


Abstract
Background/Aim: This study gives an insight into recent trends for Human papillomavirus (HPV)-specific infection and its fluctuation over the years 2011-2016. Materials and Methods: A total of 2,417 Caucasian women between the age of 18 and 71 years underwent their annual gynaecologic examination at the Outpatient Gynaecological Clinic in the study period. Results: Overall HPV prevalence was 43.9%, and high-risk HPV accounted for 31.3%. HPV16 was the most common high-risk type followed by HPV51 and HPV31. HPV positivity was higher in those with low- and high-grade squamous intraepithelial lesions (HSILs) than in women with a normal cytological test. HPV infection was highest in 2011.The prevalence of single infections remained higher than multiple infections over the entire study period. HPV16 prevalence was very high in the first years of the study and HPV18 exhibited highest prevalence in 2011. Younger women exhibited a significant increase in HPV infection from 2014. Overall HPV infection decreased over the study period. Conclusion: These data suggest that HPV vaccination might reduce the frequency of HSILs and cervical cancer and are useful for the development of a national screening programme.
Human papillomavirus (HPV) infection is the most common sexually transmitted disease and infection with oncogenic types has been well established as the leading cause of cervical cancer. In Greece, 421 new cervical cancer cases are diagnosed annually, making cervical cancer the second most common female malignancy among women aged 15 to 44 years (1).
Papillomaviruses evolved together with their hosts (2). Over 100 types of HPV can infect the anogenital epithelium, but only 13 types, designated as oncogenic can progress to severe lesions (3). Most infections are encountered by the immune system and regress spontaneously without even being clinically detected. However, viral proteins act to modulate innate immune response to establish persistent infections (4) that if left untreated can lead to cervical intraepithelial lesions and cervical cancer.
The long time interval between infection and cancer has made cervical cancer screening rather effective (5). Pap test screening has led to the decrease of cervical cancer (6) and co-testing with HPV DNA test has been used in many developed countries. However, debate is continuing on whether HPV DNA test will replace cytology in primary screening as it is more sensitive than cytology for high-grade cervical intraepithelial neoplasia (CIN), but less specific (7).
Although the prevalence and distribution of individual HPV types might vary in different geographic regions worldwide, specific guidelines have only been established in certain countries. HPV types are also distributed differently among distinct grades of intraepithelial lesions, depending on their ability to cause transformation in cervical cells (8, 9).
Genotyping provides information in HPV-type specific infections. It is necessary to monitor HPV infection and type distribution in a population in order to assess the measures that need to be taken for eliminating cervical cancer (10, 11). Relatively few studies have been conducted to investigate specific HPV type infections in Greek women (12-17).
HPV16 and HPV18 are the most common oncogenic types associated with cancer (9, 18). Recently a 9-valent vaccine including virus-like particles of HPV types 6, 11, 16, 18, 31, 33, 45, 52 and 58 has been introduced. It has been assessed that on a worldwide scale, the 9-valent vaccine could potentially prevent approximately 90% of HPV-related cancers of the cervix, vulva, vagina and anus (18-22). Obtaining data before applying vaccination is crucial in order to evaluate effectiveness of this vaccine in preventing neoplastic lesions associated with the above genotypes (23). It is also interesting to monitor the distribution of HPV types after vaccination, which in Greece began in 2007.
This study gives an insight into recent trends in specific HPV infection and its fluctuation in different age groups and cytological abnormalities.
Materials and Methods
This prospective study consisted of consecutive samples from 2,417 Caucasian women who attended the Outpatient Gynaecological Clinic of St. Savvas Regional Anticancer Oncology Hospital of Athens between May 2011 and November 2016, in order to have their annual gynaecological examination. The patients were also offered HPV test with the knowledge that it was not part of the screening. Women were eligible if they were not pregnant and had no history of HPV-related cervical disease and they were screened only once in the current study. Ethical approval was granted by the Ethics Committee of St. Savvas Regional Anticancer Oncology Hospital of Athens (approval number: 6937/448).
Cervical cell scrapings were collected by a gynaecologist with a cytobrush (Rovers Cervex; Brush Combi Rovers Medical Devices B.V, Oss, the Netherlands) from the ecto- and endo-cervix of the uterus. A slide was prepared for conventional cytology and the cytobrush was then placed in specimen transport medium (Thin-Prep PreservCyt Solution; Hologic, Inc. Ltd., Manchester, UK) and stored at 4°C until prepared for HPV molecular analysis. Cytological findings were classified in line with the 2001 Bethesda classification system (24).
