


Abstract
Background/Aim: This study analyzed moesin immunoexpression in 91 lip squamous cell carcinomas and its influence in patients' prognosis. Materials and Methods: Moesin immunoexpression was evaluated at the invasive tumor front by a semi-quantitative score method. The association of moesin with the clinicopathological variables was analyzed by the Chi-square test, the survival rates were calculated by Kaplan–Meier and the survival curves compared using the log-rank test. Results: The expression of moesin was strong at the invasive tumor front and weak/negative in differentiated cells such as keratin pearls. There was no association between moesin expression and the clinicopathological variables, but there was a tendency for patients with lip cancer and strong moesin expression to have lower 5- and 10-year overall and disease-free survival rates. Conclusion: Our results confirm the participation of moesin in oral carcinogenesis and suggest that this protein can influence the survival rates of patients with lip squamous cell carcinoma.
Moesin is a member of the ERM (ezrin, radixin and moesin) family that is expressed in normal and neoplastic oral mucosa (1-6). This protein has been found predominantly at the membrane of basal and parabasal layers of oral squamous epithelium (1, 2, 6) and its cytoplasmic expression was associated with basal proliferating cells (2-4). In oral cancer, membranous moesin is redistributed to the cytoplasm inducing cytoskeleton remodeling (1) and altered expression of this protein contributes to carcinogenesis and metastasis (6, 7). The knockdown of moesin in oral squamous carcinoma cell lines reduced cell migration and invasion, cell spreading and filopodia formation, confirming a role of this protein in tumor progression (6).
We have shown previously the involvement of ERM proteins in mechanisms of cell adhesion, invasion and expansive growth of benign and malignant oral tumors (7-12). In benign odontogenic tumors, the moesin expression was detected mainly in areas of greater epithelial activity, suggesting a participation of this protein in the expansive growth or local invasion of these tumors (11). Furthermore, in oral cancer, moesin overexpression has been considered as an independent prognostic indicator of tumor progression and poorer outcome for patients with oral squamous cell carcinoma (2, 6). Confirming these results, our recent study revealed that strong cytoplasmic expression of moesin in 84 oral squamous cell carcinomas, clinical stage II and III, was an indicator of unfavorable patient's prognosis (7).
Despite previous evidence reinforcing that strong moesin expression is a biomarker of poorer prognosis for oral cancer patients, the participation of this protein, specifically, in lip squamous cell carcinoma has not been investigated. Thus, we decided to analyze the pattern of moesin distribution in the initial stages of lip cancer and its influence in patient's prognosis.
Patients and Methods
From 436 patients who underwent surgical treatment for primary lower lip squamous cell carcinoma, at the Head and Neck Surgery and Otorhinolaryngology Department of the A.C. Camargo Cancer Hospital, São Paulo, Brazil (from 1970 to 2009), 91 were selected for this study, after applying the inclusion criteria, previously established by Assao et al., 2017 (12). Clinical data (age, ethnic group, gender, tobacco and alcohol consumption, TNM stage (UICC, 2004), treatment and clinical follow-up) were obtained from the medical records of the A.C. Camargo Cancer Hospital. Histopathological analysis included vessel infiltration, perineural infiltration, muscular infiltration, glandular infiltration and lymph node involvement. All cases were selected from the pathology archive and Hematoxylin & eosin (HE) staining was performed to classify the tumor according to the grade of malignancy and to select the most representative lip tumor area. The Committee of Ethics and Research of the Bauru School of Dentistry, University of São Paulo, has approved this study (process #551531/2014 – CAAE 01594912.2.0000.5417).

