


Abstract
Background/Aim: The sacrifice of a major hepatic vein can cause hepatic venous congestion (HVC). We evaluated the effects of HVC on regional liver function using the liver uptake value (LUV), that was calculated from 99mTc-labeled-galactosyl-human-serum-albumin (99mTc-GSA) single-photon emission computed tomography (SPECT) /contrast-enhanced computed tomography (CE-CT) fused images. Patients and Methods: Sixty-two patients underwent 99mTc-GSA SPECT/CE-CT prior to hepatectomy for liver cancer and at 7 days after surgery were divided into groups with (n=8) and without HVC (n=54). In the HVC group, CT volume (CTv) and LUV were separately calculated in both congested and non-congested areas. Results: The remnant LUV/CTv of the HVC group was significantly smaller than that of the non-HVC group (p<0.01). The mean functional ratio was 0.47±0.05, and all ratios were ≥0.39. Conclusion: After hepatectomy with sacrifice of major hepatic vein, liver function per unit volume in the congested areas was approximately 40% of that in the non-congested areas.
- Hepatic venous congestion
- 99mTc-labeled-galactosyl-human-serum-albumin SPECT/CE-CT fused image
- liver uptake value
- hepatic function
- liver failure
Hepatic venous congestion (HVC) often seems to be related to extended right and left hepatectomy when sacrificing the middle hepatic vein and venous congestion has been observed in the left medial or right anterior sector of the remnant liver, respectively (1, 2). Contrast-enhanced computed tomography (CE-CT) imaging is clinically useful in the diagnosis of postoperative HVC (3). The negative impact of HVC has been reported in morphological regeneration after hepatectomy (1, 4-6). However, the liver volume cannot directly represent hepatic functional change itself (7, 8). Thus, the liver volume measured from CT (CTv) alone is not completely adequate for assessing the overall effects of HVC on hepatic functional recovery after hepatectomy.
99mTc-Labeled galactosyl human serum albumin (99mTc-GSA) scintigraphy has been used for the quantitative assessment of preoperative liver functional volume for patients with liver cancer (9-12). Moreover, the indices obtained by 99mTc-GSA single-photon emission computed tomography (SPECT) have been proven useful in evaluating the hepatic function during the regeneration process (9). Quantitative indices of liver uptake value (LUV) obtained by the combination of 99mTc GSA SPECT and CT images have yielded an accurate estimation of the hepatic function and histopathological damage in patients with chronic liver disease (13). We crafted a 99mTc-GSA SPECT and CE-CT fused imaging technique using SPECT and a multi-detector row CT integrated system, which is now commercially available (8, 14, 15). The registration between 99mTc-GSA SPECT and CE-CT images is considered to be satisfactory, and able to estimate the remnant liver function and the congested area precisely based on the LUV.
In HVC, remnant hepatocytes are regarded as compensating for the functional loss during the initial stages after hepatectomy (16-18). However, little is known regarding the exact nature of the effects of HVC on the regional and remnant hepatic functions. The aim of the present study was to clarify the impact of HVC on regional and remnant hepatic functions using the 99mTc-GSA SPECT/CE-CT fused imaging technique.
Patients and Methods
Between January 2011 and December 2014, 333 patients underwent 99mTc-GSA SPECT/CE-CT examinations for the perioperative evaluation of hepatectomy, mainly for liver cancer. We selected the patients who underwent segmentectomy or more and performed 99mTc-GSA SPECT/CE-CT examinations on them prior to surgery and then again at 7 days after surgery. The presence or absence of a congested area was assessed using the method described below. The primary endpoint was a comparison of liver function per unit volume in the congested and non-congested areas. Secondary endpoints included the influence of HVC on postoperative liver function and the postoperative course. Blinded evaluation of functional scintigraphic and functional CE-CT imaging was performed by separate radiologists/nuclear medicine physicians (M.Y. and S.S.). Based on the hepatic function on postoperative day 7 and the criteria established by the International Study Group of Liver Surgery (19), we determined whether postoperative liver failure actually occurred in these patients. Data were prospectively collected. This study was approved by our Institutional Review Board (approval number: 1383), and informed consent was obtained from all patients.
Liver resection. Liver resection was performed using our previously described techniques (15, 20). A suitable extent of liver resection was selected according to the indocyanine green (ICG) retention rate at 15 min (ICG R15) and functional volumetry by 99mTc-GSA SPECT/CE-CT images (21). If the estimated congested area was extensive, then venous preservation or reconstruction was planned.