Five millilitres of Thin Prep samples were used for DNA isolation. They were centrifuged, diluted in lysis buffer (NucliSENS lysis buffer; bioMérieux Hellas S.A, Athens, Greece) and finally subjected to the NucliSENS easyMAG platform (bioMérieux Hellas S.A, Athens, Greece) for automated extraction, according to the manufacturer's instructions. Nucleic acids were eluted in 55 μl of elution buffer. DNA quality test was carried out using Human Globin, Beta, Primer set kit (Maxim Biotech, Inc., South San Francisco, CA, USA) according to the manufacturer's instructions. Aliquots were stored appropriately for further processing. PapilloCheck HPV-Screening (Greiner Bio-OneGmbH, Frickenhausen, Germany) was used. This technology is based on a DNA chip for the type-specific identification of 24 HPV types (high-risk: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 73, 82, probable high-risk 53 and 66 and low-risk: 6, 11, 40, 42, 43, 44/55, 70) (5). E1-based polymerase chain reaction (PCR) was performed according to the manufacturer's guidelines. For each sample, 19.8 μl PapilloCheck MasterMix, 0.2 μl HotStarTaq plus DNA polymerase (5U/μl, Qiagen, Hilden, Germany) and 5 μl DNA from the cervical sample were mixed. Hybridization followed by mixing 30 μl of the PapilloCheck Hybridization buffer in a fresh reaction tube with 5 μl of the polymerase chain reaction product at room temperature and transferring 25 μl of the hybridization mix into each compartment of the chip. Positive and negative controls were used in each chip. The chip was incubated for 15 min at 25°C in a humid atmosphere and then washed in three buffer solutions, centrifuged and scanned on the CheckScanner™.
Data were stratified by year, age group and cytology and analysed using SPSS 20 (IBM, Armonk, NY, USA). The prevalence of HPV infection was calculated and expressed as a percentage together with the 95% confidence interval. Two-by-two contingency tables and Fisher's exact test were used to assess statistical significance of any differences in prevalence. Changes in HPV prevalence over time and by age group were assessed by Chi-squared trend test. p-Values of less than 0.05 were considered statistically significant.
Results
The age of 2,417 women ranged from 18-71 years (mean=32.6 years). Women were divided into three age groups (18-25, 26-46 and 47-71 years) in accordance with the biological alterations in the female reproductive system. All samples included in the study were positive for human beta globin. Women with normal cytology represented 54.6% of the total population, atypical squamous cells of undetermined significance (ASCUS) were found in 4.6%, low-grade squamous intraepithelial lesions (LSILs) were found in a large proportion of women (37.4%) and high-grade squamous intraepithelial lesions (HSILs) were detected in 3.4%. Only three women had cervical cancer, including two cases of adenocarcinoma and one case of squamous cell carcinoma (0.1%).
Overall HPV prevalence was 43.9% (95% CI=41.9-45.9%) and high-risk HPV types accounted for 31.3% (95% CI=29.4-33.1%). Overall, HPV16 was the most common high-risk HPV type followed by HPV51 and HPV31. HPV42 was the most frequent low-risk HPV type (Figure 1).
Regarding cytology, HPV16 was highly prevalent in HSILs (43.9%, 95% CI=33.2-54.6%), ranking first in both ASCUS (15.4%, 95% CI=8.7-22.2%) and LSILs (16.9%, 95% CI=14.5-19.4%). HPV31 also ranked high in HSILs, with prevalence of 18.3% (95% CI=9.9-26.7%). All three patients with cancer harboured HPV18. Two of the cancer cases presented co-infection with HPV6. HPV6 appeared in 6% (95% CI=4.4-7.5%) of the women with LSIL (data not shown). As expected, HPV positivity was higher in those with LSIL and HSIL than in women with a normal cytological test (p<0.001).
Figure 2 illustrates the trend in HPV prevalence from 2011 to 2016 when taking into consideration all study women. HPV infection was highest at 48.1% in 2011, remaining at a rather stable level until 2013, followed by a notable decrease to 36.7% in 2014 (p=0.043). After 2014, the level was relatively stable, with non-significant changes in 2015 and 2016 (p=0.463 and p=0.508, respectively).
Single and multiple HPV infections were found in 26.1% (95% CI=24.4-27.9%) and 17.9% (95% CI=16.3-19.4%) of the samples, respectively, and single infections remained higher than multiple infections over the entire study period (Figure 3). Multiple infections presented a decreasing trend until 2014, then showing a very moderate gradually increasing trend, until 2016. Single infections tended to increase from 2011 to 2013, then declined in the period 2013-2016.
