


Abstract
Background: No standard second-line chemotherapy has been yet established for gemcitabine-refractory biliary tract cancer (BTC). Patients and Methods: We conducted multivariable Cox regression analysis to examine the prognostic factors for overall survival (OS) in patients who had received gemcitabine-based treatment. Results: Forty-six patients received second-line chemotherapy. The median serum carbohydrate antigen 19-9 (CA 19-9) value was 487 U/ml. The modified Glasgow prognostic score (mGPS) was: 0 (n=24), 1 (n=10), or 2 (n=10). The second-line chemotherapy included: S-1 in 20 patients, gemcitabine-based in 20, and tyrosine kinase inhibitors in five. The median OS was 8.3 months, and the median progression-free survival was 3.0 months. Multivariate analysis identified serum CA 19-9 ≥500 U/ml, mGPS ≥1, and presence of liver metastasis as significant prognostic factors for OS. Conclusion: Second-line chemotherapy for gemcitabine-refractory BTC remains inadequate. Randomized trials with appropriate stratification criteria are required.
Gemcitabine plus cisplatin is widely recognized as the standard first-line chemotherapy for advanced biliary tract cancer (BTC) because randomized controlled trials have demonstrated an improved overall survival (OS) in patients receiving gemcitabine plus cisplatin compared to patients receiving gemcitabine monotherapy (1, 2). Although most patients develop tumor progression during gemcitabine plus cisplatin treatment, there are no published reports of randomized clinical trials of second-line chemotherapy in patients with gemcitabine-refractory BTC. Since S-1 has been approved for use in patients with BTC, S-1 has been commonly used for second-line chemotherapy in patients with gemcitabine-refractory BTC in Japan. To date, the usefulness of S-1 has been evaluated in two single-arm clinical trials. In one, the response rate (RR), median progression-free survival (PFS) and median OS were 22.7%, 5.4 months and 13.5 months, respectively (3). In the other, the RR, median PFS and median OS were 7.5%, 2.5 months and 6.8 months, respectively (4). Thus, the efficacy of S-1 as second-line chemotherapy differed between the two clinical trials. We speculated that the differences in the sample size and patient backgrounds, such as history of surgery, were responsible for the difference in efficacy between the two trials. Therefore, no standard chemotherapy has been established yet for patients with gemcitabine-refractory BTC.
The modified Glasgow prognostic score (mGPS) is based on the serum C-reactive protein (CRP) and serum albumin levels, and is an inflammation-based prognostic factor (5). It has been recognized as a prognostic factor in patients with various types of solid tumors (6, 7). To the best of our knowledge, there is no report on the relationship between mGPS and OS in patients with gemcitabine-refractory BTC receiving second-line chemotherapy.
Therefore, we carried out a retrospective evaluation of the efficacy of second-line chemotherapy and the prognostic factors for OS in patients with gemcitabine-refractory BTC receiving second-line chemotherapy. Furthermore, we investigated the relationship between the mGPS and OS in the setting of second-line chemotherapy.
Patients and Methods
Study population. We retrospectively examined the data of patients with advanced BTC who had received first-line treatment with a gemcitabine-based regimen between January 2009 and December 2015 at Kyorin University Hospital. Patients with histologically confirmed unresectable or recurrent BTC, including intrahepatic bile duct, extrahepatic bile duct, gallbladder and ampulla of Vater cancer, who had received first-line chemotherapy were reviewed. Among 102 patients who had received a gemcitabine-based regimen as first-line treatment, 46 patients (45%) also received second-line chemotherapy (Figure 1). We analyzed the incidence of adverse events (AEs), the antitumor effect of the treatment, PFS, OS and prognostic factors associated with OS in the patients who were receiving second-line chemotherapy. One patient was excluded from this study because the second-line chemotherapy was initiated at another hospital. This study was conducted with the approval of the local Institutional Review Board (approval number: 795).

Consort diagram. Among 102 patients treated with a gemcitabine (gemcitabine)-based regimen as first-line treatment, 46 patients (45.1%) received second-line chemotherapy.
Assessment of response and AEs. The tumor response was evaluated by computed tomography (CT) or magnetic resonance imaging (MRI), in accordance with the Response Evaluation Criteria in Solid Tumors 1.1. CT and MRI were basically performed every 2 to 3 months until confirmation of progressive disease. Adverse events were recorded in accordance with the Common Terminology Criteria for Adverse Events 4.0.
