


Abstract
Aim: Retrospective studies have suggested a protective effect of regional anesthesia against recurrence after cancer surgery. But confirmation of the in vivo antitumor effects is lacking. We examined the in vitro antitumor effects of lidocaine on various breast cancer cell lines and then assessed these properties in vivo at clinically relevant concentrations. Materials and Methods: In vitro experiments: normal breast epithelial cells (NBEC) MCF-10A and three tumor breast epithelial cells (TBEC) lines (MCF-7 luminal A, MDA-MB-231 triple-negative and SKBr3 HER2 positive) were exposed to increasing concentrations of lidocaine. Cell viability, migration and anchorage-independent growth were assessed by MTT, wound healing, and soft-agar growth assays. In vivo experiments: 6-week-old severe combined immunodeficient mice were injected intraperitoneally with MDA-MB-231 cells and were treated with intraperitoneal lidocaine or phosphate-buffered saline. The mice were euthanized when they reached experimental endpoints or sacrificed to determine peritoneal carcinomatosis index and global tumor volumes. Results: Lidocaine reduced the viability of all the cell lines, inhibited migration of TBEC compared to the NBEC, and compromised the anchorage-independent growth of the triple-negative cells. Intraperitoneal lidocaine improved survival of mice with MDA-MB-231 peritoneal carcinomatosis using doses that are consistent with the current clinical settings for analgesia. Conclusion: In agreement with the notion that local anesthesia may be beneficial for cancer therapy, lidocaine has a protective effect against breast cancer cells in experimental studies. However, the beneficial impact of local anesthetics on breast cancer needs to be strengthened by additional preclinical and clinical trials.
Breast cancer is the most commonly diagnosed cancer and the second cause of cancer-related death after lung cancer in women (1). Patients are increasingly opting for mastectomy; therefore, the number of breast surgery procedures has increased in recent years (2). The perioperative period is considered as a period of risk, since in some cases, surgery may be associated with cancer cell shedding and may have a metastasis-promoting effect (3-6).
Several retrospective studies have suggested an impact of anesthesia on survival of patients with cancer (7); notably, regional anesthesia is associated with a reduced risk of cancer relapse or recurrence (8, 9). One of the proposed hypotheses to explain these observations includes the opioid-sparing effects of regional anesthesia. Opioids have been implicated in promoting cancer progression (10, 11). Another possible reason for the improved cancer outcomes with regional anesthesia may be related to the antitumor effects of local anesthetics, including prevention of proliferation, migration or invasion of cancer cells (12, 13). Perioperative intravenous lidocaine infusion has been shown to reduce postoperative pain and opioid requirements (14, 15). Lidocaine has also been shown to induce apoptosis and suppress tumor growth in human breast tumor cells (16) as well as other in vitro tumor cells (12, 17-21). Additionally, it has been reported to enhance sensitization of breast cancer cells to chemotherapeutic drugs (22).
Although there are several in vitro studies assessing the antitumor effects of lidocaine, there is limited evidence of its effects in vivo (21). Moreover, the lidocaine concentrations used in these in vitro experiments may fit with infiltration use but were higher than those observed after systemic administration (23). Thus, there is a need to test the antitumor properties of lidocaine at doses relevant to systemic administration, notably, using doses which have been shown to improve recovery and prevent chronic pain in patients undergoing breast cancer surgery (24). In addition, it is postulated that lidocaine may exert antitumor properties through different mechanisms: directly on cell growth, inducing apoptosis or inhibiting proliferation, and indirectly by preserving natural killer cell activity (23), modulating pro-inflammatory macrophages, modifying mesenchymal stromal cells and then the local microenvironment (25-27). All these possible actions of lidocaine remain to be tested in a relevant preclinical model. The aim of this study was to evaluate the in vitro antitumor effects of lidocaine on several human breast cancer cell lines completed by in vivo assessment of the effects of lidocaine in a preclinical model of cancer.
Materials and Methods
In vitro Experiments
Cells and cell culture. Three human breast cancer cell lines representatives of the three main molecular subtypes used throughout this study were obtained from the American Type Culture Collection (Manassas, VA, USA): MCF-7 [estrogen (ER) and progesterone receptor (PgR)-positive], SKBR3 (ER- and PgR-negative) which has a high level of erb-b2 receptor tyrosine kinase 2 (ERBB2) oncogene amplification, and MDA-MB-231 (ER- and PgR-negative, no amplification of ERBB2 oncogene). When appropriate, they were compared to a non-tumorigenic mammary epithelial cell line: MCF-10A. The detailed characteristics of the tumor cell lines are described elsewhere (28). MCF-7 and SKBR3 cells were grown in Dulbecco's modified Eagle's medium (DMEM) enriched with 10% fetal calf serum (FCS), 2 mM glutamine, 50 μg/ml gentamycin in an atmosphere of 5% carbon dioxide (CO2) and 95% air at 37°C. Cell culture medium for MCF-7 was supplemented with bovine insulin (0.6 μg/ml). MDA-MB-231 cells were grown in RPMI-1640 without HEPES and enriched with 10% FCS and gentamycin (40 μg/ml). MCF-10A were grown in DMEM (1g/l glucose)/HAM F12 (3:1) enriched with 20 μg/ml adenine, 5 μg/ml insulin, 5 μg/ml human apo-transferrin, 1.5 ng/ml triiodothyronine, 2 ng/ml human epidermal growth factor (hEGF), 0.5 μg/ml hydrocortisone, 10% FCS and 40 μg/ml gentamicin. Subculturing was routinely carried out every week using diluted trypsin solution (0.25%) in Dulbecco's phosphate buffered saline (DPBS) without calcium and magnesium (pH 7.2).