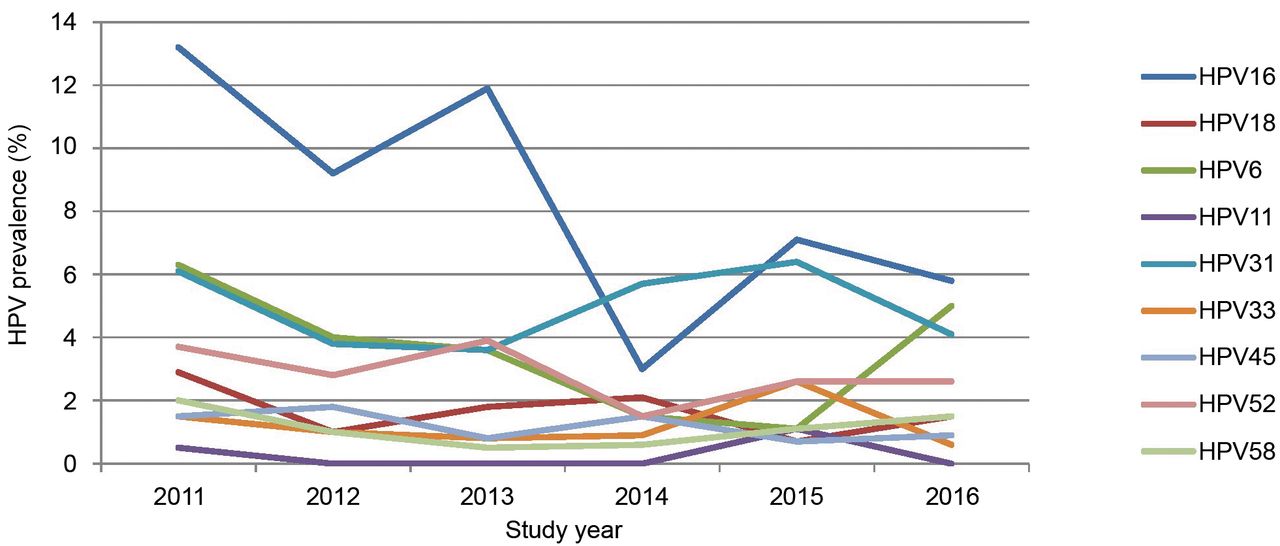
HPV16 presented very high prevalence in the first years of the study. The lowest prevalence was noted in 2014. HPV18 exhibited highest prevalence in 2011 (2.9%) decreasing to 0.7% in 2015 and staying relatively low although doubling in 2016. HPV31 prevalence increased after 2013 reaching the rate of HPV16, which ranked first. The prevalence of HPV45 remained relatively constant at lower rates. HPV6 tended to decrease in frequency except for 2016, in contrast to HPV11, which remained at a very low percentage (0-1.1%) (Figure 4).

Human papillomavirus (HPV) type distribution in the total study population.

Human papillomavirus (HPV) infection across the study years: prevalence ±95% confidence interval.
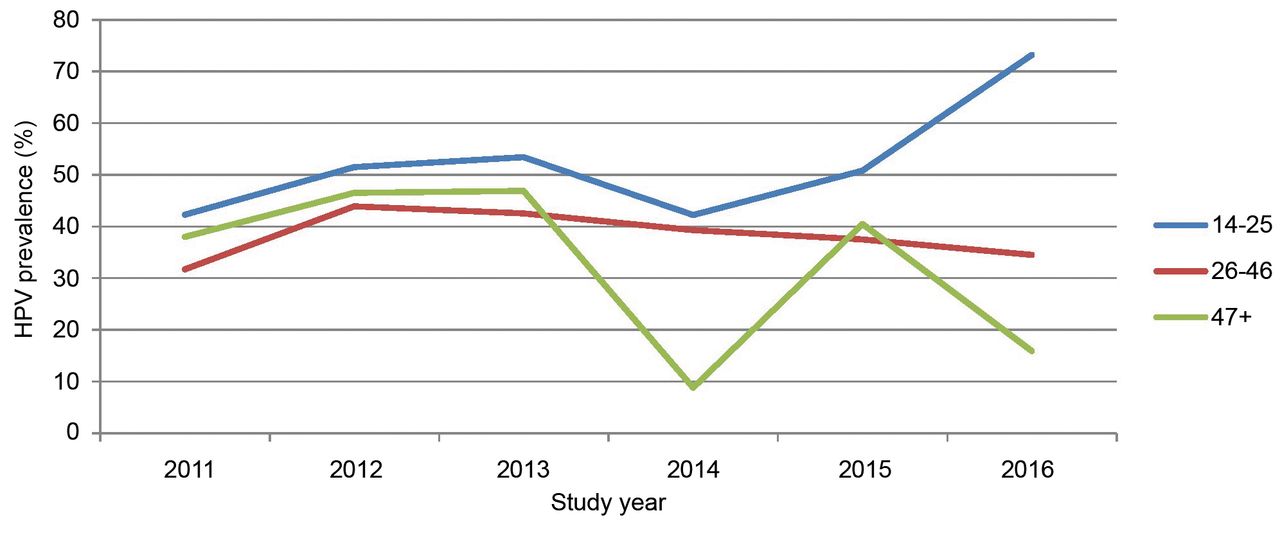
HPV infection varied greatly among the age groups over the study period. Younger women exhibited a significant increase in HPV infection from 2014 (p=0.004) reaching a peak of 73.2% in 2016. Women aged 26-46 years presented a stable prevalence, unlike older women, who had two peaks in HPV infection in 2013 and 2015 (Figure 5).
