


Abstract
Background/Aim: We evaluated the effects of storage of formalin-fixed, paraffin-embedded (FFPE) sections on the tumour proportion score (TPS) for programmed cell death ligand 1 (PD-L1), as indicator in non-small cell lung cancer (NSCLC) tissues of treatment efficacy. Materials and Methods: NSCLC postoperative specimens with PD-L1 TPS ≥50% were obtained and cut into five serial sections. One section was stained immediately, and four were stored at 4°C for 2, 4, 6, or 8 weeks. Slides were subjected to PD-L1 immunohistochemistry using the anti-PD-L1 clone 28-8. PD-L1 TPS were blindly evaluated by two independent pathologists. Results: Twelve specimens (60 slides) were evaluated. After slide storage for 2, 4, 6, and 8 weeks, a TPS of <50% was obtained in five (41%), four (33%), seven (58%), and eight (67%) patients, respectively. Conclusion: TPS values for PD-L1 were reduced by long-term slide storage of FFPE specimens. Sectioned slides should be stained for PD-L1 without delay.
Lung cancer is the leading cause of cancer-related deaths worldwide, and non-small cell lung cancer (NSCLC) accounts for approximately 80% of all lung cancer cases (1). Programmed cell death 1 (PD-1) axis inhibitors have efficacy in patients with advanced NSCLC (2, 3). Moreover, previous studies have revealed that the tumour proportion score (TPS) for programmed cell death ligand 1 (PD-L1), i.e. the proportion of positively-stained cells by immunohistochemistry (IHC), is a predictive biomarker for the efficacy of PD-1 axis therapies (4, 5). Following the KEYNOTE 024 trial, pembrolizmab (Merck Sharp and Dohme, Kenilworth, NJ, USA) was approved as a first-line therapy for patients who are strongly positive for PD-L1 (TPS ≥50%) (6).
PD-L1 IHC results determine the treatment strategy for patients with NSCLC. If patients with a true PD-L1 TPS ≥50% are evaluated as having a TPS of less than 50%, they cannot receive immunotherapy as a first-line treatment, yielding a shorter overall survival. Currently, predictive markers other than PD-L1 IHC are not available. Therefore, an accurate evaluation of PD-L1 TPS is necessary.
The accuracy of staining results is limited by technical issues. In fact, the long-term storage of paraffin tissue sections leads to a loss of IHC antigenicity to human epidermal growth factor receptor 2 (HER2), p53, and other antibodies (7, 8). According to the guideline on HER2 testing established by the American Society of Clinical Oncology (ASCO)/College of American Pathologists (CAP), specimens should be stained within 6 weeks of sectioning to minimize false-negative results (9). The ATLAS of PD-L1 IHC testing in lung cancer published by the International Association for the Study of Lung Cancer (IASLC) recommends that sectioned slides be stained within 3 months (10). However, to the best of our knowledge, a time-course analysis of PD-L1 IHC results after sectioning has not been performed. The extent of antigenicity loss depends on the type of antigen, and the algorithm for IHC evaluation differs between HER2 and PD-L1. Therefore, it is necessary to investigate the time course of PD-L1 IHC in sectioned slides in order to comprehensively identify candidates for therapy with PD-1 axis inhibitors.
In this study, we investigated the time course of TPS for PD-L1 in NSCLC postoperative paraffin slide sections using clone 28-8 anti-PD-L1 (complementary diagnostics for nivolumab) and proposed optimal pathological processing methods for accurate PD-L1 assessment.
Patient characteristics.
Materials and Methods
Patient selection criteria and study design. This study was part of a retrospective study that compared the TPS for PD-L1 of patients with NSCLC with or without interstitial lung disease (ILD) (unpublished data). Patients with pathological stage I or II NSCLC who underwent surgery at Kobe City Medical Center General Hospital (Hyogo, Japan) between January 2007 and January 2016 were reviewed. In total, 826 patients were included in the study, and PD-L1 status was screened in 124 randomly selected patients. Among them, 12 patients had TPS for PD-L1 of at least 50%. The formalin fixation time was 24-72 h. Using FFPE postoperative specimens, five new serial sections were made of each specimen, four of which were stored at 4°C for 2, 4, 6, or 8 weeks. Patients who reported never having smoked were defined as never smokers, those who had smoked within 1 year of their diagnosis were categorised as current smokers, and the remaining patients were considered former smokers. The FFPE storage period was defined as the period from the day of operation to IHC staining. This study was approved by the Ethics Committee of Kobe City Medical Center General Hospital (zn170303).
