


Abstract
Background: Radiofrequency ablation (RFA) is an alternative to hepatic resection and one of the major therapeutic options for hepatocellular carcinoma (HCC). Here, we investigated the long-term outcomes of RFA as an initial treatment for HCC. Patients and Methods: From January 2000 to December 2014, we treated 1,043 patients with RFA for HCC at the Kumamoto University Hospital; 327 of these patients (31.4%) were treated for primary HCC. After exclusion of 75 patients who underwent combined therapy, data for 252 patients were examined. We retrospectively analyzed the long-term outcomes of RFA and identified factors of poor prognosis. Results: The median platelet count, prothrombin activity and indocyanine green retention rate at 15 min were 9.1×104/μl, 83% and 26%, respectively. The 5-year overall survival (OS) rate was 69% and the median survival time was 7.0 years. The 5-year recurrence-free survival (RFS) rate was 17%, and the median RFS was 2.0 years. A multivariate analysis revealed that age >80 years [hazard ratio (HR)=7.76, p=0.011], tumor diameter >2 cm (HR=1.68, p=0.047) and multiple tumors (HR=1.87, p=0.014) were independent prognostic factors for poor OS. For RFS, des-γ-carboxy prothrombin (DCP) ≥40 mAU/ml (HR=1.47, p=0.038) and multiple tumors (HR=1.63, p=0.0056) were independent prognostic factors. Local recurrence at the ablated site occurred in 33/252 patients (13%), and in 33/372 tumors (8.9%). Conclusion: Although our cohort included patients with relatively worse liver function, a favorable 5-year survival rate 69% was obtained by RFA. DCP ≥40 mAU/ml and multiple HCCs contribute to a higher risk of recurrence. Patients with these factors should therefore be followed-up intensively.
Hepatocellular carcinoma (HCC) is the fifth most common cancer in the world (1). Many treatments are now available for HCC, including hepatic resection, local ablation therapy, transcatheter hepatic arterial chemoembolization (TACE), and transplantation (2). Local ablation such as radiofrequency ablation (RFA), microwave coagulation and percutaneous ethanol injection play important roles in the management of HCC (3). Hepatic resection or RFA is recommended for HCCs with a diameter of ≤3 cm in patients with good liver functional reserve, according to the guidelines established by the American Association for the Study of the Liver Disease (4), the European Association for the Study of the Liver (5) and Japanese evidence-based guidelines (6, 7)
RFA is becoming an alternative therapy for small HCC tumors (≤3 cm) because it is efficient and has an extremely low associated mortality rate, and it is much less invasive than hepatic resection (8, 9). The 5-year overall survival (OS) rate after percutaneous RFA of small HCCs is reported to be comparable to that of hepatic resection (7, 10-12). However, relatively high local recurrence rates of HCC following RFA have been reported, with 1-year local recurrence rates ranging from 9.7% to 15.0% and 3-year local recurrence rates ranging from 19% to 27% (13-16). It was also reported that 12.5% of a series of patients with HCC showed biopsy-proven needle-track seeding 4-18 months after RFA, and intrahepatic dissemination after RFA could be a serious problem (17-19). It is thus important to evaluate long-term outcomes and identify risk factors for recurrence after RFA for HCC.
Here we retrospectively examined the long-term outcomes after RFA as initial treatment for patients with HCC with relatively unlimited tumor size and liver function, and identified factors of poor prognosis in the patients.
Patients and Methods
Patients. From January 2000 to December 2014, we treated 1043 patients with RFA for HCC at Kumamoto university hospital. Of these patients, 327 (31.4%) were treated for primary HCC. Seventy-five patients (22.9%) were excluded from the study because they had undergone RFA combined with therapies such as hepatic resection (67 patients), microware coagulation (one patient) and percutaneous ethanol injection (eight patients). Thus, a final total of 252 patients were examined. The median follow-up time of this patient series was 41 months.