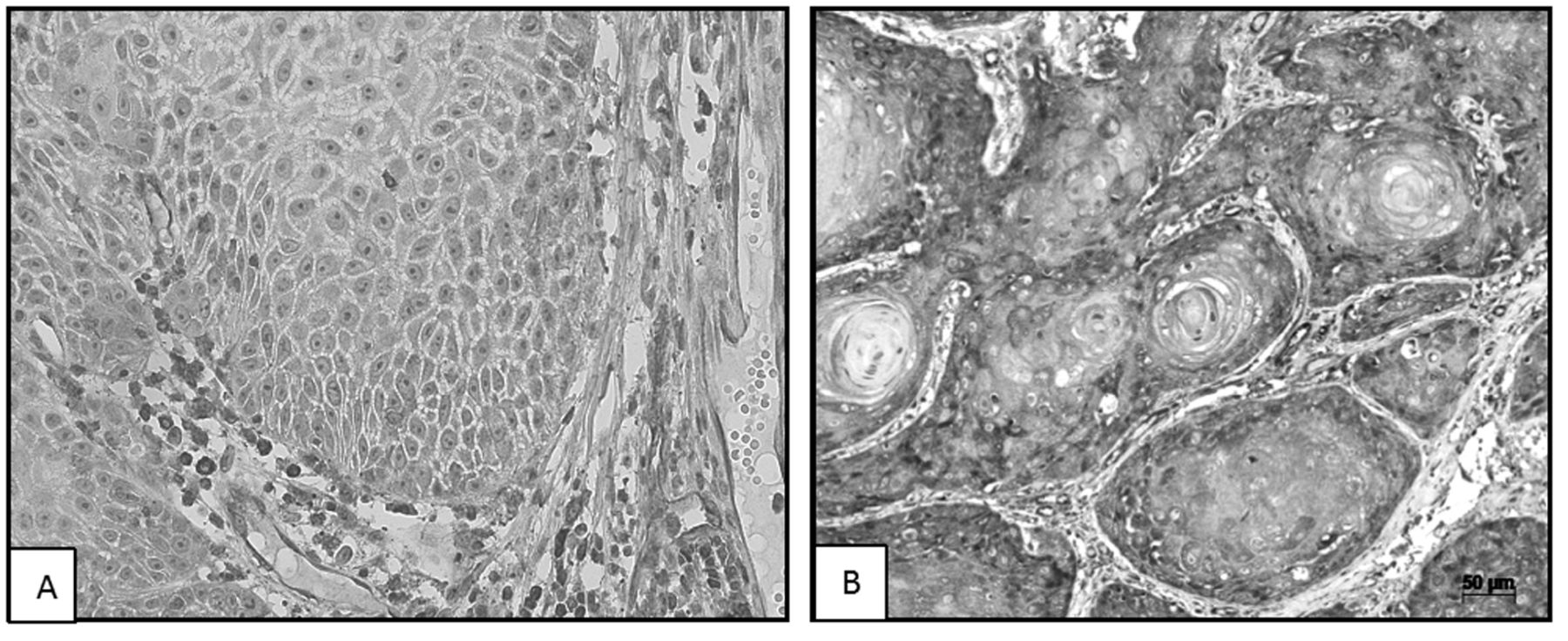
Immunohistochemical expression of moesin by neoplastic cells showing weak/no positivity (A) and strong positivity (B) in lower lip squamous cell carcinomas. (A, IHQ magnification 400×; B, IHQ 200×).
Immunohistochemistry technique. The immunohistochemistry technique followed the protocol of the Department of Pathology of the A.C. Camargo Cancer Hospital. All the selected specimens of squamous cell carcinoma of the lower lip were fixed in 10% buffered formalin, embedded in paraffin and cut into 3 μm-thick sections. The tumor sections were incubated with primary anti-moesin antibody (38/87 clone, Thermo Scientific, LabVision, CA, USA. EUA, dilution 1:400). Then, the antigen–antibody reaction was visualized using 3.3’diaminobenzidine tetrahydrochloride (DAB/SIGMA, ref D-5637, St. Louis, MO, USA) and the tumor sections were counterstained with Mayer haematoxylin. Placenta was used as a positive control for anti-moesin antibody.
Histopathological grade of malignancy of lip cancer. The histopathological grade of malignancy of lower lip squamous cell carcinomas, was determined according to the protocol proposed by Brandwein-Gensler et al. (2005) (13).
Immunohistochemistry evaluation. Moesin expression in 91 squamous cell carcinomas of the lower lip was evaluated in 10 microscopic fields (×400 magnification), sequentially captured at the invasive tumor front. The digital images of each tumor field were recorded in a computer program system (Axiovision 4.9, Zeiss, Jena, Germany).
The assessment of moesin expression in the invasive front tumor, followed a semi-quantitative score system, previously established by Faustino et al. (2008) (14). The final score was determined by the sum of the immunostaining intensity and the percentage of positively immunostained cells. According to the final score, moesin expression was classified as absent (score 0), weak (scores from 1 to 5) and strong (scores 6 to 8) immunoexpression by malignant cells.