Tissue processing and evaluation of IHC. Rabbit monoclonal anti-PD-L1 clone 28-8 were used (Abcam, Cambridge, UK). Tissue sections (4 μm-thick) were cut from FFPE tumour blocks and then routinely deparaffinised and rehydrated (95°C for 20 min). The antibody was diluted 1:500 and applied according to DAKO (Glostrup, Denmark) recommended detection methods (11-13). Tumour PD-L1 scores were evaluated by two independent pathologists (K.U. and Y.I.). Specimens were considered PD-L1-positive when the cell membrane was partially or completely stained, irrespective of staining intensity. Haematoxylin and eosin (HE) staining was used for each case to help orientate the pathologists' reading of the IHC slides. TPS was estimated in increments of 10%. According to previous reports, we set the cutoff value as 50% (6). Namely, patients with TPS of at least 50% were considered strongly positive, patients with TPS of 0-49% were considered weakly positive or negative. Specimens classified as TPS <50% were defined as false-negatives. Each slide was anonymised and randomised. Two weeks after the independent examination, PD-L1 TPS were confirmed by a central review.
Comparison of patient characteristics between impaired and unimpaired tumour proportion score for programmed cell death ligand 1.
Results
Patients and specimen characteristics. A total of 12 specimens (60 slides) were included in this study. Patient characteristics are summarised in Table I. All patients were male smokers, and the majority had stage I disease (n=9, 75%) with squamous cell histology (n=10, 83%). Five patients (42%) had ILD, and the median PD-L1 TPS was 60% [interquartile range (IQR): 50-67.5%]. The FFPE storage period was 45.0 months (IQR: 22.3-91.9 months).
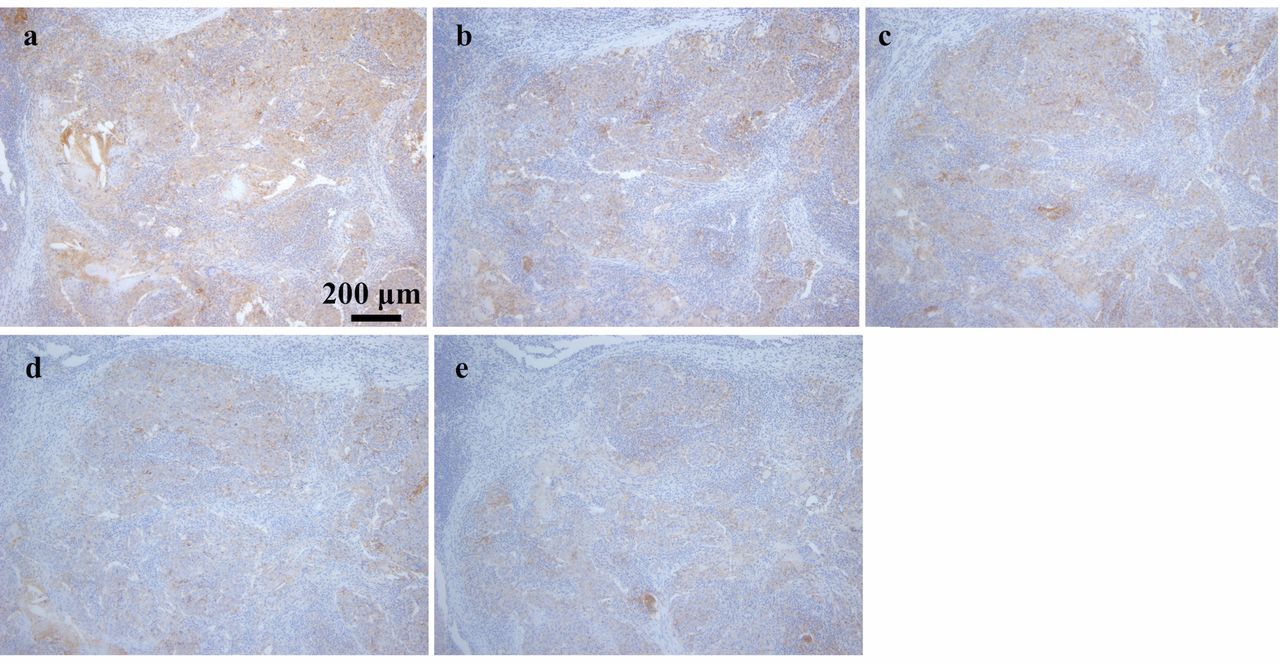
Relationship between PD-L1 TPS and storage period. Generally, PD-L1 IHC results became less accurate over time. Representative IHC examples are shown in Figure 1. After 2, 4, 6, and 8 weeks storage, specimens of five (41%), four (33%), seven (58%), and eight (67%) patients were classified as weakly positive (Figure 2).