RFA procedures. When a patient's tumor was not close to the liver surface and was detected by percutaneous ultrasonography, percutaneous ultrasonography-guided RFA was selected. When the tumor was located on the liver surface or was undetectable by percutaneous ultrasonography, laparoscopic RFA or RFA with laparotomy was selected (20). When the tumor was located near the hepatic dome and was undetectable by percutaneous ultrasonography, thoracoscopic RFA or RFA with thoracotomy was selected (20). When tumors were multiple and located on the liver surface or deeper, percutaneous and laparoscopic or thoracoscopic RFA were combined.
For tumor ablation, an electrode with a 2- to 3-cm exposed tip (Radionics, Burlington, MA, USA) connected to a 500-kHz RF Generator (Radionics) was used. A tip temperature of 10-20°C was maintained by chilled saline solution infusion via a peristaltic pump. After electrode insertion into the lesion, we gradually increased the power to 60 W in a 2-cm-long needle or 80 W in a 3-cm-long needle at the rate of 20 W/min. After ablation exposure, we stopped the pump and measured the temperature of the needle tip. To achieve an accurate and wide tumor margin, we ablated not only the tumor nodule, but also the area surrounding the tumor, especially if the target nodule was >2 cm in diameter. Enhanced computed tomography (CT) was performed 7 days after RFA to evaluate the tumor response to RFA in all patients. Complete ablation was defined as the absence of contrast enhancement within the entire tumor. The procedure was repeated if an unablated tumor remnant was suspected.
Statistical analysis. Continuous variables are expressed as means±standard deviation (SD) and were compared using Student's t-test. Categorical variables were compared using either the chi-squared test or Fisher's exact test, as appropriate. Any death that occurred in the hospital after RFA was recorded as a mortality. Grade III-V complications of Clavien-Dindo classification (21) were recorded as morbidity. The OS and RFS curves were generated by the Kaplan–Meier method and compared by the log-rank test. We subjected variables that exhibited a probability value of less than 0.05 in a univariate analysis to a multivariate analysis using the Cox proportional hazards model. All analyses were performed with JMP® Pro 9.0.2 (SAS, Cary, NC). p-Values of less than 0.05 were considered significant.
Clinical characteristics of our cohort. Data are the mean ±SD or number.
Tumor-related and surgical factors of our cohort. Data are the mean±SD or number.
Results
Patient clinicopathological characteristics. The clinical characteristics of our cohort are summarized in Table I. The median age was 68 years. The ratio of men to women was 3 to 2. The tumor-related and surgical factors of our cohort are summarized in Table II. The median tumor size was 2 (0.5-6.7) cm. The numbers of single- and multiple-HCC were 162 and 77 patients, respectively. We treated a maximum of 10 tumors at one time.
Prognostic factors related to OS and RFS. The survival curves related to OS and RFS are illustrated in Figure 1. The 5-year OS rate was 69%, and the median survival time was 7.0 years. The 5-year RFS rate was 17%, and the median recurrence-free survival time was 2.0 years.
The univariate analysis revealed the following as factors of poor prognosis for OS: age >80 years, alpha-fetoprotein (AFP) ≥10 ng/ml, Lens culinaris agglutinin-reactive fraction of AFP (AFP-L3) ≥0.6%, des-γ-carboxy prothrombin (DCP) ≥40 mAU/ml, tumor diameter >2 cm and multiple tumors (Table III). The multivariate analysis revealed that age >80 years [hazard ratio (HR) =7.76, p=0.011], tumor diameter >2 cm (HR=1.68, p=0.047), and multiple tumors (HR=1.87, p=0.014) were independent factors of poor prognosis for OS (Table IV).
