


Abstract
Background: Vitamin D is known for its anticancer potential. Prostaglandin E2 (PGE2) is a proliferative and inflammation-activating agent. The production of PGE2 is dependent on the activity of cyclooxygenase-2 (COX2). A link between vitamin D and PGE2 metabolism was shown recently. Materials and Methods: In MDA-MB-231 and MCF-7 breast cancer cell lines, we investigated the influence of calcitriol and the COX2 inhibitor celecoxib on cell growth via the MTT test, as well as on the protein and mRNA expression of COX2 using western blot and quantitative real-time polymerase chain reaction (qRT-PCR). Results: The proliferation of MCF-7 and MDA-MB-231 was inhibited by both calcitriol and the COX2 inhibitor celecoxib and even more strongly by their combination. Moreover, calcitriol inhibited COX2 protein expression in MDA-MB-231 cells, as well as COX2 mRNA expression in both cell lines. Conclusion: The combination of calcitriol and celecoxib demonstrated a synergistic growth-inhibitory effect in breast cancer cell lines.
The estimated annual incidence of breast cancer in the USA for 2014 for women is 232,670, with an estimated 40,000 deaths (1). In 2010, 17,853 patients with breast cancer died in Germany (2). Thus, it is the most significant malignancy in females. Because of the increasing number of patients, there is an unmet need for new preventative strategies and new treatment approaches.
Many advances in breast cancer treatment have been made in the past decade. Many biological approaches have led to targeted and more effective treatment, and gene-expression profiling for a better understanding of breast cancer and its subgroups. Numerous new promising targets still warrant further exploration. Two of these targets are cyclooxygenase-2 (COX2), the key enzyme required to convert arachidonic acid to prostaglandins (PG), and calcitriol [1,25-dihydroxycholecalciferol or 1,25-(OH)2D3], which is the biologically active form of vitamin D (3).
Calcitriol is known to suppress cell growth, tumor growth and inhibit metastasis, as well as prolong survival in animal models (4). It particularly inhibits the growth of human breast cancer cell lines (5, 6). Multiple epidemiological studies have suggested that vitamin D has a protective effect against the carcinogenesis and progression of breast cancer (7-10). However, concerning the correlation between vitamin D intake and breast cancer risk, data are still conflicting (9-13). Calcitriol has been shown to exhibit significant anti-inflammatory actions in breast cancer cells (14, 15). The pro-inflammatory PGs play an important role in the development and progression of breast cancer (16).
Increasing attention has been paid to the role of an inflammatory microenvironment in carcinogenesis. The interaction of inflammatory cytokines, growth factors and oncogene activation has been implicated in the fast induction of COX2 expression during carcinogenesis as COX2 affects tumor progression by participating in malignant proliferation, invasion and metastasis (17). High expression of COX2 is associated with increased proliferation, invasion, apoptotic resistance and angiogenesis (18, 19) and is, therefore, associated with a poor prognosis for patients with cancer (20).
Several epidemiological, preclinical and clinical studies support the idea that COX-targeting non-steroidal anti-inflammatory drugs (NSAIDs) play protective roles against breast cancer (21-24). Consequently, we hypothesized that a combination of COX2 inhibition and calcitriol could exert an increased antiproliferative effect on breast cancer cells and could offer new preventative or treatment approaches in the future. A link between vitamin D and PGE2 metabolism (25-27) was already proposed in breast cancer tissue (28, 29) in our recent publications.
The aim of the current study was to evaluate a possible synergistic activity of calcitriol, as the active form of vitamin D, and the COX2 inhibitor celecoxib in breast cancer cells.
Materials and Methods
Cell culture. MCF-7 and MDA-MB-231 breast cancer cell lines were purchased from Leibniz-Institut DSMZ-Deutsche Sammlung von Mikroorganismen und Zellkulturen GmbH (Braunschweig, Germany). The cells were grown in RPMI 1640 (Life-Technologies, Darmstadt, Germany) supplemented with 10% fetal calf serum (FCS) and penicillin/streptomycin (both from PAA-Laboratories, Cölbe, Germany), at 37°C in a humidified atmosphere with 5% CO2.
