


Abstract
The widespread use of endoscopy and imaging in combination with the continuous update of the staging systems for neuroendocrine tumors has led to an increase in the incidence of small intestinal neuroendocrine tumors (si-NENs) globally. Despite high survival rates, severe complications may occur even in early stages due to the anatomic location of the primary site and the desmoplastic reaction. Surgery plays a central role in the management of patients with si-NENs. Excision of locoregional disease along with extensive lymph node dissection should be performed in fit patients, even in the presence of metastases. Multimodality treatment of liver metastases includes hepatectomy, ablative techniques and liver transplantation. Hormone therapy with somatostatine analogs is of high importance for symptomatic control; special caution should be exercised both pre- and intra-operatively. A multidisciplinary approach is essential in order to provide personalized therapeutics for patients with si-NENs. Clinical research and specialization in this field should be further encouraged.
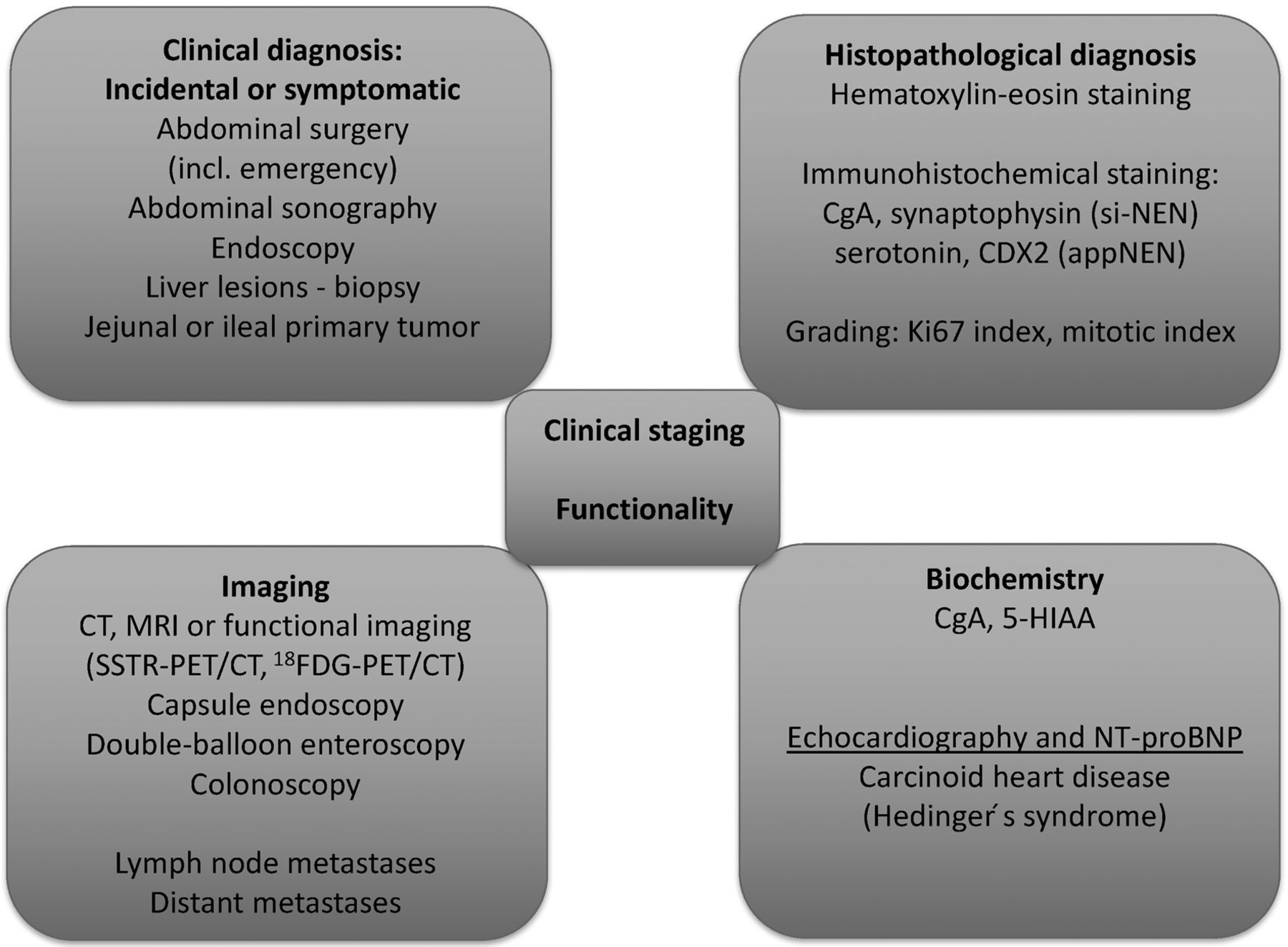
Small intestinal neuroendocrine tumors (si-NENs) are the most common neoplasms of the small intestine and are mainly found in the terminal ileum (1). They are usually focal lesions, less than 2 cm in diameter; however, one-third of cases present with multifocal disease (2). Their incidence has increased from 1.09/100,000 person-years in 1973 to 5.25/100,000 person-years in 2004 (3). This is mainly attributed to medical advances in recent decades, including staging systems, endoscopic examinations, improvement of imaging modalities and pathological examinations of surgical specimens. A diagnostic algorithm for si-NENs is depicted in Figure 1. The current classification of si-NENs is described in Table I.