Detection of HVC. Hepatic regions drained by hepatic vein tributaries were calculated on the basis of preoperative CE-CT imaging using the Ziostation2 workstation (ZIOSOFT, Tokyo, Japan). In previous studies (3, 4). HVC has been recognized as the attenuation difference area on arterial and hepatic portal phase CT images (Figure 1). We confirmed that the hepatic attenuation difference area calculated from postoperative CE-CT imaging obtained on postoperative day 7 was the same as the hepatic vein tributaries calculated from preoperative CE-CT imaging on the workstation. Patients were divided into two groups: the group with congestion who had definite postoperative HVC and the non-HVC group who did not have postoperative HVC.
CT volumetry. The region of interest was manually set for the whole liver on each image of every slice; regions without any tumors were included (8, 20). We measured the whole liver and simulated remnant CTv from preoperative CE-CT images and the remnant CTv from postoperative CE-CT images. Moreover, in the HVC group, the simulated remnant volumes of the congested and non-congested areas were also measured on the basis of the surgical procedure and hepatic portal/venous tributaries from preoperative CE-CT imaging.
Functional volumetry by 99mTc-GSA scintigraphic imaging. A SPECT/CT system was used for scintigraphy and CT imaging, respectively (22). 99mTc-GSA (185 MBq) was injected as a bolus
into an antecubital vein. The image parameter of SPECT image is summarized in Table I. The attenuation-corrected SPECT and CT images were analyzed using a dedicated workstation (Ziostation2; ZIOSOFT, Tokyo, Japan). Whole-liver and simulated remnant LUVs were calculated from the preoperative 99mTc-GSA SPECT/CE-CT images, and the remnant LUV was obtained from the postoperative 99mTc-GSA SPECT/CE-CT images (8). Moreover, in the HVC group, we calculated the simulated LUV of the congested and non-congested areas on the basis of the surgical procedure and hepatic portal/venous tributaries from preoperative CE-CT imaging. According to the attenuation difference on postoperative CE-CT images, we separately measured the LUV of these areas. To evaluate apparent effects of HVC on regional function, the LUV/CTv was calculated using pre-and postoperative 99mTc-GSA SPECT/CE-CT images. Furthermore, in the HVC group, the LUV/CTv of the congested and non-congested areas were independently measured. Finally, we calculated the functional ratio between the congested and non-congested areas using the following formula:

Image parameters of hepatic single-photon emission computed tomography (SPECT) imaging.
Statistical analysis. Values are expressed as mean±standard deviation (range). To examine variations in the parameters within any two groups, a two-way analysis of variance in multiple comparisons was used. Values between any two groups were compared using the Mann–Whitney U-test, and correlations were analyzed using the Pearson test. Statistical analysis was performed using the JMP statistical software package (version 11; SAS, Cary, NC, USA). p-Values of less than 0.05 were considered statistically significant.
Results
Initially, out of the 333 patients, 65 who underwent segmentectomy or more were selected. A total of 11 patients were diagnosed as having impaired blood flow; however, three patients were excluded because they had accidental congestion in the remnant liver. They experienced partial outflow block with or without inflow block. Finally, 62 patients were divided into two separate groups: an HVC group comprising eight patients in whom the trunk of the main hepatic vein had been sacrificed and the non-HVC group comprising 54 patients without transection of the main hepatic vein trunk. A typical case with HVC is shown in Figure 1. The perioperative clinical characteristics of patients are summarized in Table II. In the HVC group, six out of the eight patients had hepatocellular carcinoma (HCC), one had intrahepatic cholangiocarcinoma, and one had a large hemangioma. In the non-HVC group, 41 out of the 54 patients had HCC, seven had liver metastasis, five had intrahepatic cholangiocarcinoma, and one had a large hemangioma. Segmentectomy, monosectionectomy, and disectionectomy or more were performed on two, none, and six patients in the HVC group and two, 26, and 26 patients in the non-HVC group, respectively. There were no statistical differences in the preoperative hepatic functional tests, hepatic fibrosis, and surgical insult between the two groups.