Representative immunohistochemistry results for programmed cell death ligand 1 using clone 28-8 antibodies: a: freshly-stained specimen; b: 2 weeks of storage; c: 4 weeks of storage; d: 6 weeks of storage; e: 8 weeks of storage (×100).
Differences between patients with impaired and unimpaired TPS. After 8 weeks, the TPS for PD-L1 of eight patients (67%) changed from strongly positive to weakly positive. The unchanged group was composed of patients with stage I disease; however, there were no apparent clinical differences in age, smoking status, histology, presence of ILD, stage, and FFPE storage period among patients with impaired and unimpaired TPS (Table II).
Discussion
To the best of our knowledge, this is the first study demonstrating the time course of PD-L1 TPS after sectioning. Our results revealed that the TPS for PD-L1 decreased substantially over time. A reduction in TPS resulted in an underestimation of the PD-L1 status, yielding false-negative results for patients with initially strongly positive PD-L1 results.
In our study, we found two important features of PD-L1 IHC results according to the time since sectioning. Firstly, there was an apparent impairment, which caused an underestimation of the PD-L1 TPS after long-term storage. Surprisingly, slide storage for 6 weeks or more yielded false-negative PD-L1 staining results in more than half of patients with strongly positive PD-L1 on freshly sectioned slides. These results are consistent with those of previous reports indicating the impairment of HER2, p53, and Ki-67 IHC staining after long-term slide storage (7, 8, 14-16). Secondly, the observed impairment started 2 weeks after sectioning. Similarly, a previous report demonstrated that p53 staining was impaired after only 2 weeks of storage (7). The PD-L1 TPS determines the patient's prognosis; therefore, we believe that our findings have significant implications for daily clinical practice. Although the ATLAS of PD-L1 IHC testing in lung cancer recommends that sectioned slides be stained within 3 months, clinicians and pathologists should not permit any delay between sectioning and the IHC procedure to ensure the identification of all candidates for therapy with PD-L1 axis inhibitors.

Changes in distribution of the tumour proportion score (TPS) for programmed cell death ligand 1 (PD-L1), using a 50% cutoff. After 2, 4, 6, and 8 weeks of slide storage, false-negative results were observed in five (41%), four (33%), seven (58%), and eight (67%) patients, respectively.
Previous studies have shown that some IHC intensities decrease with long-term slide storage, and a loss of antigenicity of HER2 and p53 has also been reported in tissue microarrays (7, 14-18). However, the IHC intensity of oestrogen receptor staining is not affected, and that of vimentin is even elevated by slide storage (8, 15). These reports imply that the impairment of antigenicity is not a uniform phenomenon but is specific to each antibody. Oxidation of antigens plays an important role in the loss of antigenicity (10, 19). In fact, IHC results are dependent on various conditions, including slide storage duration, storage temperature, FFPE storage period, and antigen retrieval conditions. In this report, we revealed that PD-L1 IHC results become less accurate with storage of slide sections. More studies are needed to optimise the methods for PD-L1 IHC evaluation.
Our study had certain limitations. Firstly, we included only a few specimens collected at a single institution. Secondly, 42% of patients in this cohort had ILD; therefore, there was patient selection bias. However, a strong tendency for antigenicity loss during slide storage was observed in this analysis. We believe that further large-scale studies are warranted to identify all possible candidates for therapy with PD-1 axis inhibitor and to establish optimal pathological processing methods for accurate PD-L1 assessment.
In conclusion, the storage of sectioned NSCLC slides led to the underestimation of PD-L1 TPS. Tissue sections should be stained quickly for evaluation of PD-L1.
Acknowledgements
This study was supported by internal funding from Kobe City Medical Center General Hospital. The Authors would like to thank Masashi Sugawara, Shuji Imoto and Keiko Sakuragawa for their administrative assistance.
Footnotes
Conflicts of Interest
The Authors have no conflicts of interest to disclose.
- Received December 7, 2017.
- Revision received January 15, 2018.
- Accepted January 16, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.