6)/Janus kinase (JAK)/signal transducer and activator of transcription 3 (STAT3) signalling pathway in NSCLC cells (44). EGFR-TKIs treatment reduced the secretion of IL6 from cancer cells and then reduced the activation of JAK/STAT3, thus inhibiting the expression of PD-L1, leading to reduced proliferation and increased apoptosis of NSCLC cells. Okita et al. evaluated the impact of PD-L1 expression and EGFR and human epidermal growth factor receptor 2 (HER2) in tumour cells from pathological stages IA-IIIA NSCLC (45). They showed that PD-L1 overexpression was associated with poor recurrence-free survival (p=0.012) and OS (p<0.001). It was also positively correlated with EGFR expression (p=0.027) and inversely correlated with HER2 expression (p<0.001) in resected NSCLC tissue. Moreover, they suggested that PD-L1 expression might be partially regulated via phosphatidyli-nositol-3-kinase/protein kinase B (PI3K/AKT) and JAK/STAT pathways.
Tang et al. found that high levels of PD-L1 in patients with EGFR-WT were a prognostic factor of poor OS (p=0.029). In EGFR-WT NSCLC, cancer cells can evade host immune responses by expressing PD-L1 to down-regulate cytotoxic T-lymphocyte activation in the tumour microenvironment, allowing cancer cells to survive (46). Gainor et al. showed the lack of concurrent PD-L1 expression with high levels of CD8+ TILs in EGFR-mutant patients, suggesting an innate resistance to the activity of PD-1/PD-L1 inhibitors (47).
Akbay et al. demonstrated that activation of the EGFR pathway induced PD-L1 expression and led to evasion of the host antitumour immune response (43). EGFR-driven tumours may induce an immunosuppressive microenvironment in the lung with an increase of immunosuppressive cytokines, growth factors and chemokines involved in immune cell accumulation. EGFR inhibitors reduced the PD-L1 level in NSCLC cell lines with activated EGFR, confirming the correlation between PD-L1 expression and EGFR signalling (43).
D'Incecco et al. found that PD-L1-positive patients treated with EGFR-TKIs (gefitinib or erlotinib) had higher response rates (61.2% vs. 34.8%, p=0.01) and longer time to progression (11.7 months vs. 5.7 months, p<0.0001), compared to PDL-1 negative individuals. In a subgroup of patients with EGFR-mutated NSCLC, time to progression was significantly longer (29.5 months vs. 21.1 months, p=0.01) in PD-L1-positive than in PD-L1-negative cases (48). Haratani et al. showed that patients without EGFR-T790M mutation but with other EGFR mutations are more likely to benefit from nivolumab after EGFR-TKI treatment (PFS=2.1 vs. 1.3 months, p=0.099), possibly as a result of higher PD-L1 expression than in EGFR-T790M-positive patients (49) (Table II).
Relationship between expression of programmed death ligand-1 (PD-L1l and epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitors (TKIs).
In the CheckMate 057 trial, a subgroup analysis showed that nivolumab did not confer a survival benefit in patients with non-squamous EGFR-mutated tumours when compared with docetaxel therapy (HR=1.08, 95% CI=0.69-2.00) (6). Similar results emerged from KEYNOTE 010 trial: no significant survival advantage was shown in EGFR-mutant NSCLC (HR=0.88, 95% CI=0.45-1.70) treated with pembrolizumab when compared with EGFR-WT (HR=0.66, 95% CI=0.55-0.80) (50).
EGFR TKIs in Combination with Immunotherapy
Based on pre-clinical data that activation of the oncogenic EGFR pathway up-regulates PD-L1 expression, enhancing susceptibility of NSCLC cells to PD-L1 blockade, combining EGFR-TKIs with immunotherapy appears to be a promising therapeutic approach (43). Combination therapy of different EGFR-TKIs with various immune-checkpoint inhibitors is currently under investigation (51). Preliminary results from ongoing phase I/II clinical studies of combination therapies show promising efficacy but high incidence of severe adverse events: nivolumab plus erlotinib (NCT02574078) (52) was associated with 19% of grade 3 toxicities; erlotinib plus atezolizumab (NCT02013219) recorded 39% grade 3/4 adverse events, such as liver enzyme elevation (7%), pyrexia (7%) and rash (7%); the combination of osimertinib plus durvalumab (NCT02143466) (53) was associated with 38% of grade 3/4 interstitial lung disease; and grade 3/4 liver enzyme elevation was reported with the association of gefinitib plus durvalumab (NCT02088112).