Drug treatment. To perform in vitro experiments, lidocaine and lidocaine hydrochloride monohydrate were obtained in a pure powder form (MW 234.34 and MW 288.81 respectively; Sigma-Aldrich, St. Louis, MO, USA). A stock solution (50 mg/ml in absolute ethanol, and water, respectively) was freshly prepared and increasing drug concentrations (0.1, 0.5, 1, 5 and 10 mM) were obtained by diluting the stock solution in cell culture medium. We controlled for the pH of final media containing lidocaine or vehicle ensuring they were in the same normal range.
3-(4,5 Dimethylthiazol-2-yl) 2,5 diphenyl-tetrazolium bromide (MTT) assay. This rapid colorimetric assay was elaborated by Mosmann for cellular growth and survival (29). For each cell line, exponentially growing cells were enzymatically detached and a single tumor cell suspension in culture medium at a density of 30×103 cells/ml was prepared. Cells were seeded in 24-well microtiter plates (1 ml/well) and allowed to attach for 24 h under the previous specified conditions. Culture medium in each well was aspirated and replaced with fresh culture medium containing different lidocaine concentrations and cells were allowed to grow for a further 4 h. Triplicate wells were used for controls (absolute ethanol as vehicle alone) and each concentration. The cell viability was then determined by the MTT assay (30) with minor modifications. In brief, 100 μl of MTT (2 mg/ml in DPBS) were added and the plates were incubated at 37°C for 1 h in the dark. This assay is based on the cleavage of the tetrazolium salt by viable cells and the accumulation of a water insoluble formazan salt proportional to the number of living cells in the well. After careful aspiration of the culture medium, 150 μl of dimethylsulfoxide were added to each well and the plates were incubated for a further 1 h. The plates were read at wavelength 595 nm with reference to the appropriate blank (dimethylsulfoxide only) in a 96-wells microplate spectrophotometer (Biorad Laboratories, Hercules, CA, USA).
Cell migration was assessed by gap closure in wound-healing assay. A cell monolayer was made by seeding 4×105 cells in 6-well plates (2 ml/well) for 24 h. A scratch was then made using a 500 μl tip to mimic an injury. The wells were then washed with PBS and medium without FCS containing 0.1 mM of lidocaine or absolute ethanol as control and incubated for 24 h (and 48 h for MDA-MB-231 cells). Images were acquired at 0 and 24 h to measure the wound closure using ImageJ software (U.S. National Institutes of Health, Bethesda, MD, USA).
Soft-agar growth. Onto a culture plate was poured 0.6% UltraPure Low Melting Point Agarose (Invitrogen, Carlsbad, CA, USA) in the appropriate medium with lidocaine hydrochloride monohydrate, or water as control. On the top of this layer, a gel containing 5×103 MDA-MB-231 cells in 0.3% UltraPure Low Melting Point Agarose in appropriate cell medium and lidocaine hydrochloride monohydrate concentration, or water as control, was added. After 19 days of culture, stained colonies (1 mg/ml MTT) were visualized and counted using ImageJ software.
In Vivo Animal Experiments
Given that lidocaine affects cancer cell viability and migration in vitro, we extended this study to an in vivo preclinical model of cancer. In order to study the antitumor effects of lidocaine on MDA-MB-231 tumor cell line in vivo, a tumor model of peritoneal carcinomatosis in the Mouse was used.
Tumor model of peritoneal carcinomatosis. To generate intraperitoneal xenograft tumors, 5- to 6-week-old severe combined immunodeficiency (SCID) female mice (20 g in weight; Envigo, Gannat, France) were injected intraperitoneally with a suspension of 5×106 MDA-MB 231 tumor cells in 200 μl of Hanks' Balanced Salt Solution. Mice were clinically checked three times a week and were sacrificed when mice developed tumor side-effects such as ascites or reduced general condition with weight loss or bad grooming which constituted our experimental endpoints. All animal experiments were carried out according to the revised European Community directive (2010/63/EU, September 24, 2010) on the protection of animals used for scientific purposes and with an ethical agreement (no. 38.2012.01.046) according to the French transposition of the European Community directive.
Lidocaine dosage. Protocol of administration of lidocaine was designed to be relevant to general clinical practice: doses were chosen according to the current intraperitoneal lidocaine prescription used to reduce postoperative shoulder pain after laparoscopy (8 mg/kg) (31); dose adjustment for mice was made using the body surface area normalization method (32) resulting in a dose of 100 μl/10 g body weight of lidocaine solution (Aguettant, Lyon, France) at a concentration of 10 mg/ml. The repeated injection pattern was based on serial intravenous lidocaine infusions for the chronic management of patients with fibromyalgia (33) who received three injections of lidocaine at one-week intervals.
Experimental protocols. In a first group, used to determine the median survival of this peritoneal carcinomatosis model, 10 mice were inoculated with tumor cells as described above and were clinically examined three times a week until they were sacrificed when they reached the experimental endpoints. The obtained median survival day was used as the day of animal sacrifice in the determination of Sugarbaker index in the subsequent experiments.
