


Abstract
Background/Aim: Ovarian cancer (OC) has a high mortality rate and usually presents late in advanced stage, which poses challenges to management. Better understanding of the disease biology and application of radical surgery (RS) to achieve no visible residual tumor, alongside with chemotherapy, may lead to longer survival amongst these patients. Our purpose was to examine the demographic characteristics, surgical morbidity and outcomes of patients undergoing RS for OC. Materials and Methods: A retrospective cohort study of women undertaking surgery for OC between February 2014 and September 2016 in Aberdeen Royal Infirmary. Results: A total of 121 women had surgery for OC of whom 78 (64.5%) were stage II and above. Of these, 40 (51.3%) women had primary and 38 (48.7%) had interval debulking surgery with 42 (53.8%) having radical surgery. The most common procedures that were performed as part of RS included rectosigmoid resection (n=20, 47.6%), small bowel resection (n=10, 23.8%), splenectomy (n=9, 21.4%). Morbidity outcomes included blood loss >1.5 lt. (n=14, 33.3%), hospitalization >7days (n=31, 73.8%), sepsis (n=8, 19%). There was no short-term mortality. Debulking outcomes were: no macroscopic residual disease (n=36, 85.7%), ≤10 mm disease (n=2, 4.8%), and ≥10 mm disease (n=3, 7.1%). Conclusion: Our findings support the practise where RS for OC can be offered to selected patients, with good surgery outcomes and low morbidity rates.
Ovarian cancer (OC) is the second commonest gynecological cancer with an overall incidence of 1.4%, associated with high mortality rate (1, 2). Eighty percent % of cases present in advanced stage with good response at initial treatment (1) but with a high recurrence rate of 75% and 5-year survival of 35% (1).
The key post-operative prognostic factor for women undergoing debulking surgery for OC is residual disease size after surgery (1, 3, 4). Better understanding of the disease biology with implementation of radical surgery to achieve no visible residual tumor, alongside with chemotherapy, has led to longer survival (2). The “standard treatment” (5) consists of primary debulking surgery (PDS) when possible, a procedure that includes hysterectomy, bilateral salpingo-ophorectomy, total omentectomy followed by platinum-based chemotherapy (6-9). Radical surgery (RS) includes the additional steps of colonic resection, splenectomy, partial pancreatectomy, resection of peritoneal or diaphragmatic resection, partial gastrectomy (5).
Complete cytoreduction is defined as the removal of all grossly-evident tumor to microscopic residuum (no visible residual), whereas optimal surgical cytoreduction is defined as residual disease of ≤10 mm and sub-optimal surgical cytoreduction described as residual disease ≥10 mm (2, 10).
Individualization of prognosis is difficult (1). The morbidity rate of debulking surgery is high which can affect the prognosis and patient's quality of life (QoL) (6). Overall, prognosis is related to tumor variables (stage of disease, histology, and grade), patient variables (age, performance status, nutritional status), pre-operative laboratory values, surgical expertise and result of surgical treatment (1, 4).
Current aim is to improve current prognostic models for women undergoing debulking surgery for OC (3). Studies reported that the greater the surgical radicality the higher the rate of intra-operative and peri-operative complications such as bleeding, infection and long-term hospitalization, which inevitably lead to reduction of patient's QoL (1-3, 10). Therefore, is questionable whether the benefits in overall survival after RS are substantial enough to compensate for the surgical risks. Hence, in order to maximize the benefit and minimize the risks, surgery must be used judiciously and with careful patient selection and treatment planning. It is also logical to suggest that high-risk patients for RS may benefit from alternative treatment methods such as neo-adjuvant chemotherapy. Thus, one of the most vital questions is to decide whether PDS or interval debulking surgery (IDS) is the best option with the aim of leaving no visible residual tumor at surgery with acceptable morbidity.
Aberdeen Royal Infirmary (ARI) is the gynecological oncology centre of Northeast Scotland covering a population of 1.2 million. In Scotland, ARI was one of the first hospitals which implemented RS for ovarian cancer. The main purpose of our study is to examine the clinical and demographic characteristics, surgical morbidity and outcomes of patients undergoing RS for OC.