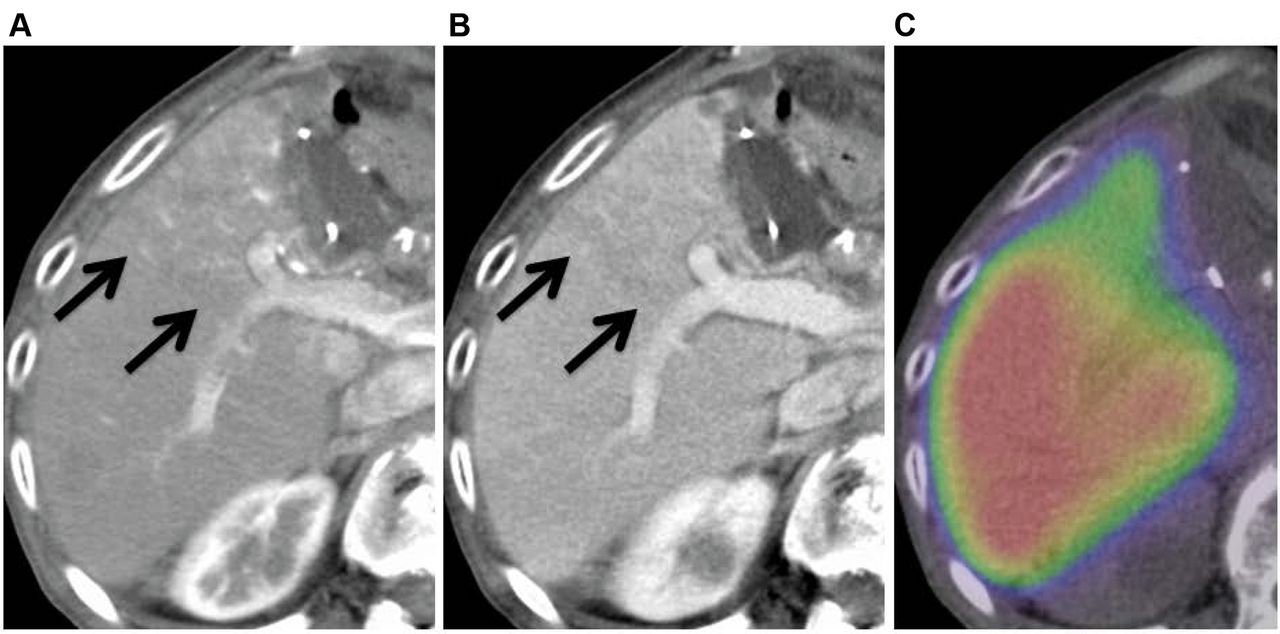
Patient 1 underwent extended left hepatectomy (S5). In the arterial (a) and portal (b) phases, venous congestion is seen in the anterior section. On 99mTc-labeled-galactosyl-human-serum-albumin (99mTc-GSA) single-photon emission computed tomography (SPECT)/contrast-enhanced computed tomography (CE-CT) fused imaging (c), radioactivity was lower in the congested area than that in the non-congested area.
Effects of HVC on regional hepatic functional volume. In the HVC group, the simulated CTv of the congested and non-congested areas before hepatectomy was 172.1±70.7 cc and 711.6±210.2 cc, respectively, and 124.9±60.7 cc and 837.1±231.4 cc, respectively, after hepatectomy. Before hepatectomy, the LUV/CTv of the HVC and non-HVC groups was 0.043±0.017%/m2/cc and 0.043±0.012%/m2/cc, respectively, but the differences were not significant (p=0.96).
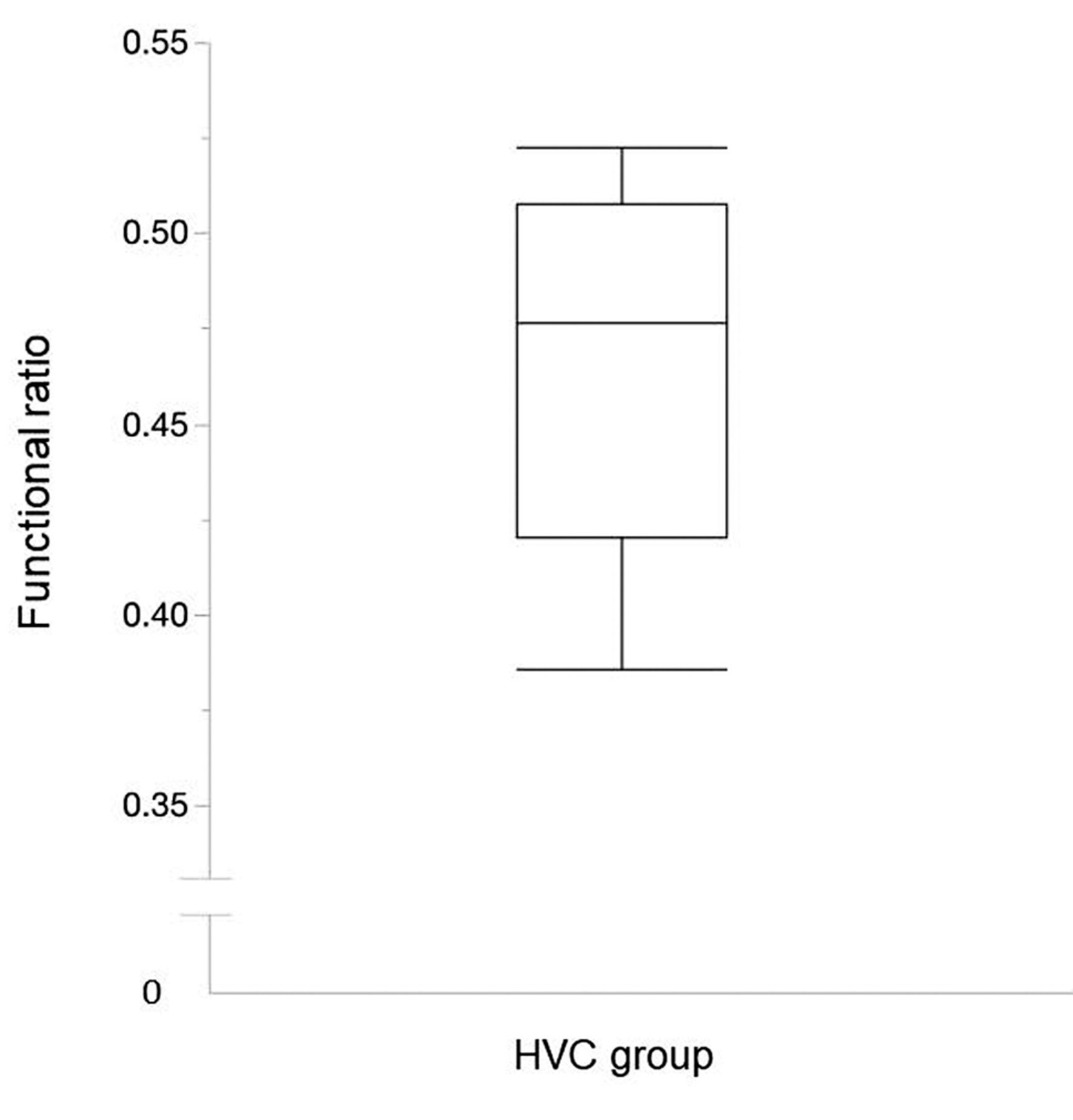
After hepatectomy, the remnant LUV/CTv of the non-HVC group was 0.052±0.018%/m2/cc. In the HVC group, LUV/CTv of the congested and non-congested areas was 0.029±0.008%/m2/cc and 0.050±0.019%/m2/cc, respectively (Figure 2). There were no significant differences between the remnant LUV/CTv of the non-HVC group and that of non-congested areas in the HVC group (p=0.96). In contrast, the remnant LUV/CTv of the congested areas was significantly smaller than that of the non-HVC group (p<0.01). The remnant LUV/CTv of the congested areas was smaller than that of the non-congested areas, but the difference was not significant (p=0.07). The functional ratio was 0.47±0.05, and all of the recorded data were ≥0.39 (Figure 3).
Postoperative liver failure. There were no surgery-related deaths within the 3 months after the surgery. According to the criteria (24), on postoperative day 7, 16 out of the 62 patients experienced postoperative liver failure, including three (38%) out of the eight patients and 13 (24%) out of the 54 patients in the HVC and non-HVC groups, respectively. In the HVC group, one patient had grade A, one had grade B, and one had grade C postoperative liver failure. In the non-HVC group, nine patients had grade A, three had grade B, and one had grade C postoperative liver failure. The frequency of all grade liver failure was similar in both groups (p=0.22), whereas that of grades B and C was higher in the HVC group than in the non-HVC group, but the difference was not significant (p=0.24).

Liver uptake value (LUV)/liver volume measured from CT (CTv) of the groups with and without hepatic venous congestion (HVC) on postoperative day 7. No significant differences were observed between the remnant LUV/CTv of the non-HVC group (0.052±0.018%/m2/cc) and that of non-congested areas (0.050±0.019%/m2/cc) in the HVC group (p=0.96). On the other hand, the remnant LUV/CTv of the congested areas (0.029±0.008%/m2/cc) in HVC was significantly smaller than that of the non-HVC group (p<0.01) and was also smaller than that of the non-congested areas in HVC, but the difference was not significant (p=0.07).