In a second experiment, the first tumor reduction study with lidocaine treatment included two randomized groups of 10 mice each. The lidocaine group was injected intraperitoneally with 100 μl/10 g body weight of lidocaine solution (Aguettant) at a concentration of 10 mg/ml (or 100 mg/kg) weekly from day 14 to day 28 after inoculation of the cancer cells. The control group was injected intraperitoneally with 100 μl of PBS/10 g body weight using the same sequence protocol of injection. The animals were clinically examined three times a week until they were sacrificed when they reached the experimental endpoints and the corresponding median survival and log-rank tests were calculated. Mice were examined in a random order by an investigator who was blinded to drug-treatment group.
In order reduce the number of animals needed to be tested, a pilot study was designed with six mice in each group to determine survival rate and to perform a sample size calculation. According to a survival rate of 0.33 in the lidocaine-treated group and 0 in the control group at day 49, we calculated that 10 mice in each group (10% attrition included) would be required for the study to have 90% power with a two-sided alpha level of 5% for survival analysis (34). Because the materials and procedures used in the pilot study were similar to that in the main study, the data from the pilot study were incorporated into the main study.
In a second tumor reduction study, we used groups of five mice each devoted to the determination of peritoneal carcinomatosis index (PCI) according to Sugarbaker scaling adapted to small animals (35). Mice were randomly injected intraperitoneally with 100 μl/10 g body weight of lidocaine solution at a concentration of 10 mg/ml or with 100 μl/10 g body weight of PBS weekly from day 16 to day 28 after inoculation of the tumor cells. Animals were sacrificed at the day determined by the first in vivo experiment for PCI and tumor volume determined.
Determination of the Sugarbaker index and volume of the peritoneal carcinomatosis. Mice were euthanized via neck dislocation performed under inhalation anesthesia with 3% isoflurane (Forène, Abott, France) in 100% oxygen. The abdomen was opened by bilateral paramedian incision completed by a horizontal pubic incision generating a skin flap, which was folded upwards. The extent of peritoneal carcinomatosis was given by a modified peritoneal index (Sugarbaker index) adapted for tumor size and areas in rats as previously described (35). The resulting lesion size score was: 0 for no tumor seen, 1 for tumor up to 2 mm of diameter, 2 for tumor between 2 and 5 mm, and 3 for tumor more than 5 mm or confluent. Thirteen areas were recorded and the maximum score was 39.
After careful collection of all the tumors found in the different areas, the whole tumor volume was measured by water displacement (expressed in cm3 as ml equivalent). PCI and whole tumor volumes were assessed by an investigator who was blinded to drug-treatment group in random order for all animals.