In a large series of patients with gastroenteropancreatic NENs diagnosed between 1973 and 1997, 44.7% were si-NENs, among which more than 50% were located in the ileum (1, 3). Median age at diagnosis is 66 years and 52% of the patients are males (4). In a recent meta-analysis, ever smoking, and family history of malignancy or colorectal cancer were significantly associated with increased risk of si-NEN (5).
Most patients with si-NENs have prolonged survival due to the low NEN cell proliferative rate and, thus, patients with localized disease have a 5-year overall survival (OS) rate of 70-100%, whereas for those with distant metastases, more common in the liver, it is 35-60% (6). In autopsy studies, the reported incidence of si-NENs is high (8,34/100,000), indicating that their true incidence may be higher than suspected, since many will remain undiagnosed due to lack of clinical manifestations (7).
The mainstay of si-NEN therapeutics is surgery, which may be curative in the case of R0 resection (8). However, in most patients, R0 resection is far from feasible mainly due to advanced stage at diagnosis. In this setting, surgery aims to reduce the disease burden in order to improve survival. Patients with operable disease have better prognosis than those with inoperable, even in advanced stages (9, 10). Approximately 80% of disease-related deaths are due to liver insufficiency and 16% due to bowel obstruction; therefore, surgical intervention may help improve survival and quality of life (11).
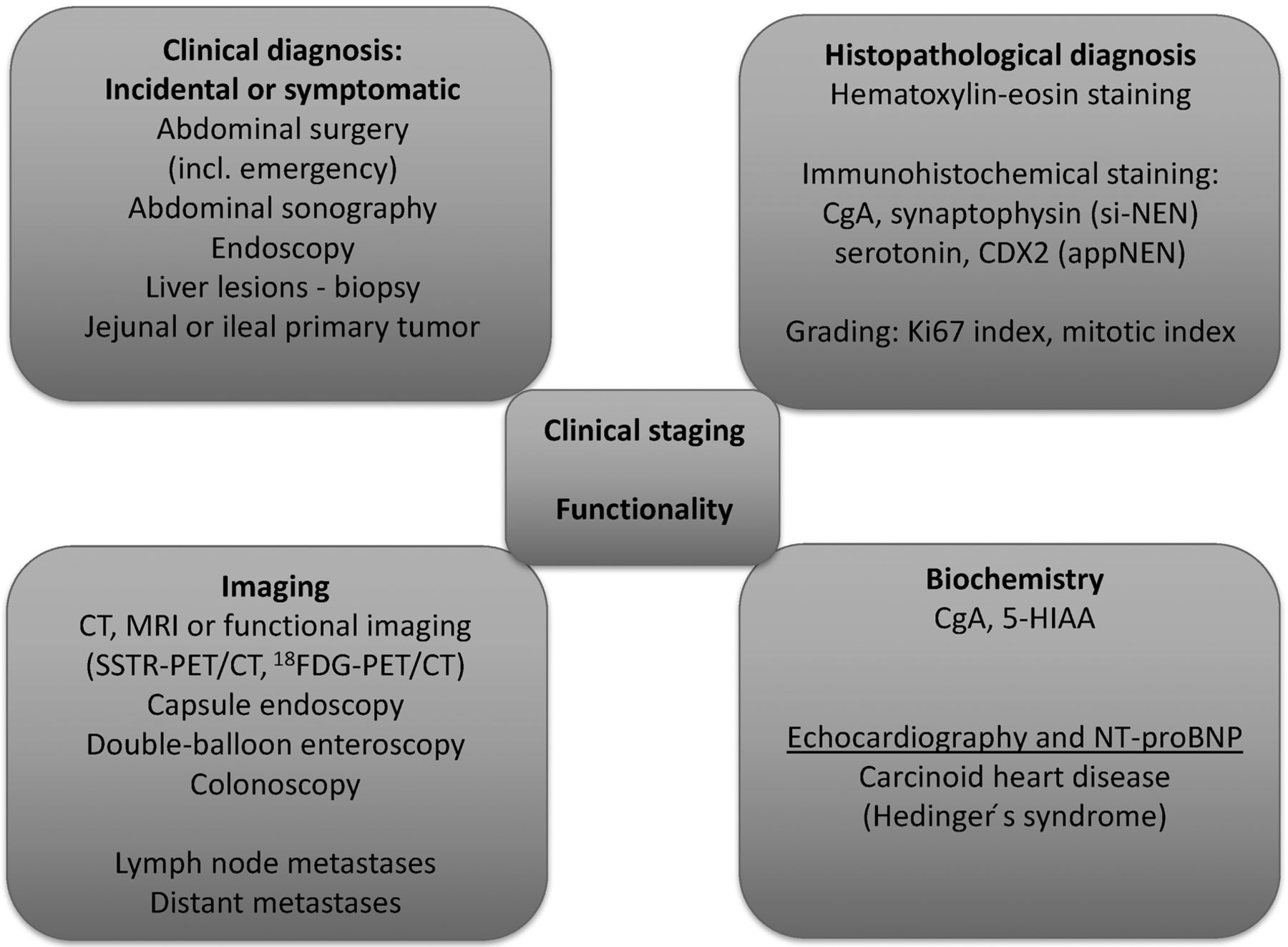
Diagnostic algorithm for small intestinal neuroendocrine tumors. CgA: Chromogranin A; appNEN: neuroendocine tumor of the appendix; 5-HIAA: 5-hydroxyindoleacetic acid; CT: computed tomography; MRI: magnetic resonance imaging; SSTR: somatostatin receptor; PET: positron-emission tomography; 18FDG: 18F-deoxyglucose; NT-proBNP: N-terminal pro B-type natriuretic peptide.
Surgical management is challenging, also taking into consideration that approximately 30% of cases present with multifocal disease and more than 50% (up to 80%) present with metastatic disease at diagnosis (12). For inoperable cases, hormone symptom control and suspension of tumor proliferation should be among the therapeutic aims.
Herein, we review the current knowledge in the surgical management of si-NENs. The principles of surgical treatment are summarized in Table II.
Preoperative Care
Preoperative tests should include computed tomography (CT) or MRI, somatostatin receptor scintigraphy (SRS) or 68gallium positron-emission tomography (PET)/CT, 5-hydroxyindoleacetic acid (5-HIAA) levels in 24-h urine sample, and echocardiogram for assessing the burden due to carcinoid syndrome (10). The main scope of this workup is the prevention of perioperative carcinoid crisis presenting with hyperthermia, shock, arrhythmias, hyper- or hypotension, tachy- or bradycardia, flushing or bronchospasm.