Discussion
In the present study, we focused on patients with planned HVC and estimated the liver function of the congested area was approximately 40% that of the non-congested area. Although the function of the congested area can be calculated using the 99mTc-GSA SPECT/CE-CT system, currently this system is not widely used. In contrast, in patients with planned HVC, future congestion volume is easily simulated before surgery as a perfusion area of the sacrificed hepatic vein from preoperative CE-CT imaging in the dedicated workstation. Considering that the functional ratio of the congested area was approximately 40% or more, it is immediately possible to calculate the limit of safe liver resection volume. If the liver function of the congested area is calculated as 0%, then the remnant liver function can be estimated to be smaller than actual liver function.
In congested areas, the venous blood was regurgitated to the portal vein through the sinusoid and portal blood supply was reduced (3, 25). In a completely congested area, the blood can flow into the hepatic artery and out of the portal vein, instead of the hepatic vein (25). Decreased GSA uptake in the congested area is caused by a decrease in the portal blood supply. The degree of HVC might be related to that of hepatic dysfunction at the very early postoperative stages. Moreover, the congested area can develop venous collaterals into the remnant hepatic venous system during the course of postoperative regeneration (25). In this study, the functional ratio was distributed within a narrow range of 0.39-0.52.

Distribution of functional ratios in the group with hepatic venous congestion (HVC) (n=8). The bottom and top of the box show the first and third quartiles, and the band inside the box is the median. The median of the functional ratio was 0.47. The end whiskers show the lowest and highest points of the entire spectrum (0.39-0.52).
On intra-operative ICG fluorescence imaging, Kawaguchi et al. found the hepatic function in the congested areas in HVC was reduced to 40% compared with that in the non-congested areas (26). This imaging modality can evaluate the liver function of the congested area in HVC immediately after hepatic vein occlusion. Surprisingly, their functional ratio of 40% for the congested area was identical to that of our study. ICG fluorescence imaging was difficult to perform before hepatectomy and was captured only on the liver surface in their study, whereas 99mTc-GSA SPECT/CE-CT can be performed before hepatectomy and can evaluate the entire liver. We recommend that these two methods be used in a complementary manner. In contrast, upon using gadolinium-ethoxybenzyl-diethylenetriamine penta-acetate magnetic resonance imaging (EOB-MRI), the hepatic function in the congested segment was reduced to 70% compared with that in the non-congested segment (27). In that study, the liver to muscle ratio was compared between non-congested area and whole HVC segment. The HVC segment included both congested and non-congested areas: therefore, the hepatic function was estimated to be better than actual liver function. Although EOB-MRI was useful for detecting the tumor, a functional assessment for preoperative simulation was not completely established (27, 28). By evaluating the clinical course, several reports have confirmed that 99mTc-GSA SPECT/CT is useful for preoperative functional simulation and assessment of postoperative functional liver regeneration (8, 11, 15).
Clinical characteristics of all patients (n=62).
Hepatic functional indices of the group with hepatic venous congestion before hepatectomy.
In the HVC group, there was a relatively higher incidence of postoperative liver failure; therefore, HVC might be a factor responsible for this medical complication. Not much attention has been paid to the role of HVC at the time of preoperative decision making regarding liver resection. In this study period, we made minor changes to the extent of liver resection intraoperatively. Considering the relationship between HVC and portal blood supply, the effect of HVC on regional hepatic function might not be mild. Impaired portal blood supply substantially reduces regional hepatic function (7). The subsequent lack of portal blood supply impairs early postoperative liver function and regeneration of the liver remnant (4-6). In this study, three patients experienced liver failure. Considering the latent risks involved in hepatectomy, we recommend venous reconstruction or portal vein embolization in patients with an insufficient functional reserve (29, 30). In patients with noninvasive HCC, the preservation of the hepatic vein is also possible.
There exist some limitations to the present study. Firstly, this was a retrospective study performed at a single academic center. The population included a small number of patients with HVC. Therefore, the results obtained need further confirmation by large multicenter studies. Secondly, the degree of HVC varied among cases on postoperative day 7 because of the degree of the formation of intrahepatic collaterals between obstructive and non-obstructive veins. Thirdly, we did not evaluate the relationship between HVC and other risk factors of postoperative liver failure, such as preoperative chemotherapy, blood transfusion, postoperative complications, and postoperative external biliary drainage (31, 32). These may be related to both hepatic functional recovery and postoperative liver failure.
We conclude that hepatic function per unit volume in the congested areas was approximately 40% of that in the non-congested areas. For preoperative simulation, a more accurate estimation of the future remnant liver volume may be obtained by calculating the sum of the volume of the congested area multiplied by 0.4 and the volume of the non-congested area.
Acknowledgements
The Authors declare that they have no conflict of interest in regard to this study.
- Received February 22, 2018.
- Revision received March 15, 2018.
- Accepted March 20, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.