Statistical analysis. Data are expressed as the mean±standard deviation. Each in vitro assay was performed in triplicate and at least three times. Results were compared with one-way repeated-measures ANOVA followed by a Dunnett test or Student's unpaired test where appropriate. Concerning in vivo data, tumor volumes, determined by water displacement, were tested for statistical differences between animal groups using one-way ANOVA followed by a parametric Student's unpaired t-test. Rodent survival curves were generated according to the Kaplan–Meier method (36) and differences between animal groups were put to the log-rank test. GraphPad InStat statistics software (GraphPad Software, Inc., La Jolla, CA, USA) was used for these analyses. p-Values of less than 0.05 were considered statistically significant.
Results
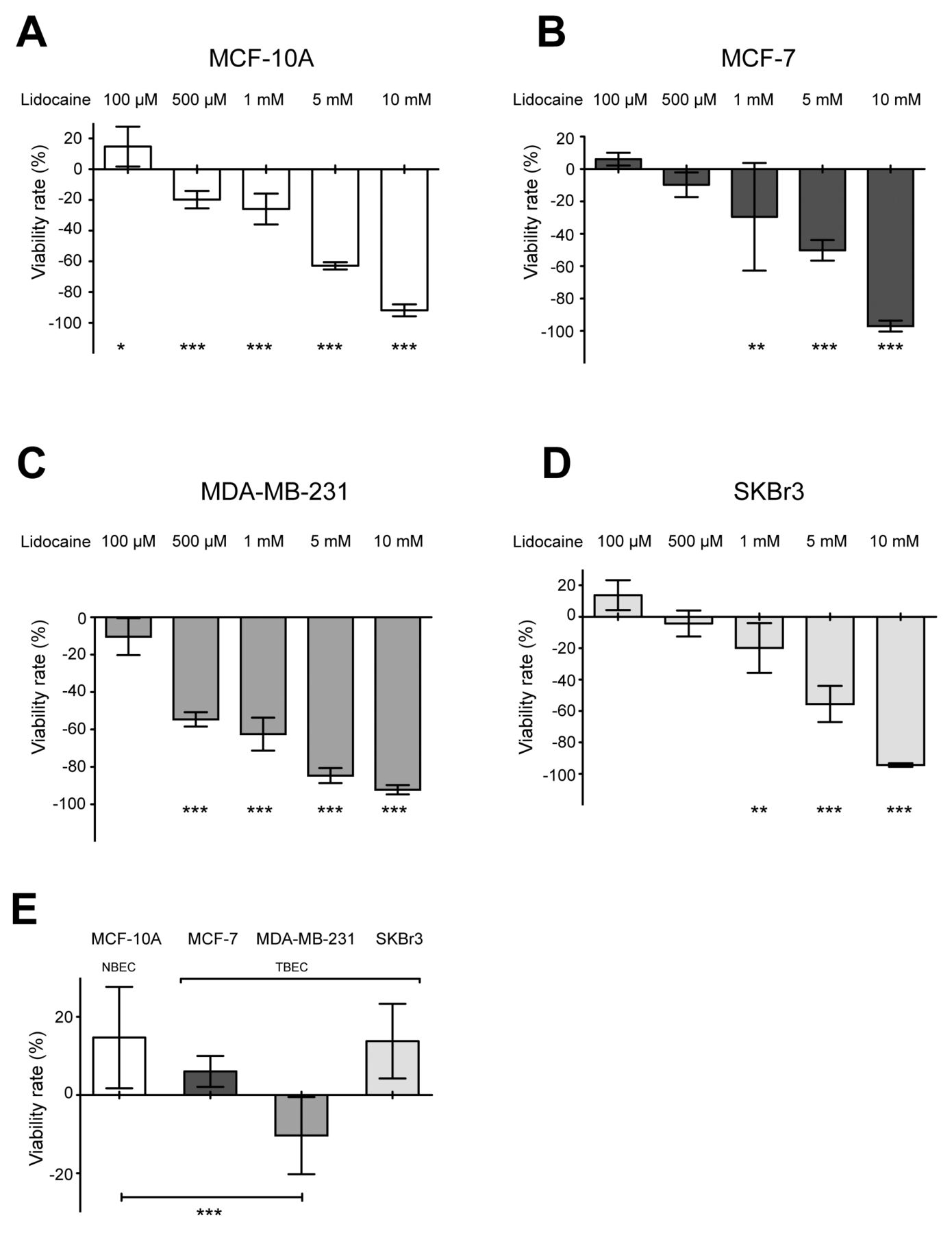
Lidocaine reduces cell viability of different human breast cancer cell lines. In order to test the effect of lidocaine on breast cancer cell viability, different cell lines were treated once with increasing dose of lidocaine for 4 h. Viability was assayed using the MTT colorimetric test. In all cell lines, high doses of lidocaine impaired viability (Figure 1). Of interest, the tumor-derived breast cancer cell lines MCF-7 and Sk-Br-3 were similarly affected by lidocaine at concentrations of 1 mM and more (Figure 1B and C). The triple-negative cell line MDA-MB-231 and normal cells MCF10A were more sensitive to lidocaine treatment, with a significant loss of viability at 0.5 mM (Figure 1A and D). Altogether these results indicate that lidocaine had a direct inhibitory effect on breast cell viability.
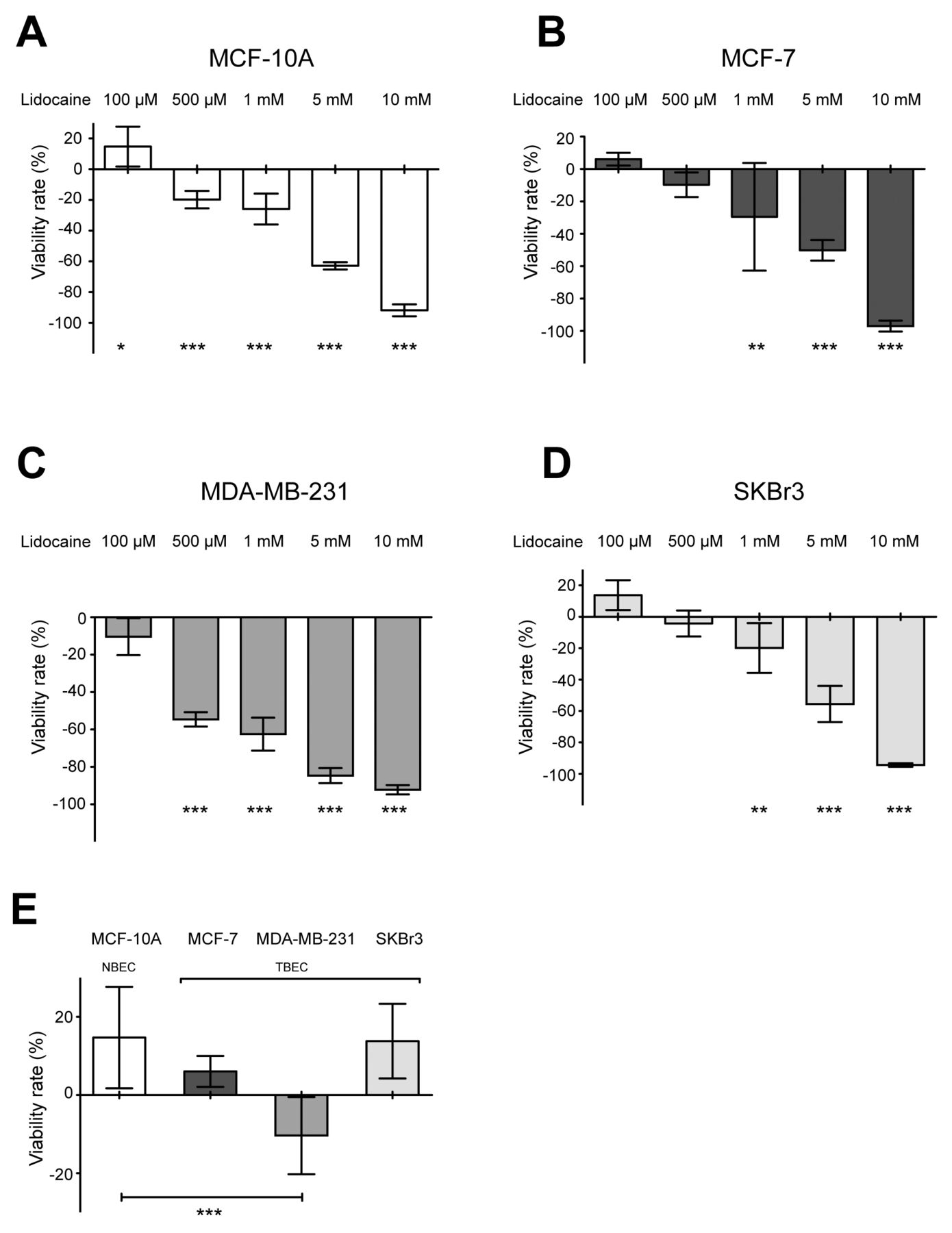
Effects of lidocaine on the viability of a panel of a breast epithelial cell lines: MCF10A normal cells (NBEC) and three tumor-derived cell lines MDA-MB-231, MCF-7 and SkBr3 (TBEC). Cells were exposed to vehicle alone (control) or increasing concentrations of lidocaine (from 100 to 10 mM) for 4 h then an in vitro MTT colorimetric assay was performed for quantitative analysis (relative to the control) of the inhibitory effects on viability on MCF10A (A), MCF-7 (B), MDA-MB-231 (C) and SKBr3 (D) cell lines. Effect on viability was also compared amongst all cell lines under the lowest concentration of 100 μM lidocaine (E). Data were analyzed by one-way repeated measures ANOVA: p<0.0001 for all the cell lines, and when comparing all the cell lines at 100 μM, followed by Dunnett's multiple comparison test (versus control): Significantly different at **p<0.01 and ***p<0.001. Data are the mean±SD, n=6.