Upon evidence or suspicion of carcinoid syndrome, therapy with somatostatin analogs (SSA), such as octreotide, should start at least 1 day before surgery, continue during the surgical procedures and up to at least 1 day postoperatively; caution should be exercised in the gradual discontinuation (13). This approach applies even for minor surgeries (14). Risk magnitude and the severity of a crisis are difficult to forsee; however, patients with a known uncontrolled syndrome are at a very high risk. There is also a high risk in cases of large tumors that secrete serotonin such as during liver metastasectomy or liver transplantation (14). Prevention remains the best therapeutic strategy in this setting.
Before surgery, any electrolytic disturbances should have been corrected. Preventive administration of octreotide is usually enough for minor surgeries (15). For major surgeries, a preoperative dose of octreotide is followed by a continuous infusion during surgery that should be doubled in the case of carcinoid crisis. Postoperative discontinuation is gradual, with 50% reduction each day (14).
TNM staging system according to the American Joint Committee on Cancer 8th edition, 2017 (23).
Other supportive care is administered as indicated. Intraoperative hypotension not attributable to blood loss, and bronchospasm necessitate the administration of fluid, octreotide and steroids, whereas the use of vasoconstrictors is debatable since they may reinforce serotonin and amine secretion (14).
Locoregional Enterectomy with Lymph Node Dissection
Surgical resection of the primary tumor with locoregional mesenteric lymph node dissection and metastasectomy, if feasible, is the only curative approach (16), although R0 resections have been reported to be feasible in only 20% of cases (17); however, it has been reported that the current rate is even higher (18).
Surgical intervention depends on the primary tumor site: oncological right hemicolectomy for tumors of the terminal ileus, small bowel enterectomies for more proximal si-NENs. Although fewer than 40% of tumors are multifocal, intraoperative inspection and palpation of the whole small bowel is considered of utmost importance (19).
Mesenteric lymph node metastases are usually present and aggravate the prognosis. Systemic lymph node dissection along with enterectomy may improve survival and rate of complications (20). Optimal lymphadenectomy may be really challenging, especially when there is coexistence of mesenteric fibrosis or large lymph node metastases of the superior mesenteric artery (SMA) (21). Optimal enterectomy with optimal lymphadenectomy is vital for improving survival and preventing recurrence (6, 20, 22). Therefore, it is advisable that such operations be conducted at specialized centers with relevant expertise treating a large number of patients.
