


Abstract
Background/Aim: In ulcerative colitis (UC) the colonic mucosa shows, in addition to a high number of inflammatory cells, crypts with architectural distortions, called corrupted colonic crypts (CCC). Here we classify the histologic repertoire and assess the frequency of CCC in UC. Patients and Methods: Five-hundred and sixteen histologic sections from 29 colectomy specimens with UC (24 having adenocarcinoma and five, high-grade dysplasia, HGD) were reviewed. Results: The vast majority of the colonic mucosa portrayed countless crypts with normal shapes (CNS) lined with normal epithelium, except for 45 CNS: 28 showed inconclusive-suspected cellular changes (ISCC), and 17, high-grade dysplasia (HGD). CCC were subdivided into four groups: i) Crypts with fission distortions, ii) Crypts with length distortions, iii) Crypts with outline distortions and iv) Crypts with axial polarity distortions. The most frequent CCC group had axial polarity distortions (33.4%), and the less frequent CCC group, outline distortions (21.1%) (p<0.05). No apparent differences in frequency between groups were found in colectomies with HGD/carcinoma, or in colectomies preformed for medically-refractory UC without HGD/carcinoma. Out of the 902 CCC present in the specimens, 343 (38.0%) displayed ISCC, 186 (20.6%) HGD, and the remaining 373 (41.4%) normal epithelium. Hence, of the 203 crypts exhibiting HGD, 186 (91.6%) were CCC and the remaining 17 (8.4%) CNS (p<0.05). Conclusion: Based on these findings it is suggested that the microscopic search for HGD in UC colectomy-specimens should preferentially be focused on mucosal areas exhibiting CCC. This view is validated by recent findings showing that p53 overexpression (a biomarker of epithelial carcinogenesis) significantly correlated with architectural distortions of the crypts in UC.
The normal colonic mucosa is built of a single layer of epithelial cells with inward folds called crypts. Crypts replicate by symmetric fission, beginning at the base of the crypts and proceeding upwards until two identical, individual crypts are created (1). Sections cut perpendicular to the surface epithelium show a characteristic appearance of “row of test tubes” due to tightly packed parallel crypts, “resting” on the muscularis mucosae. A slight variation in the configuration of the crypts and in the space between the crypts may occur, but crypt branching is rare. This architecture is retained throughout the colon, except for innominate grooves (cloverleaf-like crypts connecting to a single lumen) (1). During crypt renewal, stem cells dwelling at the bottom of the crypts, generate amplifying daughter cells that proliferate and differentiate while migrating upwards (2, 3).
In ulcerative colitis (UC) the colonic mucosa exhibits, in addition to high numbers of inflammatory cells, crypts with architectural distortions (4). These crypt distortions usually persist both during the protracted chronic-phase and during disease remission, despite decreased inflammation conveyed by treatment.
Architectural crypt irregularities in UC have received various descriptive terms such as ramification of the crypts (5) considerable branching at the base of the crypts (6), crypt bifurcations (7), architectural aberrations (8), architectural crypt distortion (9) and crypt architectural disarray (10), to name some. In this work, crypts with architectural distortions will be referred to as corrupted colonic crypts (11, 12).
Nearly 30 years ago, Allen et al. used semi-automatic image analysis to assess the architectural irregularities of colorectal mucosa in UC (13). Subsequently, Hamilton et al. applied morphometry and stereology to evaluate the architectural characteristics of regenerative and of dysplastic colorectal mucosa in ulcerative colitis (14). Using neural networks on a mosaic of pixilated images (without any image analysis or image segmentation) the authors concluded that quantitative histological analysis of mucosal abnormalities may be of use in the objective diagnosis of reactive and dysplastic changes in patients with UC (14). More recently, Ficsor et al. (15) reported architectonic irregularities in the colonic mucosa by the aid of automated digital microscopy and advanced digital analysis. Shape-related morphological changes helped to distinguish between normal mucosa and UC. Notwithstanding, the classification of the spectrum of the abnormal shape of the crypts in UC has not been systematically analyzed. In the present work, we classified and assessed the frequency of corrupted colonic crypts (CCC) in a cohort of colectomy specimens from patients with UC.