EML4–ALK Fusion Gene
ALK rearrangement appears to be associated with higher PD-L1 expression (54-59). Hong et al. found that overexpression of ALK fusion protein increased PD-L1 expression through p-ERK1/2 and p-AKT signalling but not p-JAK3/STAT 3 signalling in NSCLC cells (55). Therefore, EML4–ALK fusion protein represents intrinsic regulation of PD-L1 in NSCLC with EML4–ALK gene fusion. They demonstrated that up-regulation of PD-L1 by EML4–ALK fusion protein induced the apoptosis of T-cells through the PD-L1–PD-1 axis. Inhibiting ALK by sensitive TKIs can reverse the suppression of T-cells and reduce PD-L1 expression. Inferferon-γ was increased in a co-culture of EML4–ALK-positive cells and T-cells after treatment with ALK-TKI crizotinib or LDK378, especially LDK378. They found that PD-1 antibodies were effective in both crizotinib-sensitive and resistant NSCLC cells. No synergistic effect of combining ALK-TKIs and antibodies to PD1 and PD-L1 was observed.
Ota et al. showed that PD-L1 expression was higher in NSCLC cells positive for EML4–ALK rearrangement than in those which were wild-type (p<0.001) (56). ALK tyrosine kinase activity induced by alectinib, a selective inhibitor of ALK, increased the expression of PD-L1 in cells positive for EML4–ALK rearrangement. They found that PD-L1 expression was up-regulated via MEK/ERK and PI3K/AKT signalling in EML4–ALK fusion-positive NSCLC cells, revealing a direct relationship between oncogenic drivers and PD-L1 expression.
KRAS Status
In a recent meta-analysis, Li et al. showed that KRAS-mutant tumours were more likely to be PD-L1-positive than were KRAS-WT tumours (51% vs. 36%; OR=1.69, 95% CI=1.01-2.84, p=0.045) (57).
Chen et al. studied the correlation between KRAS mutation and PD-L1 expression. They demonstrated that KRAS mutation in NSCLC induced up-regulation of PD-L1 by persistent activation of downstream effectors through p-ERK signalling. Moreover, the authors found that up-regulation of PD-L1 by KRAS mutation induced apoptosis of CD3+ T-cells through the PD-1–PD-L1 axis and, consequently, exhaustion of T-cells, which resulted in the immune escape of NSCLC cells (58).
D'Incecco et al. described the relationship of PD-1 positivity with smoking status (p=0.02) and KRAS mutation (p=0.002) in patients with NSCLC (50). Davar et al. described a complete response to nivolumab in a patient with advanced KRAS-mutant pulmonary adenocarcinoma (59). In CheckMate 057, a subgroup analysis showed that nivolumab had a greater survival benefit in patients with KRAS-mutant tumours than WT (52). Rizvi et al. showed that KRAS mutation was most frequent in patients with NSCLC who were smokers, with a durable clinical benefit with pembrolizumab (60).
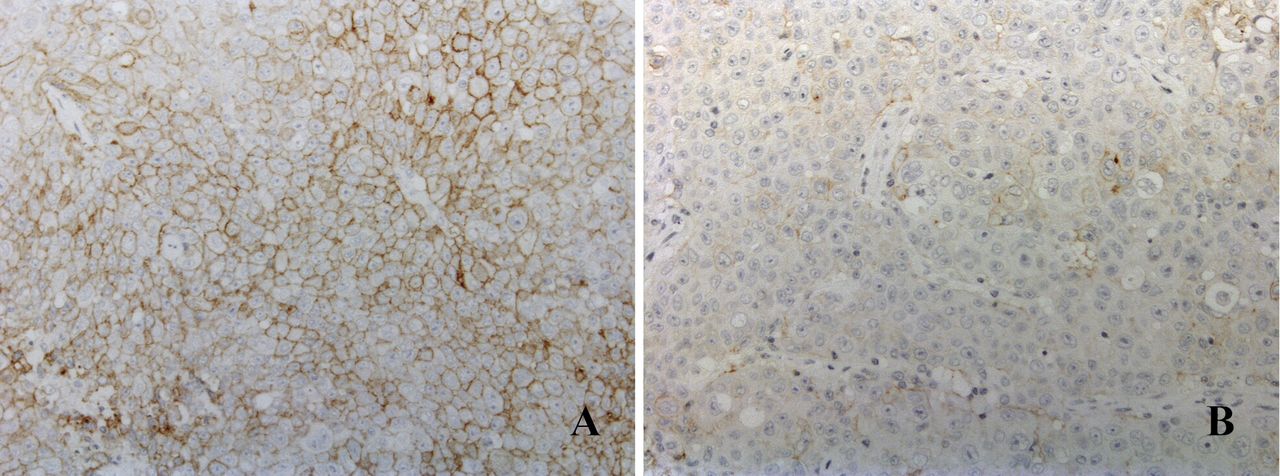
Programmed death ligand-1 (PD-L1) expression in non-small cell lung cancer in regard to suitability for immunotherapy. A: Increased PD-L1 expression in >50% of the tumour cells, with a distinctive pattern of membranous positivity. B: PD-L1 expression in fewer than 2% of the tumour cells, which according to the threshold is considered negative, therefore the patient would not be eligible for immunotherapy.