Growth experiments. To compare the proliferative rate between treated cells we used 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT)assays. Briefly, 3,000 cells/well were plated on a 96-well microplate. After 24 h, the medium was changed to contain 3% FCS and test substances were added [calcitriol (0.001, 0.01, 0.1, 1 and 10 μM), celecoxib (1 and 10 μM) and combination of calcitriol and celecoxib (10 μM calcitriol and 1 μM celecoxib, 10 μM calcitriol and 10 μM celecoxib)], all of which were re-solved and diluted in dimethylsulfoxide (DMSO); 1,000 × stock solutions for calcitriol and 10,000×stock solution for celecoxib (both from Sigma, Taufkirchen, Germany). All solvent controls contained 0.1% DMSO. Six wells were treated for each concentration of each agent used. After 72 h of treatment, the medium was replaced by 10% MTT solution (5 mg/ml thiazolyl blue in PBS; Sigma) for a further 4-h incubation period. The reaction was then stopped and dissolution of formazan crystals was performed in the dark overnight by adding 100 μl stop-solution (10% (w/v) sodium dodecyl sulfate, 50% N,N-dimethylformamide, pH 4.7). A microplate-reader (Dynatech Laboratories-MRX; DPC Biermann, Bad Nauheim, Germany) was used to measure the absorption of the wells at 560 nm.
Protein expression. To compare the COX2 protein expression, 300,000 cells were plated on 6-well plates in growth medium for 24 h. Afterwards, treatment with 0.1 μM calcitriol, 1 μM calcitriol, 1 μM celecoxib and the combination of 1 μM calcitriol and 1 μM celecoxib was performed in media without FCS for 24 h. Total protein was then extracted using MPER-buffer (GE Healthcare, München, Germany). Equal amounts of protein were analyzed in western blots with a monoclonal COX2 antibody (clone CX229; Biomol, Hamburg, Germany) and a β-actin antibody (clone AC-15; Sigma). Immunoreactive bands were detected with the Immobilon-Western-Chemiluminescent-HRP-Substrate on Hyperfilm-ECL-Performance-Chemiluminescent-Film (both from GE Healthcare). The films were scanned and a densitometric analysis of the protein bands was performed using Easy-Win software (Herolab, Wiesloch, Germany).
Expression of COX2 mRNA. For the relative comparison of COX2 mRNA expression, quantitative reverse transcription polymerase chain reaction (qRT-PCR) was used. Therefore, 300,000 cells per well were plated on a 6-well plate in growth media and the media were replaced after 24 h by fresh media containing 3% FCS together with agents. After 24 h of treatment, total RNA was isolated by using QIAzol (Qiagen, Hilden, Germany). For reverse transcription, 1 μg RNA was used together with random primers and Superscript-II (Invitrogen, Karslruhe, Germany). For qPCR, Platinum-SYBR-Green-qPCR-Super-Mix-UDG (Invitrogen) was used. As primers for COX2, we used the Hs_PTGS2_1_SG-QuantiTect-Primer-Assay (Qiagen) and for hypoxanthine-guanine phosphoribosyltranferase 1 (HPRT1), we used forward: 5’-TCA GGC AGT ATA ATC CAA AGA TGG T-3’ and reverse: 5’-AGT CTG GCT TAT ATC CAA CAC TTC G-3’ primers (synthesized at Metabion, Martinsried, Germany). The PCR protocol consisted of 42 cycles for 15 s at 95°C and 30 s at 60°C. Each sample was tested in duplicates. Data were further processed with the Excel-based program REST-MCS©-version 2 (Qiagen).
Results
Treatment of breast cancer cell lines with calcitriol. Calcitriol reduced the growth of MCF-7 breast cancer cells significantly at concentrations between 100 nM and 10 μM to 71.5% and 36.8%, respectively, compared to the solvent control (Figure 1A). The growth of MDA-MB-231 cells was also inhibited by 10 μM calcitriol to 88.4% (Figure 1B).