Analysis of prognostic factors. All data were collected before the second-line chemotherapy was initiated. The mGPS was calculated using the serum CRP and serum albumin as follows: Patients with a normal serum CRP level were assigned a score of 0, patients with both elevated serum CRP (≥1.0 mg/dl) and reduced serum albumin level (<3.5 g/dl) were assigned a score of 2, patients with only elevated serum CRP level were assigned a score of 1. Factors potentially influencing OS were selected as follows: age (<70 vs. ≥70 years), gender, Eastern Cooperative Oncology Group performance status (ECOG PS) (0 vs. 1), history/no history of prior surgical resection, PFS after first-line treatment (<6 months vs. ≥6 months), primary tumor site (non-gallbladder vs. gallbladder), presence/absence of liver metastasis, lung metastasis and/or peritoneal dissemination, serum alkaline phosphatase (ALP) level (<400 IU/l vs. ≥400 IU/l), serum carbohydrate antigen 19-9 (CA19-9) level (<500 U/ml vs. ≥500 U/ml), mGPS (0 vs. 1 or 2), and chemotherapy regimen (monotherapy vs. combination therapy). The patients were divided into two groups based on levels higher and lower than the median age, ALP and CA19-9 level.
Statistical methods. PFS and OS were calculated using the Kaplan–Meier method and differences were evaluated using the log-rank test. Univariate analysis was first performed to identify the prognostic factors for OS in the patients receiving second-line chemotherapy. Factors identified by univariate analysis as being statistically significant (p<0.05) were entered into Cox proportional hazard regression model using a stepwise procedure for multivariate analysis. The statistical analyses were performed by the statistical software package SPSS version 22.0 for Windows (IBM Corp., Armonk, NY, USA).
Results
Patients characteristics. The patients characteristics are shown in Table I. The mGPS could not be calculated for one patient because serum albumin data were missing. A total of 102 patients received gemcitabine-based treatment between January 2009 and December 2015 at our hospital. Of these, 28 patients (27%) were judged as not being suitable candidates for second-line chemotherapy because of poor general physical conditions. Eight patients (8%) wished to receive only palliative care despite being considered as suitable for receiving second-line chemotherapy. Seven patients (7%) could not receive second-line chemotherapy because of obstructive jaundice as a result of unsuccessful biliary drainage. Complete response (CR) was achieved in two patients (2%), pathological CR was achieved in one patient after 2 years of intensive combined chemotherapy with gemcitabine and S-1 (8). There was one (1%) treatment-related death due to intestinal pneumonia induced by gemcitabine. Thus, 46 (45%) patients with gemcitabine-refractory BTC who received second-line chemotherapy were finally eligible for this study. However, we excluded one patient because his treatment had been started at another hospital, and finally included 45 patients in this study (Figure 1).
Patients characteristics.
Second-line chemotherapy (n=45).
Second-line chemotherapy. The second-line chemotherapy regimens used are listed in Table II. Forty-five patients received second-line chemotherapy. S-1 used as the standard chemotherapy and as part of a clinical trial of patients with gemcitabine-refractory BTC. Gemcitabine plus oxaliplatin and tyrosine kinase inhibitors selected as part of a clinical trial in some patients. Gemcitabine plus cisplatin was selected in patients with BTC refractory to gemcitabine plus S-1. Gemcitabine monotherapy was selected in patients in whom the second drug had to be discontinued because of the emergence of AEs in response to combination therapies such as gemcitabine plus cisplatin or gemcitabine plus S-1. Gemcitabine plus S-1 is selected in clinical practice in patients with BTC refractory to gemcitabine plus cisplatin. Fixed-dose gemcitabine plus S-1 was selected by the physicians because this combination as first-line chemotherapy has been shown to be highly effective: The patient had a target lesion in lymph node before first-line chemotherapy. The target lesion was a maximum tumor size reduction of 75% and PFS was 10.3 months.
Efficacy and safety. There were no patients with CR or PR. The tumor response was classified as stable disease in 26 (57.8%) patients and as progressive disease in 37 (37.8%) patients. Antitumor effect was not evaluated in two patients because these patients were shifted to palliative care because they developed biliary tract infection immediately after the start of chemotherapy. The RR was 0% and the disease control rate was 57.8% for second-line chemotherapy in patients with gemcitabine-refractory BTC.
The PFS and OS curves are shown Figure 2. The median PFS and OS were 3.0 months [95% confidence interval (CI)=1.4-4.5 months] and 8.3 months (95% CI=4.7-11.9 months), respectively.