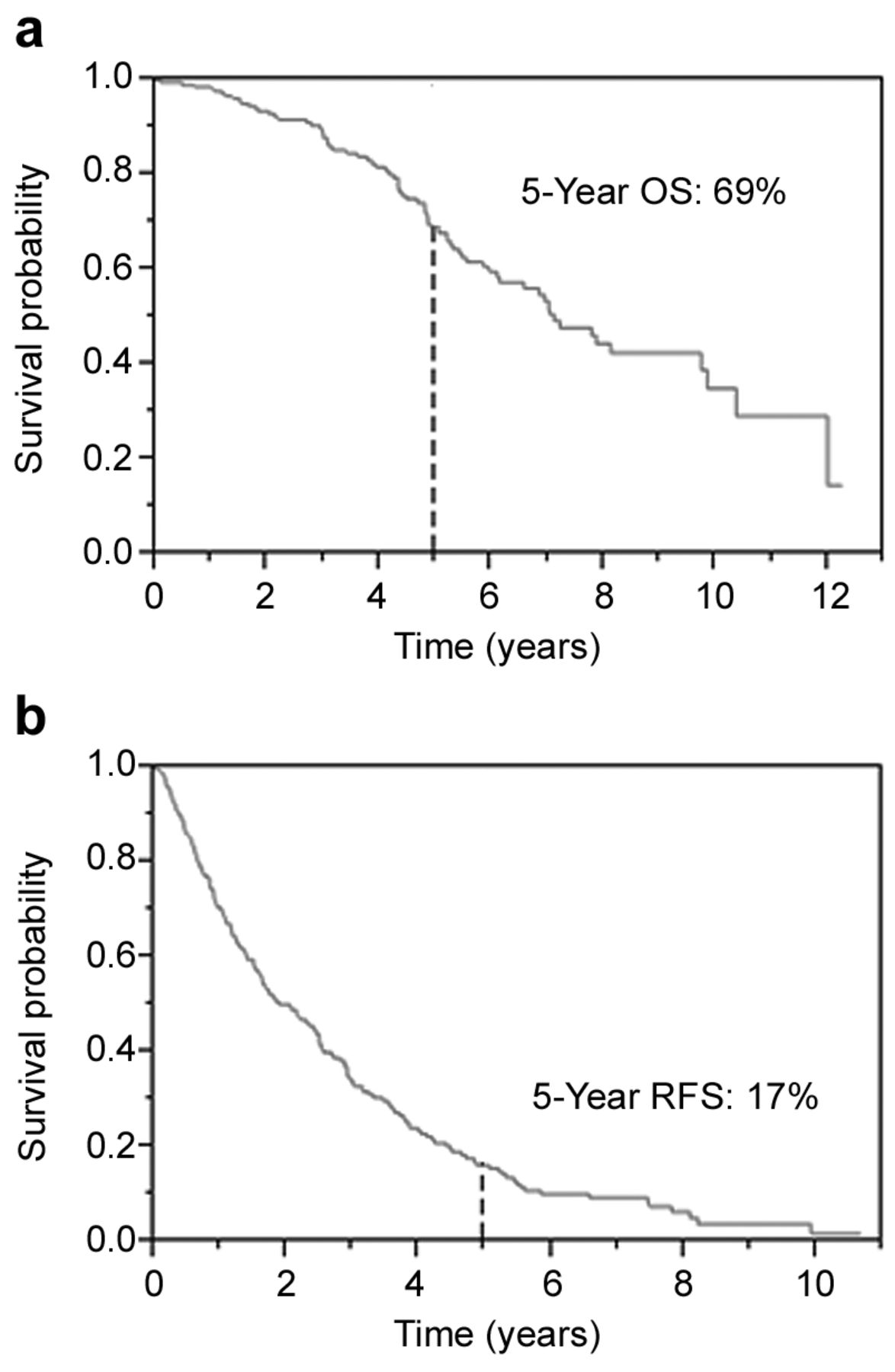
(a) The overall survival (OS) after radiofrequency ablation for primary hepatocellular carcinoma. The 5-year OS was 69%. (b) The recurrence-free survival (RFS) after radiofrequency ablation for primary hepatocellular carcinoma. The 5-year RFS was 17%.
For RFS, albumin <4.1 g/dl, AFP ≥10 ng/ml, AFP-L3 ≥0.6%, DCP ≥40 mAU/ml, and multiple tumors were identified as factors of poor prognosis in the univariate analysis (Table V). The multivariate analysis showed that DCP ≥40 mAU/ml (HR=1.47, p=0.038) and multiple tumors (HR=1.63, p=0.0056) were independent factors of poor prognosis for RFS (Table VI).