Other Drivers
Kadara et al. revealed that PD-L1 levels were significantly elevated in TP53-mutant lung adenocarcinoma (p=0.002) and reduced in PIK3CA-mutant tumours (p≤0.001) (61). Choi M et al. found that PIK3CA mutations were associated with reduced expression of tumoural PD-L1 and peritumoural PD-1 (p<0.05) (62).
Conclusion
Immunotherapy with monoclonal antibodies to PD-1, such as nivolumab and pembrolizumab, significantly improved the survival of patients with metastatic NSCLC. The efficacy of these new agents varies across individual patients, hence the importance of and need for research on biomarkers that predict response to treatment (63, 64). IHC staining for PD-L1 has been approved as a companion diagnostic tool by the US Food and Drug Administration for patients with advanced NSCLC for pembrolizumab (64) (Figure 1).
However, several studies showed that the predictive role of tumour PD-L1 expression was limited due to the variation in immunoreaction that such antibodies can show based on clinicopathological parameters such as stage of disease (early resected vs. advanced tumour), prior chemotherapy or targeted therapy (EGFR- or ALK-TKIs), prior radiotherapy, gender, mutation status of NSCLC (EGFR, ALK, KRAS), tumour differentiation, histology, and the presence of CD8+ TILs.
It is also well-known that intratumoural heterogeneity exists based on polyclonal evolution of the tumour that in some cases can show a strong but patchy expression of the antibody in specific areas and negative staining in others. Such variability can be limited by the use of different or limited diagnostic samples such as cytology or small biopsy or a non-adequate histopathological sampling of large tumoural masses.
The definition of the threshold in terms of the percentage of positively stained cells and the use of different assays or antibodies can also affect the determination of PD-L1 expression in cancer. Therefore, IHC using anti-PD-L1 may not represent the true PD-L1 status of the tumour but might represent only its expression under specific conditions and IHC staining may increase considerably at later time points in the disease course.
PD-L1 expression appears to be associated with EGFR mutation and EML4–ALK fusion protein in NSCLC (43-59). Pre-clinical models showed that these oncogenic alterations can promote an immunosuppressive tumour microenvironment, mediating immune escape of NSCLC. Thus, antibodies to PD-1/PD-L1 may represent an optional therapy in these settings (65). Currently, the role of combination therapy of EGFR-TKIs and immunotherapy is under investigation. In consideration of tumour heterogeneity and the variability of PD-L1 expression, re-biopsy and the re-evaluation of this biomarker after conventional treatments should be considered in patients that were not previously eligible for immunotherapy. Further prospective trials are necessary to evaluate this therapeutic approach.
Footnotes
This article is freely accessible online.
- Received March 11, 2018.
- Revision received May 19, 2018.
- Accepted May 23, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Longitudinal analysis of PD-L1 expression in patients with relapsed NSCLC
- Serious Immune-related Adverse Events Are Associated With Greater Efficacy of Nivolumab Therapy Against Non-small Cell Lung Cancer
- Predictive biomarkers for PD-1/PD-L1 checkpoint inhibitor response in NSCLC: an analysis of clinical trial and real-world data
- A Machine Learning Approach Using PET/CT-based Radiomics for Prediction of PD-L1 Expression in Non-small Cell Lung Cancer
- DNA Polymerase Delta 1 Catalytic Subunit (POLD1) as a Prognostic Factor in Clear Cell Renal Cell Carcinoma Patients
- Prognostic Implication of PD-L1 Expression on Osimertinib Treatment for EGFR-mutated Non-small Cell Lung Cancer
- Transcriptomic Characterization Reveals Blood-based Molecular Signatures of NSCLC Patients in Response to Anti-PD-1 Therapy Combined with Chemotherapy
- PD-L1 Expression Status Predicting Survival in Pulmonary Pleomorphic Carcinoma
- Real-world programmed death-ligand 1 prevalence rates in non-small cell lung cancer: correlation with clinicopathological features and tumour mutation status
- Combining biopsy tools improves mutation detection rate in central lung cancer
- Identification of PD1-mediated regulation of antitumor antigen response in patients with NSCLC using the trans vivo DTH assay
- Clinicopathological and Prognostic Significance of Programmed Death Ligand 1 Expression in Korean Patients With Triple-negative Breast Carcinoma