The most commonly encountered grade 3 or 4 AEs were bone marrow suppression and biliary tract infection. In regard to hematological grade 3 or 4 AEs, neutropenia, anemia and leukopenia were observed in five (11%), five (11%), and one (2%) patient, respectively. In regard to non-hematological grade 3 or 4 AEs, biliary tract infection, anorexia, thromboembolic events, hand–foot syndrome, hypertension, and creatine phosphokinase increased were observed in six (13%), one (2%), one (2%), one (2%), one (2%), and one (2%) patient, respectively. There was one treatment-related death due to biliary tract infection.
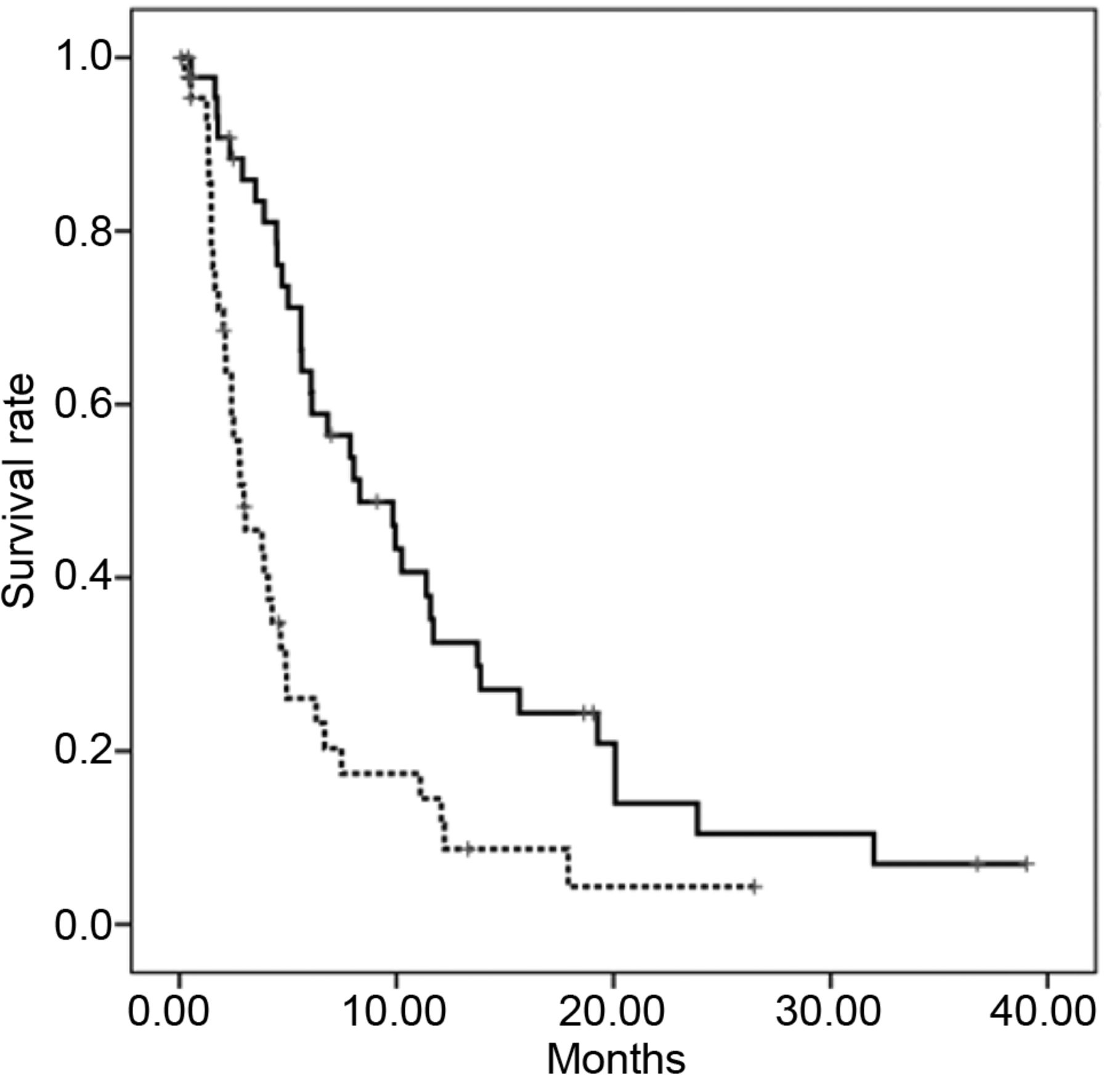
Kaplan–Meier curves for overall survival (black line) and progression-free survival (dotted line). The median progression-free survival and overall survival were 3.0 (95% confidence interval=1.4-4.5) months and 8.3 (95% confidence interval=4.7-11.9) months, respectively.