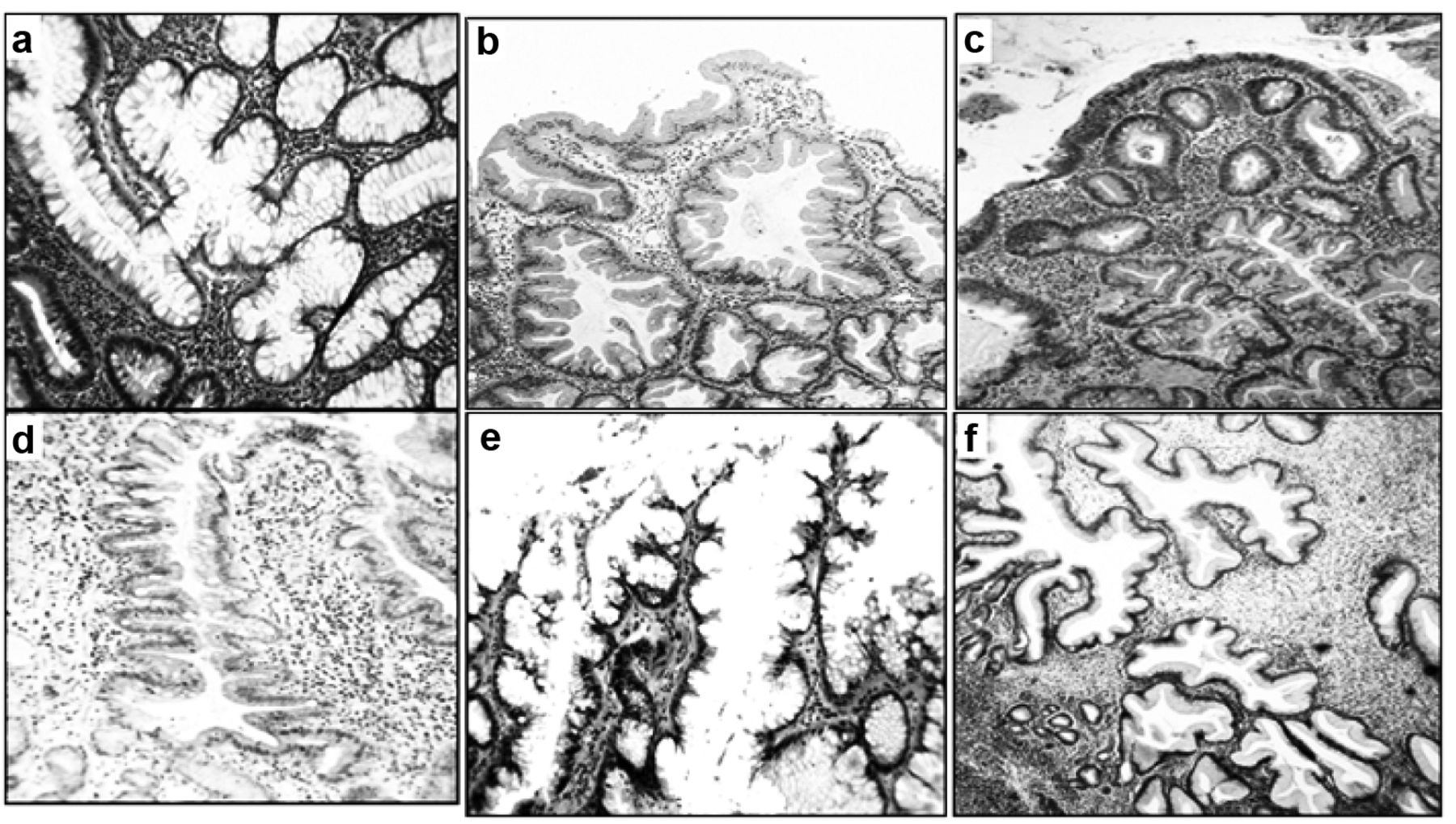
Corrupted colonic crypts with fission distortions (Ulcerative colitis). a: Normal colonic mucosa showing tightly packed, parallel crypts “resting” on the muscularis mucosae, H&E ×20. b-f: Corrupted colonic crypts with fission distortions (ulcerative colitis) b: Colonic crypts with chronic mucosal inflammation, H&E ×4, c: Corrupted colonic crypts with asymmetric fission at arrows. Note expansion of the muscularis mucosa due to chronic inflammation, H&E ×4, d: Corrupted colonic crypts with three asymmetric fissions, H&E ×20, e: Corrupted colonic crypts showing inverted T and L shapes, H&E ×20, g: Corrupted colonic crypts with cystic dilatation, H&E ×20).