Even in the presence of metastatic disease, patients with si-NEN should undergo optimal surgery with lymphadenectomy in order to prevent ischemia, obstruction, and perforation. Dissection of at least eight (10, 14, 20) or 12 (23) lymph nodes has a positive impact on survival. A recent meta-analysis showed that among patients with metastatic disease, palliative resection of the primary tumor conferred a survival benefit (24).
In the presence of liver metastases, locoregional disease control gives the opportunity to focus on the treatment of hepatic disease, whereas it improves symptoms and, thus, quality of life (6, 25).
Lymph node skip metastases have been reported and systematic and extended lymph node dissection in the retropancreatic area may be necessary in order to prevent logoregional recurrence (26).
Surgical Procedure
Intraoperative exploration with a radioguided detector has shown promising results in guiding resection of the primary tumor and metastatic lymph nodes. However, technique standardization and specific guidelines for its role are still under debate (27). Whole small bowel (from Treitz ligand to the ileocecal valve) inspection and palpation with both hands is of great importance for pinpointing otherwise undetectable tumors (10, 18). Preoperative CT- or MRI- angiography may be useful in determining the tumor and the lymph nodes sites in relation to the vessels, so that the optimal surgical resection is feasible, with adequate length of small bowel left behind (at least three jejunal arteries) in order to prevent short bowel syndrome (28, 29). Residual metastatic lymph node disease may result in mesenteric ischemia or recurrent obstructive episodes, therefore a thorough investigation and dissection of malignant lymph nodes is important (14). Concurrent cholecystectomy is also preferable because the adjuvant treatment with SSAs and, possibly, chemoembolization may cause cholestasis, with a high risk of complications such as necrotic cholecystitis (18, 29).
The ileocecal valve should be preserved, if it is oncologically acceptable, especially in patients with carcinoid syndrome in whom the lack of ileoceccal valve reduces the postoperative quality of life. It is estimated that up to 40% of cases may retain the ileocecal valve (14). Boudreaux et al. conducted several studies assessing the role of stains such as isosulfan blue or methylene blue in the mapping of lymphatic drainage (9, 14, 30). If the lymphatic vessels of the ileocecal valve are colored, then there is a high risk of metastasis and right hemicolectomy should be performed. This is usually the case in those with tumors exceeding 1 cm and in the presence of bulky mesenteric lymph nodes (14). Otherwise, the preservation of the ileocecal valve is suggested. Lymphatic mapping may also provide useful data regarding the link between a primary tumor and multiple primary small bowel tumors (30). This may provide a basis for the monoclonal origin of synchronous si-NENs by serial lymphatic interstitial spread caused by the obstruction of the central lymphatic drainage at the mesentery root due to the tumor and desmoplastic fibrosis (30). The same rationale may be applicable for explaining local recurrence. In this context, Boudreaux et al. (14) have proposed colored lymphatic vessels as delineating a new resection margin, instead of the rather arbitrary 5 cm. Such an approach has resulted in the improvement of survival, with 5- and 10-year OS reaching 87% and 77%, respectively, compared to 54% and 30%, respectively (9). However, this method extends the resection of small bowel to 7-10 cm, which may have aggravated diarrhea postoperatively. Preservation of the ileocecal valve may be beneficial in this setting (31).
Principles of surgical treatment.
Mesenteric Lymph Node Metastases and Desmoplastic Fibrosis
Si-NENs tend to metastasize to the lymph nodes of the mesentery root and present with bulky disease. These lymph node masses may enlarge and secrete hormones and result in desmoplastic reaction and peritoneal fibrosis. Consequently, mesenteric vessels may be encapsulated and develop thrombosis; cisterna chyli, pancreas and duodenum may also be encapsulated, with subsequent abdominal pain after meals and possibly duodenal or small bowel obstruction. This clinical presentation may result in abstinence from food, weight loss and malnutrition. SMA encapsulation result in collaterals that predispose for lower gastrointestinal hemorrhage and may provoke small bowel ischemia or even necrosis. Cisterna chyli rupture is possible and may result in bile ascites that necessitates surgical intervention. Furthermore, desmoplastic reaction may result in retroperitoneal fibrosis, ureteral obstruction and hydronephrosis (32).
In this context, resection of mesenteric lymph nodes is considered vital. A study has classified lymph node metastases into four stages in order to facilitate the preoperative surgery plan. Only stage IV metastases were considered inoperable, due to the fact that optimal lymphadenectomy would be dangerous in terms of vascularization of the remaining bowel (28).
In cases of SMA stenosis or thrombosis, transjugular intrahepatic portosystemic shunt at the level of the mass is a viable option (33). This approach was associated with obstruction resolution in 93% of cases and enteric ischemia improvement in 83% (34).