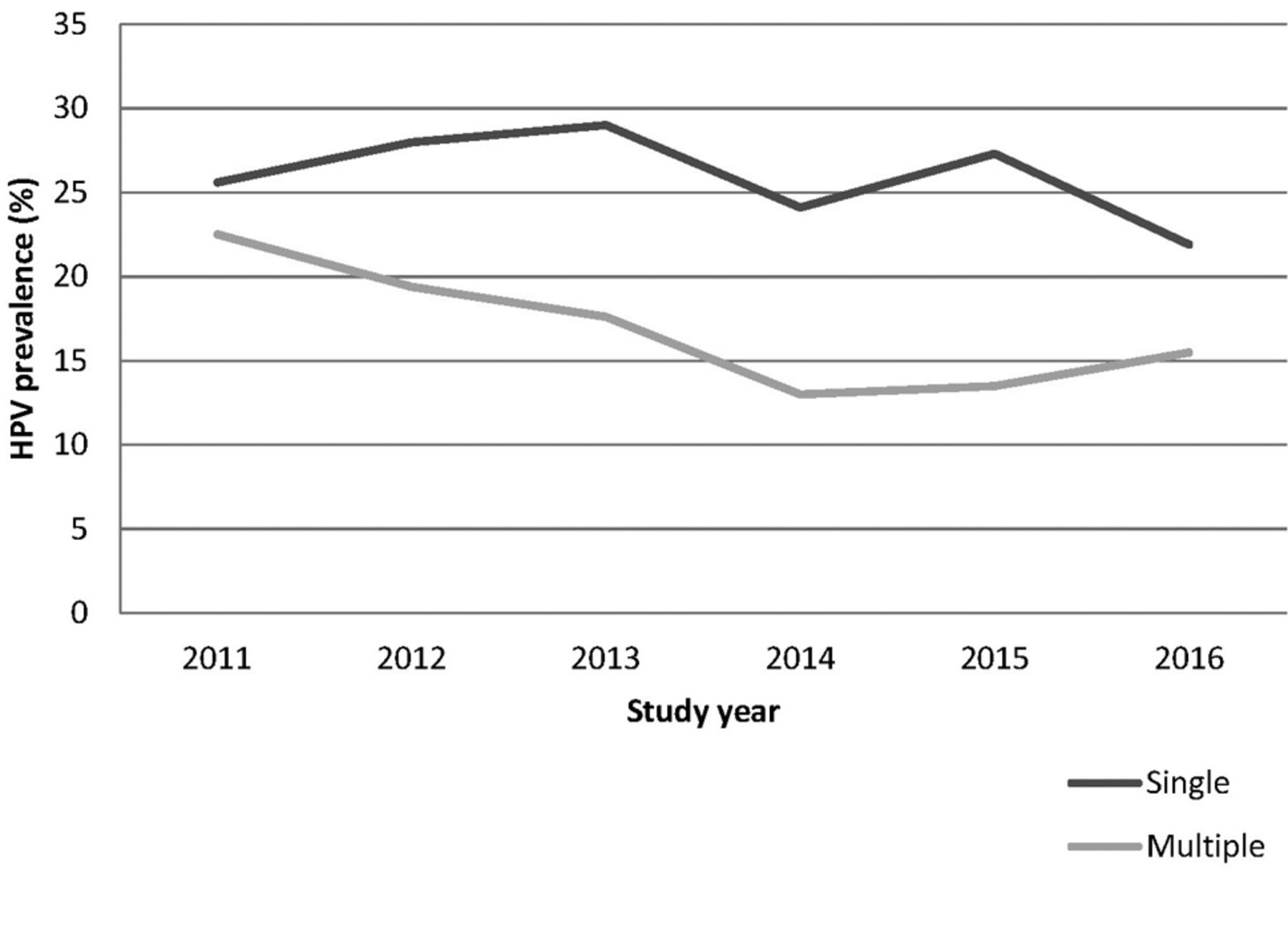
Single and multiple Human papillomavirus (HPV) infection across the study years.