Materials and Methods
Permission to collect clinical data was given by the National Health Service Grampian Clinical Effectiveness Team (Quality, Governance and Risk Unit, 19th July 2017, reference number 3790). One of the major strengths of Scottish health data is the ability to perform vigorous data linkage in a national population, using Community Health Index (11, 12). This allows for reliable population based and long-term follow up studies (12). Informed consent was not obtained from the patients due to the retrospective type of our study.
The study population included a retrospective cohort of all women ≥18 years of age diagnosed with OC who had debulking surgery between February 2014 and September 2016 in ARI.
All the patients underwent computed tomography scanning (with intravenous contrast when possible) to assess extent of disease and plan the type of radical surgery. Final decision and patient selection for debulking surgery was made after multidisciplinary team (MDT) discussion. Exclusion criteria for PDS included diffuse peritoneal, enteric and mesenteric disease or very poor patient's performance status. When PDS was not feasible, neo-adjuvant chemotherapy was given after histological confirmation of the diagnosis, followed by IDS when surgery thought to be beneficial. Selected cases had laparoscopic assessment shortly before planned surgery. Patients with borderline ovarian tumors were excluded in the study cohort.
Patients had a full staging procedure by gynecological oncologists, with colorectal and hepatobiliary surgeons input when RS was performed. Antithrombotic prophylaxis and antibiotics were administered to all patients. Final decision about surgical radicality was undertaken during surgery.
Based on the literature, we examined potential predictors of survival for OC, type and extent of surgery, additional concurrent procedures, and common peri-/post-operative complications (1, 3). Patients were classified based on age at surgery into groups: <50 years of age, 50-59 years, 60-69 years and 70 years. Race was categorized as white, black, Asian or unknown. Body mass index (BMI) corded as normal (<25 kg/m2), overweight (25-29.9 kg/m2), obese (>30 kg/m2). World Health Organization (WHO) performance status (0, 1, 2, 3), pre-operative albumin (<35 mg/dl, 35-45 mg/dl, and >45 mg/dl), and serum CA-125 at the time of diagnosis were also recorded for each patient. The presence of a number of pre-operative medical comorbidities including diabetes mellitus, tobacco use, chronic obstructive pulmonary disease (COPD), and hypertension were also noted for each patient. Every patient had a detailed pre-assessment and anaesthetic review.