Conclusively, approximately 80-88% of patients with si-NENs present with lymph node metastases at diagnosis (6, 22). Systematic lymphadenectomy with dissection of at least eight lymph nodes is important and confers a survival benefit (10). Some authors suggest 12 lymph nodes as the cut-off value (28), still others believe that disease recurrence is not predominantly influenced by lymphatic spread but by other factors such as multifocal disease, which should also be taken into consideration (22). Optimal lymphadenectomy has not yet been standardized and is rather debatable (10). Lymphadenectomy is not associated with the length of surgical specimen (28). Furthermore, the ‘pizza pie’ approach should be abandoned and the inverse approach should become standard (28). Lymphadenectomy should precede enterectomy with possible ileoceccal valve preservation (10, 18, 28, 35). R0 resection of both primary tumor and lymph node metastases is feasible in 80% of cases (10, 18, 19, 36). Only in a minority of patients with bulky mesenteric masses is optimal debulking not feasible (36). However, surgical intervention may alleviate symptoms (36).
Regarding a laparoscopic approach, it may be considered only in cases with preoperative evidence of localized disease and absence of tumor masses (37). Laparotomy is the standard of care since it enables the exploration of the peritoneal cavity and mesenteric vessels, as well as the palpation of the small bowel (17, 18).
Liver Metastases
si-NENs are most frequently metastatic at diagnosis compared to other gastrointestinal NENs (38-40). Excluding lymph nodes, the liver is the primary site of metastatic disease; up to one half of patients with primary tumor exceeding 2 cm present with hepatic metastases.
Liver resection. There are multiple approaches in the therapeutics of liver metastases including hepatectomy, thermal destruction [radiofrequency ablation (RFA), microwave ablation (MWA)], arterial embolism (TAE), chemoembolism (TACE), selective internal radiation therapy (SIRT), targeted therapy [peptide receptor radionuclide therapy (PRRT)] and liver transplantation. In patients with grade 1/2 si-NENs, hepatectomy is the standard of care in fit patients; however, its role is debatable in those with grade 3 tumors (41). Following surgery, 5-year OS is 60-80%. Multidisciplinary consensus meetings are deemed necessary in order to formulate a personalized treatment approach for each patient (16).
According to current European Neuroendocrine Tumor Society guidelines (42), resection of liver metastases should be considered when R0 resection of grade 1/2 metastatic tumor is feasible with acceptable predicted morbidity (~30%) and mortality <5%, in the absence of right heart failure or extra-abdominal metastases and diffuse peritoneal carcinomatosis; however, the latter is debatable in terms of cytoreductive surgery (9, 16, 43).
The type of liver resection (metastasectomy, partial hepatectomy, liver transplantation) depends on various factors including tumor biology, number, size and site of lesions, performance status, and predicted remaining liver function (44). Denucleation or parenchymal-sparing hepatectomy is currently the most preferable approach for many surgeons (45, 46). Combining surgery and RFA or MWA may be a feasible approach for preserving postoperative liver function. It has been supported that >70% or even 90% of the metastatic burden in liver should be resected for obtaining clinical benefit (36). Recent studies have shown that debulking surgery with a cut-off at 70% has resulted in 5-year OS of 75% (9, 36). Thus, it may be a feasible option in patients with advanced-staged disease.
In contrast to liver metastases from other types of cancer, surgical intervention in metastatic liver disease from NENs does not necessitate an R0 resection, although this would be the optimal approach (46, 47). The rationale behind this approach is that these types of metastases are not invasive, meaning that denucleation is an acceptable approach when R0 resection is not possible. Indeed, major cytoreductive surgery has shown similar outcomes with R0 resections (11).
Retrospective studies between 1990 and 2001 included a small number of patients (median=19, range=4-34), all of whom underwent complete resections. Symptom control was 88-100% and 3- and 5-year OS rates were encouraging (48). Early data indicating that cytoreductive surgery of liver metastases by at least 90% could improve hormonal symptoms were reported by McEntee et al. in 1990 (49). Their results were confirmed by Sarmiento et al. in 2003 (50) in their study of 170 patients with liver metastases from si-NENs, pancreatic NENs, and NENs of unknown primary site. Among the patients with functional tumors, 96% had symptom control, and the median time to recurrence of metastasis was 45.5 months; 5- and 10-year OS were 61% and 35%, respectively, and median OS was 81 months, whereas among historical controls with no surgical intervention, the median OS was 24-48 months. Thus, surgical intervention significantly improved OS and is an acceptable approach (47).
A more recent study in 2010 by Glazer et al. showed 24% morbidity and no mortality. A total of 182 patients with si-NEN or pancreatic NENs with hepatic metastases were included; 140 underwent surgical resection and several RFA. Overall, 47% presented with disease recurrence and 5- and 10-year OS was 77% and 50%, respectively. Median OS was 9.6 years. Interestingly, positive (R1 and R2) resection margins were not associated with inferior OS (51).