Univariate and multivariate analysis to identify factors affecting OS. In the univariate analysis, ECOG PS, PFS after first-line treatment, liver metastasis, ALP level, CA 19-9 level and mGPS were identified as prognostic factors for OS (Table III). The variables that were identified by univariate analysis were entered into the multivariate analysis model. Multivariate analysis identified raised serum CA 19-9 level, mGPS >0 and presence of liver metastasis as an independent prognostic factors for reduced OS (Table IV).
Association of the mGPS with OS. The relationship between the mGPS and OS is shown Figure 3. The median OS values were 11.7 months (95% CI=6.2-17.2 months), 9.8 months (95% CI=0.7-18.9 months) and 4.5 months (95% CI, 1.2-7.7 months) in patients with mGPS 0, 1, and 2, respectively. The log-rank test showed significant differences (p=0.01) among the three groups.

Kaplan–Meier curves for overall survival according to the modified Glasgow prognostic factor (mGPS). The median overall survival was 11.7 (95% confidence interval=6.2-17.2) months, 9.8 (95% confidence interval=0.7-18.9) months and 4.5 (95% confidence interval=1.2-7.7) months in the patient groups with mGPS 0, 1 and 2, respectively. The log-rank test showed significant differences among the groups (p=0.01).
Discussion
This retrospective study conducted on patients with gemcitabine-refractory BTC receiving second-line chemotherapy showed a RR of 0%, DCR of 57.8%, median PFS of 3.0 months, and median OS of 8.3 months. Furthermore, mGPS was identified as an independent prognostic factor for OS in patients with gemcitabine-refractory BTC receiving second-line chemotherapy, and the OS was found to be dependent on the mGPS.
Although gemcitabine plus cisplatin has been used as effective first-line chemotherapy, most patients show tumor progression over time. However, there are no established second-line chemotherapies for patients with gemcitabine-refractory BTC. To date, some single-arm trials have shown modest efficacy of second-line chemotherapy, with a median OS and PFS of 4.1 to 13.5 months and 1.6 to 5.4 months, respectively (3, 4, 9-17). Our results were similar to previous reports of the efficacy of second-line chemotherapy in patients with advanced BTC. The second-line treatments used to date do not seem to have sufficient antitumor efficacy.
The current study demonstrated a transition rate from first-line treatment to second-line chemotherapy of 45%. Even though patients receiving gemcitabine-based first-line treatment eventually develop tumor progression, about 50% of these patients with gemcitabine-refractory BTC need an effective second-line chemotherapy. Thus, establishment of second-line chemotherapy for patients with advanced BTC is urgently required.
Univariate analysis to identify prognostic factors for overall survival (OS) in patients receiving second-line chemotherapy.
Analyses of prognostic factors identified high serum CA19-9 level, a high mGPS score and the presence of liver metastasis as independent poor prognostic factors. Previous studies have reported presence of ascites, lack of response to first-line chemotherapy, elevated serum CA19-9, poor PS, no history of surgery for the primary tumor, intrahepatic bile duct cancer, and presence of metastatic disease as poor prognostic factors for OS in patients with advanced BTC receiving second-line chemotherapy (18-21). Although inflammation-based prognostic factors, such as the mGPS, have been demonstrated as prognostic factors in patients with BTC receiving first-line chemotherapy or undergoing surgical resection (22-28), there have been no reports yet of identification of such factors as having an influence on the prognosis in patients with gemcitabine-refractory BTC receiving second-line chemotherapy. The results of our current study suggest that inflammation-based prognostic factors are important in patients with BTC receiving second-line chemotherapy, just as in patients receiving first-line chemotherapy or undergoing surgical resection.
Multivariate analysis to identify prognostic factors for overall survival in patients receiving second-line chemotherapy.
This study had several limitations. Firstly, it was retrospective in its nature, the sample size was small and it was a single-center study. Secondly, it included patients treated before gemcitabine plus cisplatin was approved in Japan. Finally, various second-line chemotherapy regimens, including clinical trial regimens, were used. Therefore, a prospective multi-center study is needed to confirm the conclusions of this study in regard to these prognostic factors.
In conclusion, second-line chemotherapy using existing drugs such as S-1 has only modest activity against gemcitabine-refractory BTC. Randomized controlled trials using newer agents and appropriate stratification criteria for the patients, including serum CA19-9, mGPS, and presence/absence of liver metastasis, are required to establish a standard second-line chemotherapy for gemcitabine-refractory BTC.
- Received November 30, 2017.
- Revision received January 9, 2018.
- Accepted January 11, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}