Patients and Methods
Archival histological sections from 35 colectomies in patients with UC were reviewed. Six out of the 35 colectomies were rejected from the study: four due to partial mucosal autolysis and the remaining two due to partial faded stainability. In the remaining 29 colectomies, 516 histological sections (mean 17.8, range=10-42 sections) were available for study. Sections were cut at 4 μm thickness and stained with hematoxylin and eosin (H&E). Three colectomy-specimens performed because of severe UC, refractory to clinical treatment (without carcinoma or high-grade dysplasia (14) were included as controls.
CCC were subdivided into four groups: i) Crypts with fission distortions, ii) Crypts with length distortions, iii) Crypts with outline distortions, and iv) Crypts with axial polarity distortions (in relationship to the muscular is mucosae).
The epithelial lining in CCC displayed the following features: a) Normal epithelium, b) Inconclusive or suspected cellular changes (ISCC), ranging from cell regeneration to possibly low-grade dysplasia. CCC lined with ISCC were often seen in areas with chronic-active inflammation, with ulcerated mucosa or with severe chronic inflammation without acute inflammation, c) High-grade dysplasia (HGD) as defined by Riddell et al. (16).
Statistical analysis. The non-parametric Kruskal-Wallis test was applied, to compare difference between groups. Statistical significance was defined as p<0.05.
Results
Clinical data. Gender: Twenty-two were males and the remaining seven, females.
Age: The mean age at colectomy was 48.1 years (range=32-65 years).
No. of years with UC prior surgery: The mean number of years with UC prior surgery was 20.7 (range=10-32 years).
Histological findings. The histological examination of the 29 colectomy specimens revealed adenocarcinoma in 24 and high-grade dysplasia in the remaining five.
The vast majority of the colonic crypts both in areas with or without chronic inflammation, exhibited normal shapes (CNS) lined with normal epithelium, except from 45 CNS: 28 showing ISCC, and 17, unequivocal high-grade dysplasia (HGD).

Corrupted colonic crypts with length distortions (ulcerative colitis). a: Two hyperplastic corrupted colonic crypts with multiple asymmetric fissions (H&E ×2), b and c: Hyperplastic corrupted colonic crypts, H&E ×4, d: Atrophic corrupted colonic crypts, H&E ×2, e-f: Atrophic corrupted colonic crypts, H&E ×4.

Corrupted colonic crypts with outline distortions (ulcerative colitis). a: Mullti-lobate crypts, H&E ×4), b: Corrupted colonic crypts with serrated architecture, H&E ×4, c: Corrupted colonic crypts with serrated architecture, at arrow, H&E ×2, d: Detail of corrupted colonic crypt with serrated architecture, H&E ×10, e-f: Crypts with microtubular-like scalloped borders, H&E ×10 and ×4).
The histological evaluation also revealed a total of 902 CCC in the 29 colectomy specimens (mean 31.1 CCC/colectomy, range=22-48 CCC/colectomy). Two or more of the following histologic phenotypes could be found in each group: i) CCC with fission distortions: included asymmetric crypt fissions and cystic crypts (Figure 1), ii) CCC with length distortions: comprised hyperplastic crypts and atrophic crypts (Figure 2), iii) CCC with outline distortions: encompassed mullti-lobate-scalloped crypts, and crypts with: i) serrated outlines, and ii) microtubular outlines (Figure 3), and iv) CCC with axial polarity distortions in relation to the muscularis mucosae: included meandering-serpentine crypts, inter communicating crypts, ring-shaped crypts, inverted L shapes and horizontal ring-shaped crypts (Figure 4).

Corrupted colonic crypts with axial polarity distortions, in relation to the muscularis mucosae (ulcerative colitis). a-c: Meandering-intercommunicating crypts, H&E ×4, d: Ring-shaped crypts, e: Cystically-dilated crypt with multiple irregular fissions, f: Ring-shaped crypts “rising” in one hyperplasic crypt, H&E ×4.
The frequency of histological groups of CCC (corrupted colonic crypts) found in 29 colectomy specimens in patients with ulcerative colitis having carcinoma (n=24), or high-grade dysplasia (n=5). Three additional colectomy specimens performed because of severe UC refractory to clinical treatment (without carcinoma or HGD) are also shown.
The most frequent CCC-group (33.4%) portrayed crypt axial-polarity distortions (in relationship to the muscular is mucosae), and the less frequent CCC-group (18.7%), crypt-outline distortions (p<0.05) (Table I).