Prognostic factors related to local recurrence. We defined local recurrence after RFA as tumor recurrence in or on the ablation sites. Local recurrence at the ablated site occurred in 33 patients (13%), in other words, 33 out of a total of 372 HCCs (8.9%). After recurrence, 13 patients (39%) were treated with RFA again, 13 patients (39%) with TACE, two patients (6%) with hepatic resection, one (3%) with radiotherapy, and four patients (12%) were provided only best supportive care. The univariate analysis revealed DCP ≥40 mAU/ml as the significant predictive factor for local recurrence (p=0.0039).
Univariate analysis of factors related to overall survival.
Multivariate analysis of factors related to overall survival.
Discussion
The median follow-up time in this study, 41 months, was long compared to the 10.4-38.3 months in previous studies (1, 2, 7, 22-24). Our finding of a favorable long-term outcome, i.e. 5-year OS rate of 69.0%, was obtained although our cohort included patients with relatively poor liver functional reserve such as liver damage grade B (97 patients, 42%) and C (16 patients, 7%) (1, 2, 7, 22, 24). Other studies have reported lower 5-year OS rates after RFA for HCC, i.e. 59.4-61.1% (7, 22, 24). In two of those studies, the 2- and 5-year RFS rates were reported to be 44.6-69.3% and 23.9-28.3%, respectively (7, 22). In the present study, the 2-year RFS rate was 51.5% although tumor diameter was >3 cm in 26 patients (10.3%) and 11 (4.4%) patients had more than three tumors. We believe that the 2-year RFS rate similar to those of previous studies indicates that the efficacy of RFA in the local control of HCC was good in our cohort. The relatively worse 5-year RFS rate in our cohort suggests that more patients with multi-centric recurrences were included.
The albumin value (1), tumor diameter >2 cm, multiple tumors, AFP ≥15 ng/ml, AFP-L3 >15%, DCP ≥40 mAU/ml, age, hepatitis C virus positivity and Child-Pugh score B (2, 24) have been reported as independent prognostic factors for OS in patients with HCC. Here, we identified age >80 years, tumor diameter >2 cm, and multiple tumors as independent factors of poor prognosis for OS, and DCP ≥40 mAU/ml and multiple tumors as those for RFS. We have reported that the RFS and OS rates were significantly worse after RFA than after hepatic resection in cases of HCC >2 cm, whereas there were no significant differences in patients with HCCs ≤2 cm (7). Therefore, RFA would not be a good treatment option for patients with HCCs larger than 2 cm.
We also reported that patients with a high DCP level (>100 mAU/ml) are at risk for microinvasion even for those with HCCs ≤2 cm (25). Tumor size and the value of DCP can be confirmed before the treatment decision is made, and we therefore recommend that hepatic resection, not RFA, be performed in cases of HCC larger than 2 cm and for patients with a DCP value ≥40 mAU/ml.
Univariate analysis of factors related to recurrence-free survival.
Multivariate analysis of factors related to recurrence-free survival.
The limitations of this study include its retrospective and single-center design. We need to confirm our outcomes in more patients in multiple centers and compare our RFA outcomes to those obtained with hepatic resection and TACE. We are now registering our patients in and expecting the results of the Efficacy of Surgery vs. Radiofrequency A blation on Primary Hepatocellular Carcinoma (SURF) trial (26).
In conclusion, favorable prognosis, i.e. 69% 5-year survival rate, was obtained by RFA although our cohort included patients with poor liver function. Patients with DCP values ≥40 mAU/ml or multiple HCCs have a higher risk of recurrence, and clinicians should therefore choose RFA, hepatic resection or other treatments in a thoughtful manner and provide an intensive follow-up, especially for such patients.
Footnotes
Conflicts of Interest
The Authors declare they have no conflict of interest in regard to this study.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent: Informed consent was obtained from all individual participants included in the study.
- Received November 5, 2017.
- Revision received November 22, 2017.
- Accepted November 28, 2017.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.