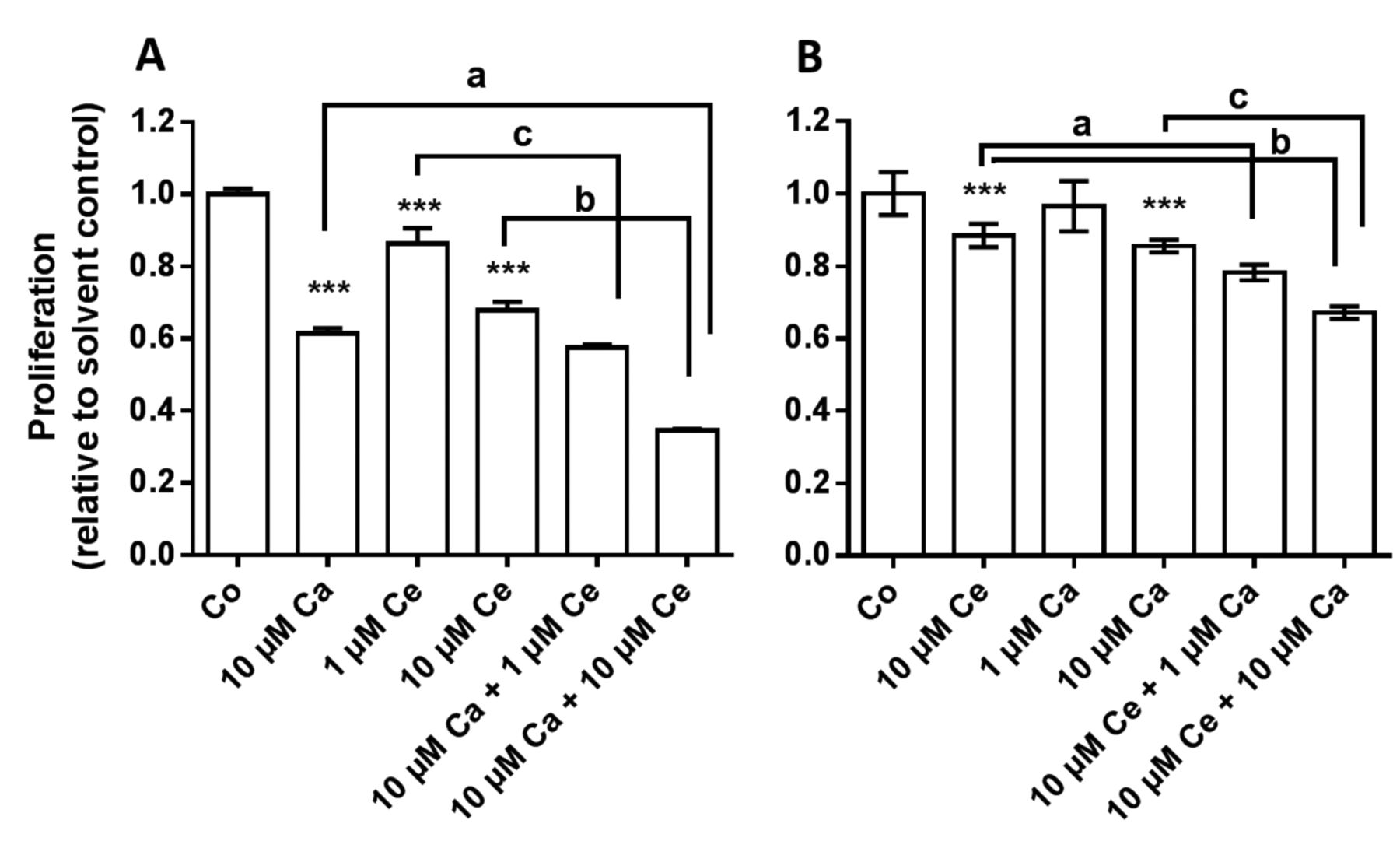
Combined treatment with calcitriol and celecoxib. The growth of breast cancer cell lines was inhibited by 10 μM calcitriol as already seen in the experiment above. Furthermore, growth was significantly inhibited by 10 μM celecoxib in MCF-7 and MDA-MB-231 cells to 67.8% and 88.4%, respectively. In MCF-7 cells, the effect of the combination of 10 μM celecoxib and 10 μM calcitriol was significantly stronger than that of calcitriol alone (Figure 2A) and of celecoxib alone (Figure 2A). Celecoxib at 1 μM significantly reduced the growth of MCF-7 cells and, furthermore, the addition of 10 μM calcitriol to 1 μM celecoxib inhibited cell growth more than 1 μM celecoxib alone (Figure 2A). In MDA-MB-231 cells, the combinations of 10 μM celecoxib with 1 μM calcitriol, as well as with 10 μM calcitriol, inhibited cell growth significantly more strongly than 10 μM celecoxib alone and 10 μM calcitriol alone (Figure 2B).
COX2 protein and mRNA expression under the influence of calcitriol and celecoxib. COX2 protein was detected in western blots of proteins from MDA-MB-231 (Figure 3) but not MCF-7 cells. After 6 h of treatment with 0.1 or 1 μM calcitriol, the density of the western blot signal for COX2 decreased at both concentrations to 62.7% compared to the solvent control. Celecoxib had no effect on COX2 protein expression and the combination of celecoxib and calcitriol reduced COX2 protein to 87%. The results were quantified using densitometry and normalized with the immunoreactive signals of β-actin. The COX2 mRNA expression in MDA-MB-231 and MCF-7 cells significantly decreased after 3-h treatment with celecoxib, as well as with calcitriol (Table I). It is remarkable that nearly the same decline in mRNA expression was found in both cell lines after treatment with celecoxib and calcitriol, because the expression of COX2 mRNA in MCF-7 cells seemed to be extremely low when compared with MDA-MB-231 cells. The latter statement is based on an estimation from the comparison of polymerase chain reaction cycle-time differences between the HPRT1 and COX2 of both cell lines. The combined treatment with celecoxib and calcitriol hardly affected COX2 mRNA expression.