Mayo et al. published the results of a multicenter study including 339 patients (52). All patients had metastatic liver disease from pancreatic NENs (40%) and si-NENs (25%): 70% underwent hepatectomy, 3% RFA, and 19% both there was no prespecified percentage of cytoreductive surgery. Overall 94% of the patients had disease recurrence at 5 years, 5- and 10-year OS was 74% and 51%, respectively, whereas median survival was 125 months. In the multivariate analysis, synchronous liver metastasis, non-functional tumors and extrahepatic disease were significantly associated with poor prognosis. The median OS for patients with extrahepatic disease was 85 months, whereas for those with non-functional tumors and R2 resection it was more than 84 months (52).
In a study by Graff-Baker et al. including 52 patients with si-NEN, a cut-off of 70% cytoreductive surgery was applied for eligibility. Positive resection margin and resection of extrahepatic disease were permitted. The median time to progression of liver metastases was 71.6 months. In the multivariate analysis, only age was significantly associated with time to progression. Disease-specific 5-year survival was 90%, while all deaths were attributed to liver failure (53).
Overall, the reported morbidity of hepatectomy in these patients was 16-24%. Most common complications include bleeding, biliary leakage, intra-abdominal abscesses and pleural effusion (50).
Intrahepatic localization of metastases may be classified into three distinct patterns (54): i. Type I: One metastasis irrespective of size (20-25%); R0 resection confers the best survival rates (41). ii. Type II: One metastasis with accompanying small lesions in both sides of the liver (10-15%); surgical approach is debatable and multiple operations may be needed (16, 40, 55). iii. Type III: Bilateral metastases irrespective of number or size. Surgery is only rarely indicated (16).
Eligibility for surgical intervention should be assessed according to the following criteria (10, 54): iv. Grade 1/2 tumors. v. Grade 3 tumors should not be treated by upfront surgery due to high risk of recurrence. vi. Negative preoperative assessment of non-operable extrahepatic disease (68gallium PET/CT). vii. Type I or II, as described above. viii. R0 resection, or R1/R2 in terms of cytoreductive surgery. ix. Negative assessment for advanced carcinoid cardiac disease. x. Specialized surgical center.
In those with metastatic si-NENs, R0/R1 resection of the primary tumor, as well as resection of metastatic lymph nodes and distant metastases seem to provide both survival and quality of life benefit. 5- and 10- year OS rates were 46-86% and 35-79%, respectively (51).
Systematic reviews have not documented a clear survival benefit in patients treated with surgery compared with those treated with other therapeutic modalities (56). This is mainly due to the lack of randomized controlled trials in the field and the selection bias that is inherent in many of the published studies. However, R0/R1/R2 surgical intervention for liver metastases from grade 1/2 si-NENs remains the sole option with curative intent (40).
Neither neoadjuvant nor adjuvant chemotherapy improve outcomes in metastatic liver disease (57). There are small series indicating that immunotherapy or PRRT, or both, may improve the possibility of achieving R0 resection (58).
Locoregional Treatment
In view of the lack of large randomized trials, the locoregional treatment approach should be on an individualized basis according to tumor and patient characteristics. Locoregional modalities should be introduced early in the treatment algorithm, but after SSA treatment for functional tumors due to the risk of carcinoid crisis (59).
RFA and other modalities of locoregional destruction. Currently available thermal destruction techniques include RFA, MWA, laser-induced thermotherapy, cryotherapy and irreversible electroporation (60).
RFA may be used either as monotherapy or in combination with hepatectomy. It is very efficient in symptom control and locoregional metastatic control. It may be performed intradermal under US or CT guidance or laparoscopically; thus it may be applied in patients ineligible for hepatectomy (13).
However, there are several limitations in RFA use (61). Only a limited number of lesions (<5), of limited size (maximum diameter <5 cm) may be destroyed. Furthermore, these lesions should not be close to vital structures such as hepatic veins and porta hepatis. Although RFA may be repeated in a single metastasis, size >5 cm renders RFA inapplicable (42). In patients ineligible for surgical excision, open or laparoscopic RFA may be performed by an interventional radiologist in order to detect any multifocal disease. Morbidity in these cases is acceptable (4-5%), including bleeding, infections, and liver abscess.
The great value of this method is that it enables the treatment of liver metastases, in combination with surgery, that otherwise would be inoperable. RFA may be performed supplementary to surgery in order to destroy multifocal disease or limit the extent of a hepatectomy and, thus, the postoperative risk of liver failure (52).
RFA results in substantial symptom control in 70-80% of patients (48). Improvement in biomarkers such as 24 h urine 5-HIAA and serum chromogranin A occurs in 65-75% of the patients (62). Among patients treated with RFA exclusively, median OS from the time of first RFA was 3.9 years and 5-year OS was 53%, whereas 22% had local recurrence at 30 months (63). Most centers around the world recommend RFA because of its efficacy in tumor control and its widespread availability (64).