Statistical analyses. The obtained results were submitted to statistical analysis using SPSS Statistical version 21.0 software (SPSS Inc., Chicago, IL, USA). The association of the clinicopathological variables and moesin immunoexpression was verified by the Chi-square (×2), or Fischer's exact tests. To estimate the overall and disease-free survival probability in 5 and 10 years, the Kaplan–Meier method was applied, and the survival curves were compared by log-rank test. The period of time between the date of surgery and death, or the date of the last communication with the patient, comprised the follow-up period for overall survival. For all tests, the significant level was set at 5% (p<0.05).
Results
According to the clinicopathological features of patients with lower lip cancer, the sample was predominantly composed of white (100%) male patients (82.4%), with ages varying from 45 to 70 years. Most of the patients used tobacco (81.3%), while alcohol consumption was reported by 53.8% of them.
The majority of the lower lip squamous cell carcinomas were small tumors, clinically classified as T1 (42.2%) and T2 (37.5%), without palpable regional lymph nodes (N0) (79.4%). Fifteen patients presented positive lymph nodes and 27 were submitted to elective neck dissection (15 patients: ipsilateral and contralateral neck dissection, 11 patients: ipsilateral neck dissection, 1 patient: contralateral neck dissection) for squamous cell carcinomas of the lower lip. Clinically, 27 patients were clinical stage I (T1N0M0), 18 patients were clinical stage II (T2N0M0), 14 patients were clinical stage III (T3N0M0; T1, T2, T3N+M0) and 5 patients were clinical stage IV (T4N0MO; T4N+M0), according to UICC (UICC, 2004) criteria.
Post-operatory radiotherapy was not usually indicated for patients with lip squamous cell carcinomas, 76.1% of the patients were not submitted to adjuvant radiotherapy and did not present a second primary tumor (85.7%). From the 91 patients with lip cancer selected for the present study, loco-regional recurrence occurred in 24 patients (19 were local recurrences, 4 were regional recurrences and 1 was in a non-specific local).
Immunoexpression of moesin in lip squamous cell carcinoma. The immunohistochemical expression of moesin in 91 squamous cell carcinomas of lower lip was predominantly strong (80.2%) at the invasive front tumor, while in the central cells of the tumor, in areas of more differentiated neoplastic cells and in keratin pearls, a weak/negative moesin expression was observed (Figure 1A and 1B).
The moesin immunoexpression by malignant cells was not statistically associated with the demographic, clinical and microscopic features analyzed, as described in Table I.
Association of moesin expression with the histopathological grade of malignancy of lip squamous cell carcinoma . The association of moesin expression with the histopathological grade of malignancy of lip squamous cell carcinoma was analyzed by Chi-square test or Fischer's exact test.
Most patients with weak moesin expression (72.2%) presented an intermediate/high risk for local recurrences and lower overall survival; while those patients with strong central moesin expression (50.7%) presented a low risk for local recurrences and lower overall survival (Table II).
Overall and disease-free survivals analyses of patients with lip squamous cell carcinoma. 5 and 10-year overall survival rates for patients with squamous cell carcinoma of the lower lip varied from 0.001 to 394 months (mean of 247 months and standard deviation of 23.3 months).
Moesin expression by cancer cells did not significantly influence the overall survival of patients with lip cancer (p=0.110), however patients with tumors having strong moesin immunoexpression tended to have reduced 5-year and 10-year overall survival rates, 80.8% and 65.8%, respectively (Table III and Figure 2).
Likewise, the disease-free survival rates were not influenced by moesin expression in lip squamous cell carcinoma (Table IV and Figure 3). The 5-year and 10-year disease-free survival rates for patients with lip cancer and strong moesin immunoexpression were 73.9% and 63%, respectively, whereas in patients with tumors having weak moesin expression the disease-free survival rates were 81.9% (5-year) and 81.9% (10-year), as illustrated in Table IV and Figure 3.
Expression of moesin at the invasive tumor front of 91 squamous cell carcinoma of the lower lip, according to clinical data, follow-up and histopathological variables.
Expression of moesin by neoplastic cells according to histopathological grade of malignancy of lip squamous cell carcinomas.