Effects of lidocaine on the cell migration of two tumor breast epithelial cell lines compared to a normal epithelial cell line. In vitro wound-healing assay was performed by a scratching cell monolayer then treating cells with lidocaine (Lido) or not (CTL). Quantitative analysis of the inhibitory effect on wound closure was assessed by comparing gap closure by lidocaine at 100 μM, on MCF-10A (A), SKBr3 (B) and MDA-MB-231 (C) cell lines and comparison of all the cell lines after 24 and 48 h (D). Data were analyzed by unpaired t-test (A-C): Significantly different at **p<0.01 for SKBr3 and ***p<0.001 for MDA-MB-231, or one-way repeated measures ANOVA (D): p<0.001. ***Significantly different at Dunnett test p<0.001. Data are the mean±SD, n=9.
Lidocaine inhibits cell migration of different human breast cancer cell lines. A characteristic of breast cancer cells is their ability to migrate. We next studied cell migration in this series of cell lines using the wound-closure assay under control and lidocaine-treated conditions. Again, a single treatment of lidocaine was used. MCF-7 cells did not show any significant migratory ability (data not shown). In the human breast cancer cell lines SKBr3 and MDA-MB-231, migration was significantly inhibited in the lidocaine-treated group compared to the control group after 24 h of exposure (Figure 2B and C). A significant reduction of wound closure persisted after 48 h for MDA-MB-231 cells. No significant effect of lidocaine was observed in the normal breast epithelial cell line MCF-10A after 24 h of lidocaine treatment (Figure 2A). Of note, exposure to lidocaine at 0.1 mM resulted in a marked inhibition of the migration of both Sk-Br3 and MDA-MB-231 breast cancer cells when compared with MCF-10A cells (Figure 2D). Collectively, these results show that lidocaine had a predominant inhibitory effect on breast cancer cell migration.
Lidocaine reduces anchorage-independent growth of MDA-MB-231 cells. We observed that MDA-MB231 cells were more sensitive to lidocaine action. To confirm this notion, we tested the impact of lidocaine on soft-agar anchorage-independent growth of MDA-MB-231 cells. Colony formation was tested using increasing concentration of lidocaine (Figure 3) at plating. No other lidocaine treatment was added during the experiment. We observed decreased colony numbers when cells were treated with lidocaine hydrochloride monohydrate. This is consistent with the effect of lidocaine on cell viability observed previously (Figure 1). Of note, a significant decrease in soft-agar cloning was observed using 100 μM lidocaine at plating, a concentration lower than that needed to compromise viability (Figure 3). These data show that lidocaine compromised anchorage-independent growth of MDA-MB-231 cells.

Effects of lidocaine on the anchorage-independent growth of the triple-negative cell line MDA-MB-231. Soft-agar assay was performed to assess the impact of lidocaine on MDA-MB-231 anchorage-independent growth using increasing concentration of lidocaine or vehicle alone. Data were analyzed by one-way repeated measures ANOVA: p<0.001 followed by a Dunnett-test: Significantly different at **p<0.001 and ***p<0.001. Data are the mean±SD, n=9.