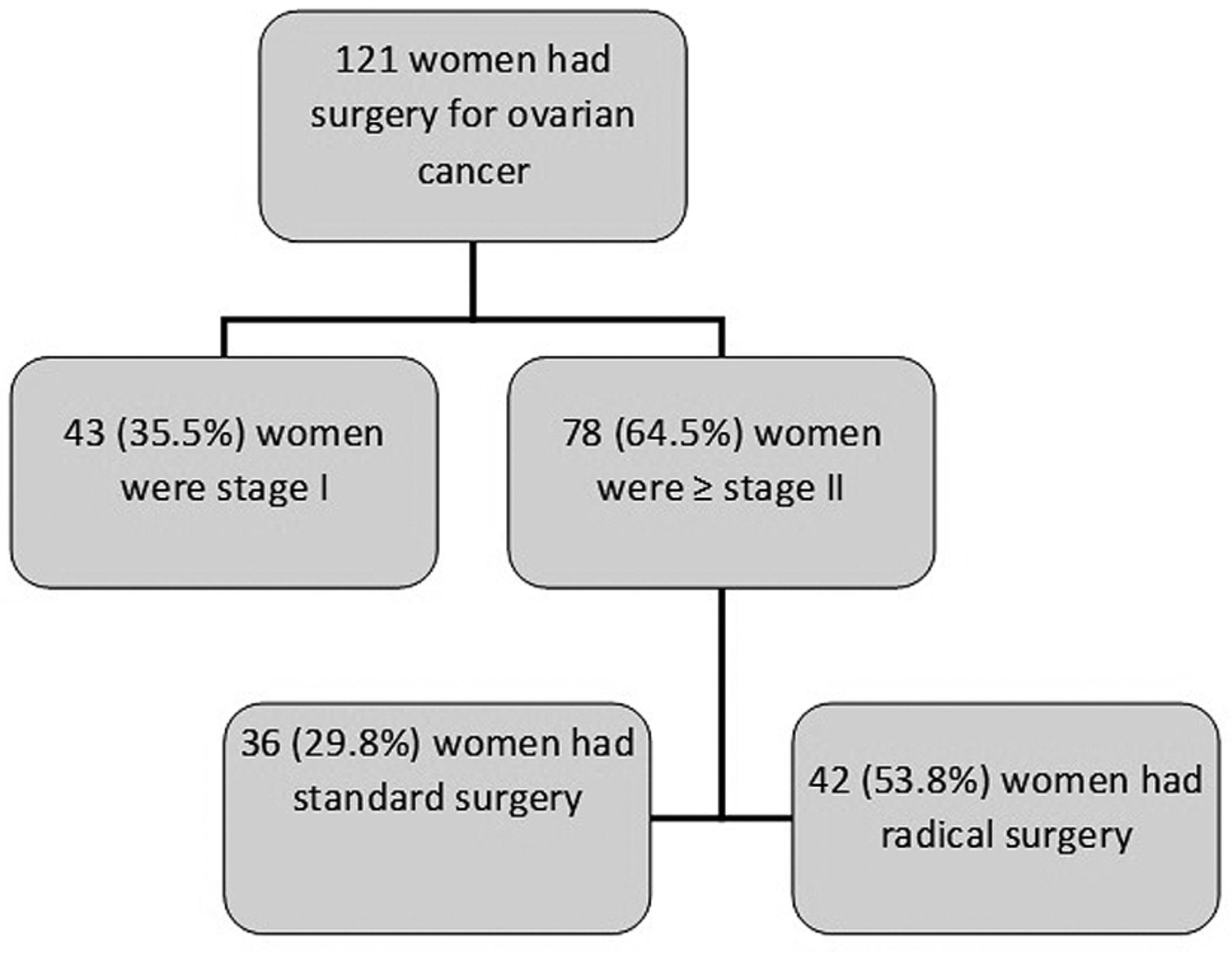
Study group flow chart.
PDS or IDS was determined and concurrent procedures defining RS included lymphadenectomy (pelvic or para-aortic), small bowel resection, rectosigmoid resection, total colectomy, abdominal peritonectomy, diaphragmatic stripping, splenectomy, partial pancreatectomy and liver resection. The residual tumor after surgery was divided as complete, optimal, and sub-optimal.
The primary outcomes of the study were peri-operative morbidity and mortality. Any complication was recorded if the patient was noted to have any of the following: sepsis, shock, pulmonary embolism, wound complications (including superficial or deep surgical site infection or an organ space surgical site infection), re-operation, prolonged length of stay (hospitalization after surgery of >7 days) and mortality within 30 days.
Frequency tables are used to present the results for categorical variables. Quantitative Continuous variables are presented as mean and standard deviation (mean±SD) and median value. Kruskal-Wallis test is used for comparison between continuous and categorical variables. All comparisons are two sided and the statistical significance p level was set to 0.05. For the statistical analysis, programming software R (version 3.3.1) was used.
Results
A total of 121 women had surgery for OC in ARI during the allocated period. From these, 78 (64.5%) women were stage II and above. Of these, 42 (53.8%) women needed RS as described above to achieve complete debulking (Figure 1). Demographic and clinical characteristics of the study cohort by stage are presented in Table I. Mean and median level of Ca125 (U/ml) per ovarian cancer histologic type at the time of diagnosis of the patients who had debulking surgery are described in Table II, with statistically significant difference between the different histologic types, p=0.045.
Demographic and clinical characteristics of the study population.
Concurrent procedures, peri-operative outcomes and complications of the study population who had RS are described in Table III. The most common concurrent procedure was rectosigmoid resection (n=20, 47.6%). Most, women had blood loss more than 1.500 ml (n=14, 33.3%). Twenty-one (50%) women were admitted to High Dependency Unit (HDU) immediately after their surgery and 31 (73.8%) women had prolonged hospitalization >7 days.
Mean and median level of Ca125 (U/ml) per ovarian cancer histologic type at the time of diagnosis of the patients who had debulking surgery.
Type of surgery and outcomes of the study population who had surgery for stage II, III & IV are described in Table IV. In our study group, there was no short-term mortality (death within 30 days).