Overall survival rates in 5 and 10 years of 91 patients with squamous cell carcinoma of the lower lip according to clinical variables and moesin expression by neoplastic cells, and histopathological lymph node status.
Discussion
It has been established that altered expression of ERM proteins contributes to carcinogenesis and metastasis (2, 4, 6). Particularly, moesin expression decreases in the membrane and increases in the cytoplasm during oral malignant transformation of the epithelium (1, 2, 6). Meanwhile, the increased expression of membranous moesin in cancer may reflect the requirement of ERM proteins for cell adhesion and contact inhibition (4). In addition, the cytoplasmic overexpression of this protein was correlated with more aggressive tumors and unfavorable prognosis for patients with head and neck squamous cell carcinoma (3, 15), including those with oral cancer (2, 6, 7).
Disease-free survival rates in 5 and 10 years for 91 patients with squamous cell carcinoma of the lower lip according to clinical variables and moesin expression by neoplastic cells, and histopathological lymph node status.
In the present study, the immunoexpression of moesin and its influence in patient's prognosis was investigated, for the first time, exclusively in a sample of 91 lip cancers. We found a predominantly strong cytoplasmic moesin expression by the neoplastic cells at the invasive front of lip squamous cell carcinoma. In contrast, more differentiated cells, as those observed in keratin pearls, showed weak moesin expression as illustrated in the Figure 1. This pattern of moesin expression confirms previous findings in head and neck cancer (1, 2, 4, 6).
The role of moesin as cross-linker between plasma membrane and actin filament was already described (2, 15), however recent investigations in cancer cell lines confirmed that moesin mislocalisation to the cytoplasm of the malignant cells induces cytoskeleton remodeling (2, 6) and contributes to tumor invasion and metastasis, through its interactions with E-cadherin/catenin adhesion complexes (6, 16).
Our clinical findings regarding the overexpression of cytoplasmic moesin at the invasive front of lip cancer suggest that probably it reflects the active functional state of the neoplastic cells that have a higher potential to invade and metastasize. Supporting our results described above, Li et al. (6) correlated the cytoplasmic moesin expression with a more aggressive phenotype and poor prognosis for patients with oral cancer. Likewise, the weak moesin expression observed in more differentiated cells, such as the keratin pearls, found in some tumors of our sample, reinforces the dormant state of neoplastic cells as suggested by Kobayashi et al. (2), Madan et al. (4), Assao et al. (12) and Barros et al. (7).