Overall, HPV16 and 31 ranked high in the first two age groups and HPV6 prevalence was rather increased in younger women at 5.8% compared with 1.1% in older women (data not shown).
Discussion
We present here a relatively large study of HPV prevalence in opportunistic hospital screening across years. In this study population, HPV infection rates decreased over the study years. The decrease of HPV infection after 2013 may reflect an increase in vaccination uptake or may be attributed in changes in social and behavioural variables. Vaccination in Greece commenced in 2007; at first it was met with suspicion as teenagers and their parents did not receive adequate information. Although the vaccination status of the studied population was unknown, it is possible that women aged more than 26 years did not receive vaccination since it was not approved for this population.

Human papillomavirus (HPV) type distribution across the study years.

Human papillomavirus (HPV) infection across the study years according to age group.
The current study showed that the most prevalent genotype was HPV16, similarly to the findings of previous studies conducted in Greece (15-17). In addition, HPV31 and HPV6 exhibited rather high rates. An interesting finding was that HPV16 decreased over the study years, while HPV31 increased after 2013. This might be attributed to an overall impact of vaccination. A recent analysis did not observe type-replacement among HPV-vaccinated women in populations with a low vaccine coverage (25). On the contrary, changes in the distribution of HPV types have been observed in a meta-analysis regarding HPV52 and HPV58 (26). This can be explained by the introduction of new HPV types from other geographical areas or by redistribution of the existing types due to behavioural or social changes.
Overall, in this study, the rate of HPV infection decreased with time in the 26- to 46-year-old group, while for younger women it increased significantly after 2014. This increase may reflect behavioural factors such as the increasing concern among younger women regarding HPV infection and their greater willingness to have an HPV DNA test. In the last two years of the study, young women did not miss their annual appointment and were better informed regarding HPV infection. A large-scale study was performed in Greece to describe the prevalence and age distribution of different HPV types among women presenting for a Pap smear in an outpatient clinic in Greece. HPV positivity, high-risk HPV and multiple HPV infections were found to be higher in young women, while HPV prevalence declined with increasing age and presented two peaks a higher (age 14–19 years) and a lower one (age 30–34 years) (16).
The rate for older women decreased over time, except for 2015, where a peak in HPV prevalence was noted. This peak might, however, be due to a natural fluctuation when examining a limited number of patients. Younger women had higher prevalence of HPV infection over time, as seen in other studies (28, 29). This finding possibly reflects physical factors such as younger women having a more naïve immune system and changes in the transformation zone, or behavioural, that is different patterns in sexual activity. In contrast, in a large US population studied to examine HPV prevalence trends from 2004 to 2011, HPV infection rates decreased over time for both age groups (21-30 and 31-64 years) (30).
A study to determine time trends in the prevalence of HPV infection in a Chinese population, from 2011-2015, found a rather constant rate over time. However, infection rates exhibited an upward trend in two young age groups (15-24 and 24-34 years) over those years (31).
The knowledge of the contribution of each HPV type to precancerous lesions is useful for the development of risk-stratified screening algorithms. The data presented here suggest that an effective vaccination programme with the 9-valent HPV vaccine, along with a population-based screening programme, might almost eliminate cervical cancer in women and reduce the frequency of HSILs.
Acknowledgements
This project was supported by St. Savvas, Regional Anticancer Oncology Hospital of Athens, Athens, Greece.
Footnotes
Conflicts of Interests
The Authors declare that there are no competing interests in regard to this study.
- Received February 26, 2018.
- Revision received March 28, 2018.
- Accepted April 2, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prevalence and Determinants of Vaginal Infection With Human Papillomavirus Among Female University Students in Vietnam
- Comparison of HPV Testing and Colposcopy in Detecting Cervical Dysplasia in Patients With Cytological Abnormalities
- Cervical Pathology Following HPV Vaccination in Greece: A 10-year HeCPA Observational Cohort Study