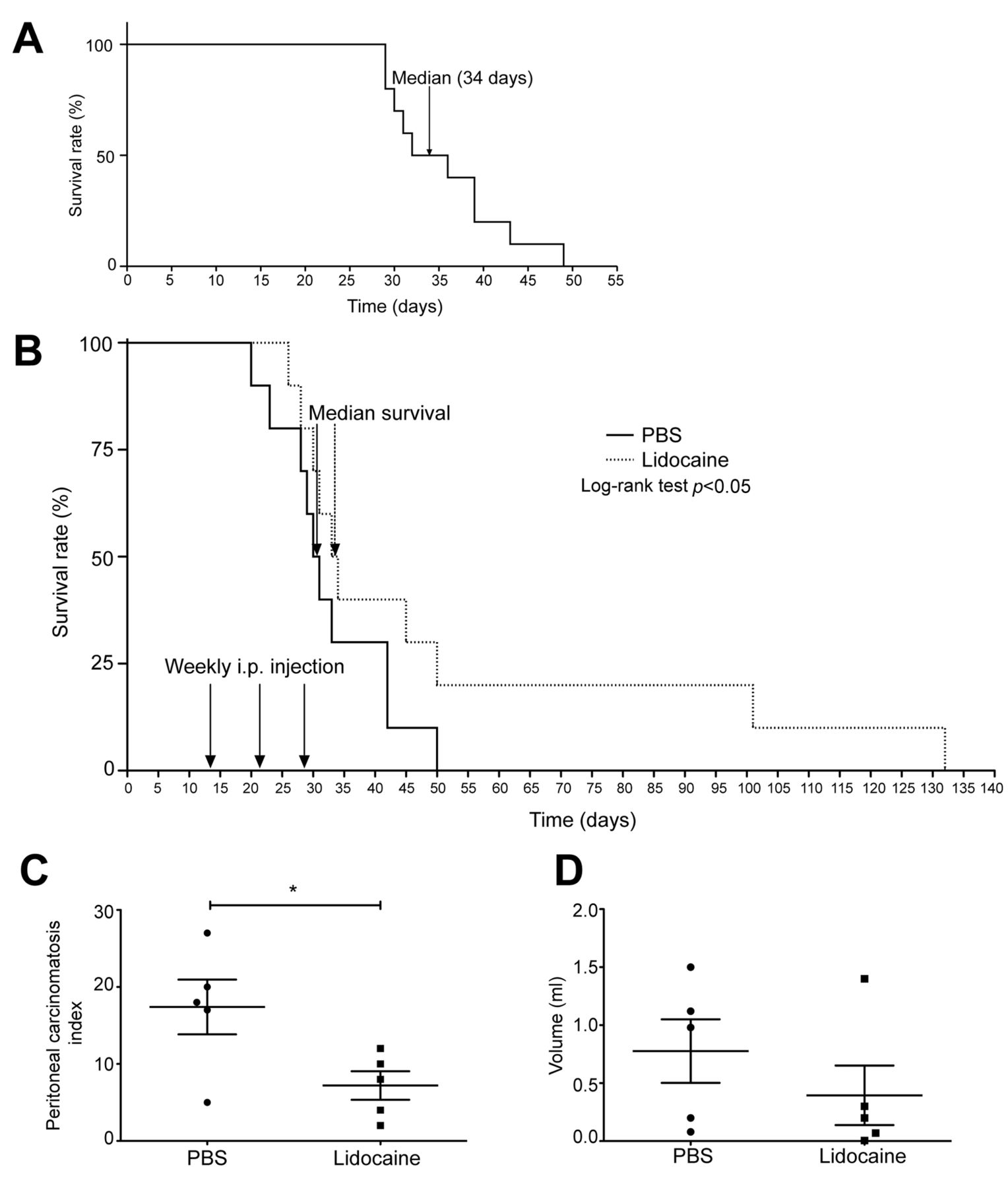
Determination of median survival of mice injected intraperitoneally with MDA-MB-231 cells. We first assessed the duration of median survival in the carcinomatosis model using MDA-MB-231 cells. The end of the experiment was established by comparing lidocaine-treated animals with those treated with PBS alone according to the Sugarbaker experiment. As illustrated in Figure 4A, the median survival time was 34 days. Because two animals out of 10 reached experimental endpoints at day 29, this time of treatment was selected for animal sacrifice to determine the PCI and tumor volumes under treatment.
Sequential intraperitoneal injection of lidocaine improves survival of mice with MDA-MB-231 peritoneal carcinomatosis. In a therapeutic attempt, lidocaine delivery began 2 weeks after carcinomatosis induction and was repeated every week to carry out a treatment over 3 weeks according to clinical repeated infusion of lidocaine in fibromyalgia (Figure 4B). With such a therapeutic regimen, lidocaine induced a significant improvement in animal survival when compared to controls (log-rank test with p<0.05) even if median survival was not significantly improved (30.5 versus 33.5 days, p=0.07). Survival of the treated animal was followed over 132 days (versus 50 days for the control group). No adverse effect was observed over the course of the experiment.