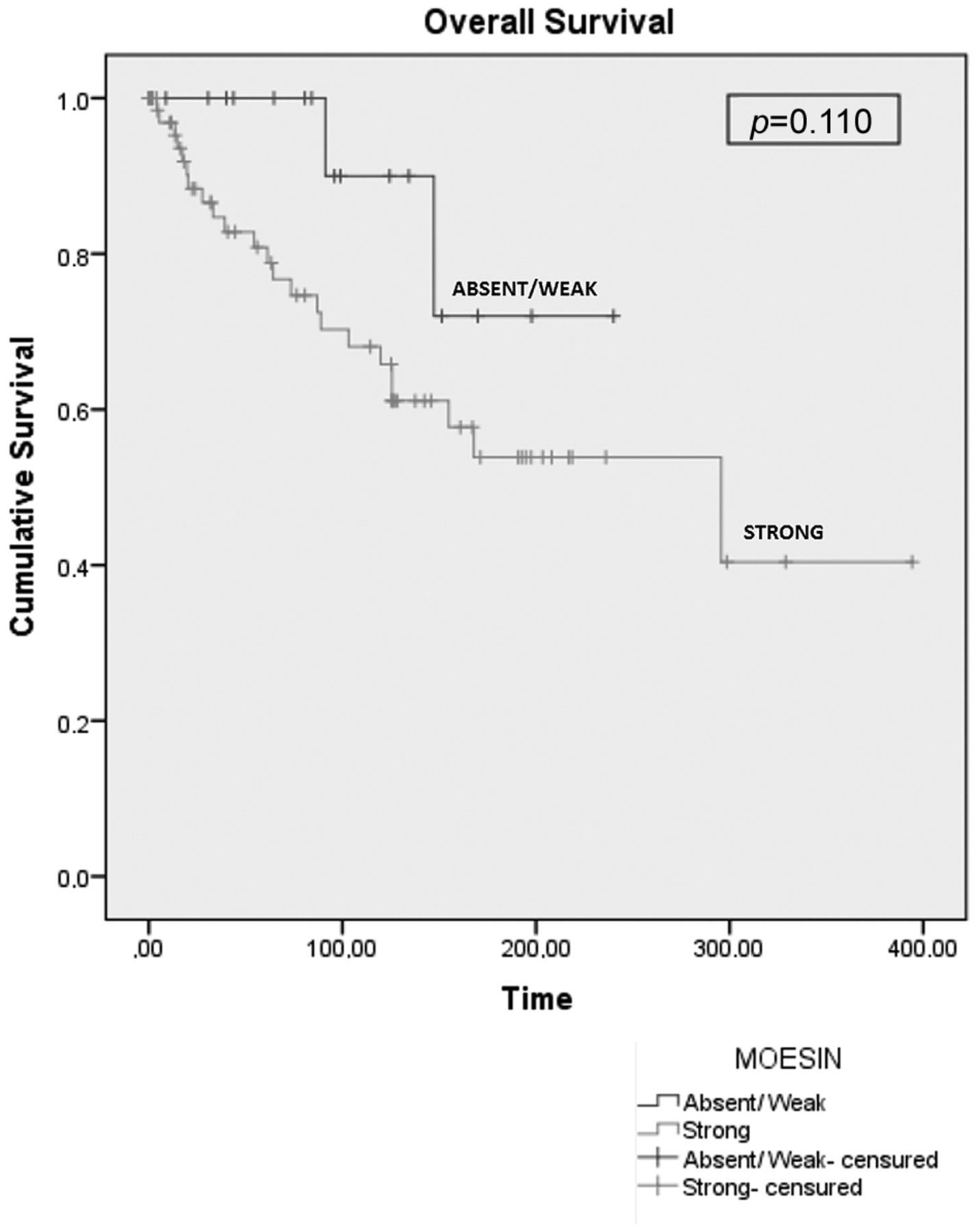
Cumulative overall survival probability for groups with strong moesin and weak/absent moesin expressed by neoplastic cells of the lower lip squamous cell carcinomas. p<0.05 was considered statistically significant.
In order to evaluate the association of moesin expression with the histopathological grade of malignancy of lip cancer, we used a specific index, considered as the best lip cancer histopathological system to predict local recurrences and overall survival (13). There was no statistically significant difference between moesin expression and low or intermediate/high risk score for local recurrences in our patients with lip squamous cell carcinoma (Table II).
The analysis of overall survival by Kaplan–Meier method showed that, as previously described by our research group (12), lymph node metastasis was a significant prognostic factor for patients with lip squamous cell carcinoma. The patients with lip cancer and pN+ showed a reduction in overall 5 and 10 years survival rates, from 67.0% to 34.4%, respectively (Table III). However, most of the patients of our sample were alive and disease-free at the end of the follow up period reflecting an indolent behavior of lip cancer, with good prognosis and higher survival rates (8, 12).

Cumulative disease-free survival probability for groups with strong moesin and weak/absent moesin expressed by neoplastic cells of the lower lip squamous cell carcinomas. p<0.05 was considered statistically significant.
In addition, there is a tendency for patients with lip squamous cell carcinoma and a strong immunoexpression of moesin to have reduced overall and disease-free survivals, as observed in Figures 2 and 3. These survival results for lip cancer patients, although without statistical significance, seem to reinforce moesin as an unfavorable prognostic biomarker for oral squamous cell carcinoma, as described by others (2, 6, 7).
Concluding, our results confirm the participation of moesin in oral carcinogenesis and suggest that this protein influences the survival rates of patients with lower lip squamous cell carcinoma. However, further investigations including a higher number of patients with lip cancer and nodal metastasis are necessary to confirm the role of moesin in tumor progression.
Acknowledgements
The Authors thank São Paulo Research Foundation (FAPESP – grants #2012/13411-6 and #2014/23236-2) and the National Council for Scientific and Technological Development (CNPq) for supporting this study.
Footnotes
Conflicts of Interest
The Authors disclose no conflicts of interest.
- Received February 19, 2018.
- Revision received March 13, 2018.
- Accepted March 14, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.