Discussion
RS for OC is one of the most challenging procedures in gynecologic oncology surgery. The best results in terms of overall and progression-free survival are observed in patients who are completely debulked prior to chemotherapy (1, 2, 7). It has been shown that there is an increased resistance of cancerous cells to platinum-based chemotherapy after longer periods of exposure by the creation of clones of chemotherapy resistant cells (2). Hence, that probably explains why women with PDS show better survival rates than those with IDS (2, 7, 13). Thus, future efforts in the treatment of advanced stage OC might be directed in improving procedures to increase the rate of complete cytoreduction (2). On the contrary, results from one large randomized study showed no difference in survival between the PDS and IDS (14). There seems to be little benefit from surgery unless cytoreduction to below 1cm is achieved (14).
The rate of complete debulking was 78.2% for the total study group and 85.7% for the women who had radical surgery, which meets the rate of Quality Performance Indicators in Scotland (15). Probably, this is related to careful case selection with all parameters taken into consideration, after MDT input and multi-disciplinary surgical input from the colorectal and hepatobiliary team. Extensive counselling for surgery pre-operatively was done by the primary surgeon with anesthetic input and final decision for upfront surgery or not was based on patients' performance status, morbidity and probable tumor resectability.
Concurrent procedures, peri-operative outcomes and complications of the study population who had radical surgery for stage II, III & IV.
In our study group from the patients who had debulking surgery for advanced stage OC, we have had almost an equal number of PDS (n=40, 51.3%) and IDS (n=38, 48.7%) with no difference in surgical debulking outcomes between the 2 groups, similar to CHORUS and EORTC studies (13, 14), though our numbers are small. From the women who had radical surgery, 38.1% (n=16) had PDS and 61.39% (n=26) had IDS. Chiva et al. showed that complete cytoreduction following IDS has an inferior outcome in terms of median survival than PDS of almost 2 years (2). Despite the higher rate of complete resection, IDS apparently fail to improve the survival figures obtained by PDS (2). On the contrary, the results from the CHORUS study failed to show any significant benefit of PDS over IDS with similar overall survival outcomes. In addition, morbidity and mortality were significantly lower in IDS group (14).
Type of surgery and outcomes of the study population who had surgery for stage II, III & IV.
Complete debulking surgery requires multiorgan resections with well recognized peri-operative surgical complications. A real challenge in everyday clinical practice is identification of patients who will benefit from RS thereby avoiding unnecessary morbidity with effect on QoL and probably shorten overall survival (3, 10). Being unable to achieve complete or optimal cytoreduction is an outcome that should ideally be predicted preoperatively. As expected a high complete rate of 85.7% has been achieved for the women who had radical surgery. For these, the most common concurrent procedures were rectosigmoid resection (n=20, 47.6%), small bowel resection (n=10, 23.8%) and splenectomy (n=9, 21.4%).
An average morbidity of 5-30% and average post-operative mortality of 3.7% after surgery for OC has been reported (16). Common complications in our study were blood loss >1,500 ml (n=14, 33.3%), hospitalization >7 days (n=31, 73.8%), sepsis (n=8, 19%), ileus (n=6, 14.3%). There was only one case of reoperation for abdominal abscess (n=1, 2.4%) and one case of long-term bowel complication after ileostomy (n=1, 2.4%). In our cohort, the short-term mortality was zero. Recently, Kumar et al. developed a useful nomogram to predict complications for patients undertaking PDS for advanced stage OC (17). This nomogram can be a potent tool for pre-operative consultation and individualization of treatment planning.
We recognize a number of strengths in our study. This is one of the few case series reported in the literature for RS in OC. There was consistency in decision made at MDT and the surgeons involved. Moreover, we have a comprehensive cancer registry. Also, tumor stage, volume and distribution of tumor implants and the type of concurrent procedures were recorded in electronic and written medical records. Thus, we are confident that our cohort is representative of our population and we were able to accurately record the surgical outcomes and morbidity.
Main limitations of our study are the retrospective type of study, the small sample size in the study period examined and that we reported outcomes for a period of 2 years and 6 months after surgery. So, long-term complications and survival have not been assessed.
In conclusion, surgery and platinum-based chemotherapy remains the key treatment for advanced stage OC. Identification of patients who will benefit from RS avoiding unnecessary morbidity is real challenge. Our findings support the practise where RS for OC can be offered to selected patients, with good surgery outcomes and low rate of morbidity. Also, it will be interesting to follow-up these patients to assess their QoL and look at survival figures.
- Received November 27, 2017.
- Revision received December 12, 2017.
- Accepted December 14, 2017.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}