Lidocaine reduces tumor growth in vivo. To quantify the antitumor effects of lidocaine, tumor volumes and the extent of peritoneal carcinomatosis were measured in a separate experiment. Carcinomatosis parameters were investigated 29 days after tumor cell inoculation as determined in the first in vivo experiment. After sacrifice, the whole abdominal cavity was examined and scored in 13 predetermined areas for the presence and the grade of peritoneal carcinomatosis importance. All the nodules were then removed and their global volume was measured. Intraperitoneal injection of lidocaine significantly reduced the PCI: 7.20±2.07 versus 17.40±3.98 in controls (p=0.02) (Figure 4C). But the reduction of the intraperitoneal volume observed with lidocaine (0.395±0.290 cm3) even if it seemed obvious was not significant when it was compared to the mean volume for the control group (0.776±0.310 cm3, p=0.17) (Figure 4D), due to the significant standard deviation of the global tumor burden observed in the two investigated groups.
Collectively, these data show that repeated intraperitoneal injections of lidocaine delayed development of peritoneal carcinomatosis resulting in a prolonged survival for the treated group.
Discussion
The main findings of the in vitro study are that lidocaine had inhibitory effects on breast cancer cell viability and migration. Lidocaine also reduced anchorage-independent growth of MDA-MB-231 cells. A preclinical study in mice showed that sequential intraperitoneal injections of lidocaine reduced tumor growth and improved survival of mice with MDA-MB-231 peritoneal carcinomatosis.
Lidocaine action was measured in vitro, using a panel of human breast cell lines including lines that are representative of the principal breast cancer subtypes (28). In addition, we used the MCF10-A cell line, derived from human fibrocystic mammary tissue, that exhibits immortality and is considered a normal epithelial cell line (37). The MCF-7 human cell line was obtained from pleural effusion derived from a breast carcinoma, and is positive for expression of ER and PgR and represents the luminal subtype of breast cancer (38, 39). The SKBR3 cell line was derived from a pleural effusion from an adenocarcinoma originating in the breast and overexpresses the ERBB2 (HER2) gene product and represents the HER2 subtype (40). The MDA-MB-231 cell line is a triple-negative breast cancer (TNBC) cell line frequently used for investigation of the TNBC subtypes. TNBC represents approximately 15% of all breast cancer; this subtype has a poor outcome compared to the other subtypes and represents a therapeutic challenge (41, 42).

In vivo effects of intraperitoneal injections of lidocaine. A: Determination of median survival of mice injected intraperitoneally with MDA-MB-231 cells (n=10). Animal survival was monitored over a period of 49 days and is presented as Kaplan–Meier curve. Median survival was 34 days. B: Survival of animals bearing peritoneal carcinomatosis generated by injection of MDA-MB 231 tumor cells treated with lidocaine or phosphate-buffered saline (PBS). Mice bearing peritoneal carcinomatosis were divided into two groups (n=10) and treated with PBS (control) or lidocaine administered weekly from 2 to 5 weeks after carcinomatosis induction. Animal survival was monitored over a period of 132 days and is presented as Kaplan–Meier curves, with median survival and p-values. C and D: Quantitative in-vivo tumor effect of lidocaine application. Mice bearing peritoneal carcinomatosis were divided into two groups (n=5) and treated with PBS (control) or lidocaine administered weekly from 2 to 5 weeks after carcinomatosis induction and then were euthanatized for carcinomatosis grading. C: Effect of lidocaine on Peritoneal Carcinomatosis Index (PCI, SEM) according to Sugarbaker scaling adapted to small animals, unpaired t-test: *Significantly different at p<0.05. D: Effect of lidocaine on intraperitoneal tumor volumes (in ml, SEM), unpaired t-test showed no significant differences.
Our study showed that lidocaine can compromise the viability of all the tested cell lines in vitro but different sensitivity was observed among them. While a high concentration of lidocaine (above 1 mM) limited cell viability for all the cell lines tested, the TBNC line was more sensitive as its viability was compromised at a lower concentration (0.5 mM). These results suggest that the mechanisms of action of lidocaine on cell viability are different among distinct cell lines. These results are consistent with findings of breast (16, 19, 22) and other cancer cell types including A549 and H520 human non-small cell lung cancer cells (20), 8505C and K1 human thyroid cancer cells (17), PC-3 prostatic cancer cells and ES-2 ovarian cancer cells (19).
We noted that lidocaine inhibited migration of the HER2 and TNBC tumor breast epithelial cells without compromising migration of the normal breast epithelial cells. Of interest, the anti-migratory effects of lidocaine were observed at a low concentration (100 μM). This concentration had no effect on cell viability. These results on viability were obtained at lower concentrations and after shorter exposure than those tested in previous experiments using different human cell lines (17, 20) or breast cancer cell lines (16), thus confirming the notion that lidocaine has a direct antitumor potential. In addition, the conditions used in our experiments are relevant to clinical application during surgery. Moreover, another study using MDA-MB-231 cells did not observe any cytotoxicity of lidocaine for a longer exposure of 24 h at 1 mM (19). In addition, using the TNBC cell line, we showed that lidocaine reduced tumorigenicity in vitro, as assayed by anchorage independent cell growth. Again, the antitumorigenic effect of lidocaine was observed at a concentration not affecting the viability of this cell line.