The influence of calcitriol on the growth of breast cancer cell lines. Cell growth of MCF-7 (A) and MDA-MB-231 (B) cells was assessed by the MTT assay after 72 h of treatment with different concentrations of calcitriol. The results are shown as the mean±SEM; statistical significance: ***p<0.001. Co, Control.

Combined treatment with calcitriol and celecoxib on MCF-7 (A) and MDA-MB-231 (B) cells. The proliferation is shown as the mean±SEM of cultures compared to the solvent-treated control. Statistical significance: ***p<0.001. For the combined treatments, compared to single treatments: A: a, b and c = p<0.001; and B: a = p<0.01, b and c = p<0.001. Co, Control; Ca, calcitriol; Ce, celecoxib.

Cyclo-oxygenase 2 (COX2) protein expression in MDA-MB-231 cells after treatment with calcitriol and celecoxib. Western blot was carried out using COX2 antibody and β-actin as a loading control. Co, Control; Ca, calcitriol; Ce, celecoxib.
Discussion
In the present study, we observed an inhibition of proliferation in two breast cancer cell lines by both calcitriol and the selective COX2 inhibitor celecoxib. We also recorded an apparently additive inhibition under their combination. This additive inhibition in breast cancer cell lines was shown for the first time.
Colston and Hansen summarized several studies, clarifying that calcitriol can influence the cell cycle, cell differentiation, invasion and apoptosis of breast cancer cells in vitro (30). In a recently published study, we showed inhibition of breast cell proliferation by calcitriol in MDA-MB-231, MCF-7 and MCF-10F cells (27). This is in line with data by Yuan et al. (17), who showed that 1,25-(OH)2D3 significantly inhibited the proliferation of MCF-7 cells in a time- and dose-dependent manner using MTT assays. In contrast to the results of Yuan et al., we used higher concentrations of calcitriol to receive comparable inhibitory effects, which might be explained by different growth conditions.
The main focus of our study was to treat breast cancer cell lines with the combination of calcitriol and the COX2 inhibitor celecoxib. The growth inhibition by celecoxib of breast cancer cell lines that we observed has been shown previously (31,32); e.g. by Dai et al., who observed a time- and dose-dependent inhibition of proliferation in both MCF-7 and MDA-MB-231. In contrast to Dai et al., we used lower concentrations of celecoxib and only one treatment time of 72 h (32). At 10 μM celecoxib, we observed a reduction of proliferation comparable to that found by Dai et al. Furthermore, we combined the application of calcitriol with celecoxib, each at 10 μM and observed significant additive antiproliferative effects compared to each of the single applications. Therefore, we suggest that the combination of both substances might be a valuable tool for the targeted treatment of breast cancer cells.
Measurement of cyclo-oxygenase 2 (COX2) mRNA after treatment with calcitriol and celecoxib. Results are the mean±SEM of treated cells versus the untreated solvent control.
A further interesting question was to examine the connection, if any, between the vitamin D and PG pathways. Therefore, we measured COX2, the central PG-synthesizing enzyme, after treatment with calcitriol. A decrease of the COX2 protein content in MDA-MB-231 cells, as well as in the mRNA level in both tested breast cancer cell lines was found. Yuan et al. also addressed this issue (17) and showed a decrease of COX2 protein in MCF-7 cells; we did rot detect COX2 protein in MCF-7 cells. Why Yuan et al. were able to detect COX2 by western blot and we were not, might be due to a different version of the cell line or different culture conditions. For us, it did not seem to be unusual that the COX2 protein content in MCF-7 was under the level of detection, since we estimated the COX2 mRNA level relative to HPRT1 to be approximately 1,000 times lower compared to that in MDA-MB-231 cells. After treatment with celecoxib, the COX2 protein level decreased in MDA-MB-231 cells. Moreover, celecoxib seemed to counteract the inhibitory effect of calcitriol. Regarding COX2 mRNA, our results are in line with Dai et al. showing a decrease in COX2 mRNA after treatment with celecoxi. However, in our study, mRNA was analyzed after 6 h and in the study of Dai et al. after 48 h (32).