More recently, the introduction of MWA (65) has enabled better thermal destruction for lesions of around 5 cm in diameter, and it may result in more durable results compared to RFA (66). Furthermore, the introduction of irreversible electroporation even enables targeted thermal destruction close to vital structures, without sacrificing them (60). Laser-induced thermotherapy is another approach that may be applicable to lesions near vital structures, but the available data are rather immature (67). Cryotherapy is not currently recommended due to the scarcity of data (68); a study including 13 patients with gastrointestinal NENs indicated that 12 patients had complete tumor destruction, two had recurrent tumors and 12 were alive at 12 months of follow-up (69).
Intra-arterial liver treatment (TACE, TAE, SIRT). Intra-arterial modalities, including TAE, TACE and SIRT (drug-eluting bead TACE) are indicated in patients ineligible for surgery and can be performed repeatedly. Their rationale is that liver metastases from si-NENs usually have rich vasculature originating from the hepatic artery (70).
TAE and TACE may result in reduction of tumor size and symptom control in more than 50% (53-100%) of patients for 10-55 months and radiological response in 35-74% for 6-63 months (71). To date, there are no data indicating TACE superiority compared to RFA (42). The most widely used chemotherapeutic drugs in TACE are doxorubicin and streptozotocin (71).
TACE should be conducted at centers with expertise due to the associated morbidity. Mortality ranges between 0 and 5.6% (0-3.3% at specialized centers) whereas morbidity ranges between 28 and 90% (66). There is also a relative contradiction in portal vein thrombosis and liver failure. Other relative contradictions include Whipple procedure and hepatopulmonary shunts. Among the major complications are necrosis of choledochal cyst (hence prophylactic cholecystectomy is recommended), hepatorenal syndrome, pancreatitis, liver abscess and hepatic artery aneurysm (70).
SIRT (drug-eluting bead TACE) with 90Y-tetra-azacyclododecane tetra-acetic acid lanreotide (with or without embolism) is effective in patients with large hepatic metastases with SRS positivity according to a multicenter study (72): 22.7% of the patients had stable disease, 60% partial response, 27% complete response and 4.9% had progressive disease. Long-term outcomes following SIRT resulted in response in 62.7%, disease stabilization in 32.5%, and 1-, 2- and 3-year OS at 72.5%, 62.5% and 45%, respectively (40).
An international multicenter trial showed that safety and response rates were similar for SIRT and TACE at 6 months (73), whereas at 12 months, the SIRT-treated group had significantly lower response rates compared to the TACE-treated group (46% vs. 66%). Toxicities include fatigue and nausea (<10%), as well as pulmonary shunts, gastritis, duodenal ulcer, and liver fibrosis. SIRT-mediated liver radiotherapy may result in liver lobe atrophy and contralateral hypertrophy. Thus it may be used for partial volume effect and down-staging (74). Although promising, more data are needed in order to determine the role of SIRT in therapeutics of gastrointestinal NENs (16).
Liver transplantation. Liver transplantation is an alternative option for patients with unresectable metastases (75). Only 0.2-0.3% of all liver transplantations are conducted due to metastatic liver disease from NENs according to the United Network for Organ Sharing database and the European Liver Transplant Registry (76, 77). Patients should be selected on a rigorous basis (77). Eligibility criteria according to Mazzaferro et al. (78) include: i. Previous R0 resection of primary tumor. ii. Histological diagnosis of well-differentiated si-NEN (grade 1/2, Ki-67 <10%). iii. Portal vein should be the venous drainage of the primary tumor. iv. Absence or complete resection of extrahepatic lesions. v. Liver metastatic disease in <50% of total liver volume. vi. Stable disease under treatment for at least 6 months before transplantation. vii. Age <55 years (relative contraindication).
European Neuroendocrine Tumor Society Criteria are similar to those of Pavel et al. (70) and include: i. Transplantation mortality <10%. ii. Absence of extrahepatic disease by PET/CT. iii. Previous resection of primary tumor. iv. Grade 1/2 NET. v. Age <50 years. vi. Low Ki-67. Explorative laparotomy or laparoscopy may be necessary for detecting peritoneal disease before transplantation. Failure of primary tumor detection should not be considered as absolute contraindication (79).
Patients with small cell tumors, grade 3 NETs or neuroendocrine carcinomas, with major comorbidities, NETs that do not drain into portal vein, extrahepatic metastases (excluding perihilar lymph nodes) and carcinoid cardiac disease (40) should be excluded. Only when the eligibility criteria are metastatic is the patient undergoing liver transplantation expected to have better OS benefit compared to those treated with conservative methods (79). However, these criteria are currently under validation and they are subject to change in the light of new data from future prospective studies (40).