Epithelial lining in CCC. Out of a total of 902 CCC, 373 (41.4%) had normal epithelial lining, 343 (38.0%) inconclusive or suspected cellular changes (ISCA) and the remaining 186 (20.6%), HGD (Figure 5). CCC with normal epithelium/ISCA vs. HGD, p<0.05). Out of the 203 colonic crypts with HGD 186 (91.6%) occurred in CCC and the remaining 178 (4%) in CNS/ISCC (p<0.05).
Discussion
A systematic analysis of the spectrum of the colonic crypts with abnormal configurations, called CCC, was carried out in colectomy specimens with UC. The scrutiny revealed a high number of CCC exhibiting a wide range of architectural phenotypes. Rationally, the crypts with ornamentation distortions were generated by the chronic inflammation. And yet, large mucosal areas with chronic inflammation in the specimens had none to occasional CCC. In similarity with these findings, none to occasional CCC were found in a variety of colonic diseases with chronic inflammation such as diverticular disease-associated colitis (17), diversion colitis (18), lymphocytic colitis (19), radiation colitis (20), collagenous colitis (21), ischemic colitis (22), chronic colitis in Behçet's disease (23) and non-specific ulcers of the colon (24). A rational explanation for these findings might be that the CCC in UC might have been generated by factors other than ongoing chronic mucosal inflammation. One possible candidate might be abnormal mucosal regeneration in areas with formerly mucosal denudation. In this context, CCC were recently found in mucosal areas bordering regenerating UC ulcers (11). Why the process of mucosal regeneration severely alters the normal architecture of the colonic crypts surrounding ulcers in colitic patients, remains enigmatic. Nevertheless, since chronic mucosal inflammation per se might not be crucial for the development of CCC (17-24), we are prone to speculate that the CCC found in the non-ulcerated colonic mucosa in UC could represent abnormal crypt regeneration in areas with formerly mucosal ulcerations in colitic patients (11).

Corrupted colonic crypts with high-grade dysplasia (ulcerative colitis). a, b: H&E ×4, c: H&E x4, d-f: ×20.
The significance of ISCA, often found in CCC in UC, remains challenging. This since McKenna and Appelman (25) postulated that the category ‘indefinite for dysplasia’ is an honest recognition of the difficulties in distinguishing reactive or regenerative epithelium from low-grade dysplasia. Moreover, studying inter-observer variation between pathologists regarding the degree of dysplasia in UC, Eaden et al. (26) found total concordance of the 13 pathologists in only four of the 51 slides. Agreement was best for high-grade dysplasia. Based on those findings we opted for classifying crypts with regenerative, ‘indefinite for dysplasia’ or low-grade dysplasia (25) as with ISCC, and those with HGD (the histological phenotype less amenable to diagnostic disagreement) (26). In conventional colonic adenomas, HGD initially develops at the luminal aspect of the crypts and progress downwards, towards the base of the crypts (27).
In UC, in contrast, dysplasia initially develops at the base of the crypts and progresses upwards, towards the luminal aspect of the crypts (28). In CCC, we found normal epithelial lining in >40%, ISCC in 38% and HGD in >20%. The finding that HGD was often found in the lower aspect of the CCC is in concert with the “bottom-up” replacement of the crypts by up-growing dysplastic cells in UC (28). It has been suggested that the CCC might act as scaffolds at the time of “bottom-up” replacement by up-growing mutated dysplastic cells, a notion previously advanced for carcinogen-induced conventional adenomas in experimental animals (12). The same crypt replacement by dysplastic cells may apply to serrated adenomas and microtubular adenomas, inasmuch as CCC with serrated and microtubular configurations lined by normal epithelium occurs in patients with UC (cfr. Figure 3) (29-33).
One possible practical implication of the present findings might be that the microscopic search for HGD in UC-colectomies should primarily be focused on mucosal areas exhibiting CCC. This notion is validated by recent findings by Popp et al. (34) showing that p53 overexpression (a biomarker of epithelial carcinogenesis) significantly correlated with architectural distortions of the crypts in UC (34). The results of Popp et al. (34) seem to be in concert with the our findings, inasmuch as HGD in UC was mainly found in CCC.
In closing, while cellular descriptions and molecular signals that control cell proliferation and cell mutations during carcinogenesis in UC have received much attention (35-40), the signals that might be instrumental in designing morphogenesis (41) resulting in the “etching” of various CCC phenotypes in UC, have remained unattended.
Footnotes
This article is freely accessible online.
- Received February 13, 2018.
- Revision received February 28, 2018.
- Accepted March 1, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}