Down-regulation of COX2 expression by calcitriol is an important issue in breast cancer, because it limits the synthesis and biological actions of pro-inflammatory PGs (5).
Epidemiological studies support a protective effect of vitamin D. In a recently published meta-analysis, the authors concluded that a low blood level of calcitriol was associated with an increased risk of recurrence and death of patients with breast cancer (10). However, regarding the prevention of breast cancer by vitamin D supplementation, data are conflicting. While in the results of the meta-analysis by Sperati et al. vitamin D supplementation did reduce the breast cancer risk (13), Chen et al. stated an inverse relationship between vitamin D intake and breast cancer risk (33).
To date, calcitriol has been evaluated in a number of preclinical and some clinical studies as an antitumor agent in different carcinomas [reviewed in Trump et al. (34)]. The maximum tolerated dose of calcitriol is still unclear and calcitriol is recommended to be used restrictively due to its potentially hypercalcemic impact (35, 36). Only a sparse number of clinical trials regarding the use of calcitriol in combination with chemotherapy for cancer treatment exist with dissatisfactory results (34). The ASCENT-I-Trial (AIPC Study of Calcitriol Enhancing Taxotere) evaluated the combination of docetaxel and calcitriol in patients with pre-treated and advanced prostate cancer but the study was stopped because the treatment arm was associated with shorter survival than the control arm (37).
The importance of COX inhibitors is widely recognized, since they suppress breast cancer cell growth both in vivo and in vitro (16, 38). The inhibition of COX2 by the selective inhibitor celecoxib apparently inactivates the transcription of aromatase and thereby inhibits the proliferation of tumor cells in estrogen-responsive breast cancer (39). Furthermore, celecoxib is able to induce apoptosis in different types of cancer (40). Epidemiological studies support the hypothesis of breast cancer prevention by NSAID administration. Several studies, including one meta-analysis, reported a reduction of breast cancer risk after NSAID use of between 16% and 40% (23, 24, 41, 42). In different murine models for breast cancer, celecoxib reduced tumor growth, increased apoptosis and reduced neoangiogenesis (43, 44).
The correlation between COX2 and estrogen metabolism is an important issue. The inhibition of aromatase expression due to COX2 inhibition is an interesting therapeutic strategy. Several clinical trials have been conducted to investigate the use of COX2 inhibitors regarding their impact on breast cancer. The German Breast Group completed a multicenter clinical phase III study, the REACT trial, which analyzed the combination of endocrine treatment and celecoxib in primary breast cancer (www.gbg.de). Various other combination therapies with COX2 inhibitors regarding the metastatic setting were completed with inconsistent data (45-48). In a preoperative decision-making setting, two studies were recently published (49, 50): In the study by Brandao et al., patients with breast cancer were randomized to receive either pre-operative 400 mg celecoxib twice daily for 2 to 3 weeks or placebo. The impact on proliferation was reflected by a reduction of Ki-67-positive cells (49). However, in a similar setting, Martin et al. found no statistically significant changes in Ki-67 expression. (50). The first data suggest a possible treatment approach for combination of COX2 inhibitors and calcitriol in breast cancer (25) as both PG and calcitriol metabolism influence carcinogenesis and tumor growth. The metabolism of calcitriol and prostaglandin is linked by various factors and thus a synergistic effect might be supposed. The group of Moreno et al. demonstrated growth inhibition in prostate cancer cells by COX2 inhibitors and calcitriol. They used benign and malignant prostate cell lines and illustrated that calcitriol inhibits the PG-dependent proliferation of prostate cancer cells. Moreover, the authors showed that a combination of calcitriol with a COX2 inhibitor had a synergistic effect on the growth inhibition of prostate cancer cells (51).
We conclude that the combination of the COX2 inhibitor celecoxib and calcitriol cooperatively inhibits the growth of breast cancer cell lines. Calcitriol reduces aromatase expression by direct repression, as well as via an indirect effect due to reduction in the levels of PGs (5), and celecoxib supports this suppressive effect on estrogen synthesis. Therefore, we suggest a therapeutic role of the combination of celecoxib and calcitriol in hormone receptor-positive breast cancer, probably with the addition of an aromatase inhibitor. Based on our findings, we believe that it is worth considering prospective clinical trials showing the beneficial actions of celecoxib and calcitriol in endocrine-responsive breast cancer.
Footnotes
This article is freely accessible online.
- Received October 31, 2017.
- Revision received December 18, 2017.
- Accepted December 29, 2017.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.