Liver transplantation for NETs is associated with a 5-year OS comparable or better than hepatocellular carcinoma (76) and ranges between 36-90%, with disease-free survival at 30-77% (40), whereas in multicenter studies, the 5-year OS was 47-49% (76, 80), but significantly lower (12%) in the subgroup with adverse prognostic features such as invasion of large vessels and greater extent of extrahepatic disease (80). In another study that applied strict eligibility criteria (78), 5- and 10-year OS were 97.2% and 50.9%, respectively, whereas other treatment modalities resulted in rates of 88.8% and 22.4%, respectively (p<0.001). The survival benefit from transplantation was 6.82 months at 5 years (p=0.019) and 38.49 months at 10 years (p<0.001) (78).
In conclusion, orthotopic or living donor liver transplantation is a viable option only when eligibility criteria are strictly addressed at specialized centers with a multidisciplinary treatment approach (40).
Diffuse Peritoneal Carcinomatosis (PC)
Approximately 17% (5-33%) of patients with si-NENs have miliary spread in the peritoneal cavity. Peritoneal cavity is the third most common site of metastasis following lymph nodes and liver (81). The reported incidence of PC is approximately 13.6%. Signs and symptoms of bowel obstruction or ascites may indicate PC. Several patients present with ‘frozen abdomen’, especially in the pelvis, despite the absence of extensive liver metastatic disease (32). The presence of bulky disease in the peritoneal cavity is an ominous prognostic characteristic (81).
Surgical intervention in PC due to NETs remains debatable (81, 82). However, it may be necessary for preventing serious complications such as bowel obstruction, mesenteric fibrosis, gastrointestinal bleeding, and portal vein hypertension (55). Following a surgical intervention, the preferred reporting system is the completeness of cytoreduction (CCR) that reflects the residual disease (83). CCR is assessed as follows (84): CCR-0: No macroscopically evident residual lesions. CCR-1: Microscopically evident residual lesions <2.5 mm. CCR-2: Residual lesions between 2.5 mm and 2.5 cm. CCR-3: Residual lesions >2.5 cm. CCR is the main prognostic factor for OS after surgery and is independent of the initial exten of PC (83). Thus, surgery should be opted for patients with anticipated low CCR score after the operation including, those with peritoneal carcinomatosis index <20, or abdominal gravity peritoneal carcinomatosis score (GPS)-A or GPS-B low (81).
Hyperthermic intraperitoneal chemotherapy (HIPEC) may improve survival rates by eradicating small PC lesions. HIPEC is applied after an extended surgical intervention including macroscopic disease, excision of the peritoneum, omentum, ovaries, uterine etc. The main limitation of HIPEC in this setting is that chemotherapy is used against tumors with a low proliferative rate (85). Added risk of morbidity and mortality should be also taken into consideration when HIPEC is considered simultaneously with another major surgery (81).
Asymptomatic Primary Tumor
Due to their small size and the submucosal site, si-NENs are rarely diagnosed before symptoms occur. In this case, an aggressive approach is recommended, especially in those with a family history of si-NENs (86). Lack of symptomatic disease is by no means a contradiction for surgery (30). Early surgical intervention may prevent an emergency surgery that would be accompanied by high morbidity and mortality risk (9, 30). More than 80% of these patients have multifocal disease and one-third of them have stage III disease. Almost one half of those with si-NENs under 10 mm have lymph node metastases (35). In this context, si-NENs should be treated aggressively with surgical excision and lymphadenectomy (10). Among patients with asymptomatic si-NENs with distant metastases, a recent study demonstrated no survival benefit among those that underwent prophylactic locoregional surgery compared to those that underwent delayed surgery or no surgery according to clinical indications. Randomized clinical trials are needed in order to elucidate this field (6).
Resection of primary asymptomatic tumor in the synchronous presence of unresectable liver metastases is debatable. The rationale of this approach is that resecting the primary tumor eliminates the burden and the potential complications that may arise and could prove fatal in the future. Unfortunately, there has been no randomized study, although unresectable hepatic metastases range between 15-80% of gastrointestinal NEN cases (40). In a meta-analysis, Capurso et al. showed that such an approach confers OS benefit, with OS reaching 75-139 months versus 50-88 months for a conservative approach (87). Prospective studies should be conducted in order to provide more rigorous data in this field.
Conclusion
As in all gastroenteropancreatic NENs, si-NEN incidence is rising steadily. Disease symptoms depend on stage and anatomical site. Carcinoid syndrome is more frequent among patients with advanced liver metastases. Treatment of logoregional disease should include surgery, while a surgical approach is also applicable to distant metastases and confers a survival benefit. Lifelong follow-up is of high importance, especially for young patients. There is a intense scientific interest in this field and the management of patients with si-NENs is surely going to be further improved in the oncoming years.
Footnotes
This article is freely accessible online.
- Received December 29, 2017.
- Revision received January 24, 2018.
- Accepted January 30, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}