Of interest, we observed that the TNBC cell line MDA-MB-231 was more sensitive to the direct inhibitory action of lidocaine. Given the high metastatic potential of this cell line and its sensitivity to lidocaine, we chose this TNBC cell line to investigate the effects of lidocaine in vivo. But considering that the concentration of 100 μM is higher than those considered to cause lidocaine toxicity in plasma [namely 5 μg/ml (15) or approximately 21 μM] an in vitro to in vivo translation experiment was strongly required to connect in vitro observations with clinical application. We chose an intraperitoneal xenograft in nude mice as a preclinical model (43). SCID mice express normal population and function of natural killer, macrophage and granulocyte cells (44) and lidocaine also has indirect antitumor properties by enhancing natural killer cell functions (23) and modulating the tumor microenvironment (25-27). We therefore assumed that lidocaine may have additive protective effects against tumor growth at relevant systemic concentrations. To measure the impact of lidocaine treatment on tumor growth, we treated mice during the course of disease progression in order to evaluate the properties of lidocaine as an adjuvant therapy. To determine the dose (31, 32) and the mode of administration of lidocaine (33) in this preclinical cancer model, we adapted protocols used in clinical practice. The dose of 100 mg/kg of lidocaine in mice corresponds to a dose of 8 mg/kg in humans according to the dose translation based on body surface area (32). In addition, in a pharmacokinetic study, the intraperitoneal administration of 400 mg lidocaine (i.e. 8 mg/kg in a 50 kg patient) was safe (45). We show that intraperitoneal lidocaine injection reduced breast cancer cell tumor burden and improves survival in the peritoneal carcinomatosis model. Moreover, no adverse effect was observed in treated mice, confirming the potential of lidocaine in clinical use.
Intraperitoneal administration of lidocaine presents many advantages: firstly, it has shown comparable efficacy as intravenous infusion in elective abdominal hysterectomy (46) or laparoscopic appendectomy (47) in term of analgesia; secondly, it could be a more efficient route for systemic chemotherapy (48), and thirdly, as our xenograft model is on of peritoneal carcinomatosis, tumors were directly exposed to lidocaine as minimal residual disease could be achieved with minimal invasive anesthetic techniques (i.e. surgical wound infiltration or infusion) (49). Along this line, the effects of peritumoral infiltration of lidocaine prior to excision are currently being assessed in a clinical trial (NCT01916317) with the aim of reducing the dissemination of cancer cells during surgery and improving the disease-free interval. Taken together, our study suggests that lidocaine may also be administered intraperitoneally to prevent peritoneal carcinomatosis even if rarely breast cancer metastasizes within the peritoneal cavity (50).
The antitumor effects of lidocaine at the molecular level remain unclear. Of interest, our study indicates that lidocaine had a greater antitumor effect on the MDA-MB-231 cell line, this line is known to overexpress the voltage-gated sodium channel (VGSC) (51), a canonical pharmacological target of lidocaine (52). The VGSC is composed of different subunits including the Nav1.5 α subunit which can be inactivated by lidocaine in cardiomyocytes (53). Consistent with the notion that lidocaine might exert its antitumor effects through this subunit, other reports showed that inactivating Nav1.5 α subunit with a different drug (e.g. phenytoin) can have antitumor effects in vitro (54) and in vivo (55). Perhaps this hypothesis should be further investigated, as phenytoin and lidocaine seem to have different binding sites on VGSC (52, 56). In addition, overexpression of the Nav1.5 subunit was reported in human breast cancer biopsy sections (57). Other hypotheses concerning other ion channels should also be explored. Indeed, the transient receptor potential channel, subfamily V, member 6 (TRPV-6), a calcium channel, may play a key role as lidocaine can inhibit the migration and invasion of TRPV6-expressing cells and reduce the intracellular-free Ca2+ level (19). Altogether, we can speculate that targeting VGSC using a well-characterized anesthetic drug such as lidocaine may be a good strategy to reduce metastatic risk (58).
Lidocaine is known to have analgesic, anti-hyperalgesic, and anti-inflammatory effects (14, 59). Indeed, intravenous lidocaine infusion administered as a component of multimodal analgesia is reported to reduce opioid requirements and improve pain relief (14). In a small clinical trial of patients undergoing breast cancer surgery, lidocaine infusion failed to demonstrate any significant effect on postoperative pain (60) but another trial showed that perioperative lidocaine infusion reduced the incidence of persistent postoperative pain (24). However, a recent meta-analysis concluded that the analgesic benefits occurred only in patients undergoing abdominal surgery (laparoscopic and open approach), and not for other surgical procedures (15). Despite the fact that the antitumor mechanisms of lidocaine are still unclear, using lidocaine during surgery might be beneficial to limit surgery-driven cancer cell escape from dormancy (5, 6) or tumor cell shedding (3, 4), and clinical trials are needed to include lidocaine in a repurposing drug program (61) notably to manage TNBC which does not respond to hormonal therapy (such as tamoxifen or aromatase inhibitors) or therapies that target HER2 receptors (such as trastuzumab).
In conclusion, the findings of these in vitro and in vivo experiments suggest that lidocaine may have a protective effect against breast cancer cells. However, the molecular mechanisms of lidocaine in cancer are unclear. The findings presented here, of potential beneficial impact of lidocaine on cancer should be strengthened by additional preclinical and clinical studies.
Acknowledgements
The Authors would like to thank Betty Heller and Corinne Wendling (IGBMC institute) for their help with the cell culture, Léa Wilhelm for the figure layouts and Marie-Christine Rio for her scientific support and discussion.
Footnotes
Funding
This study was funded by the grant ANR-10-LABX-0030-INRT, a French State fund managed by the Agence Nationale de la Recherche under the frame program “Investissements d'Avenir” labelled ANR-10-IDEX-0002-02. Thiên-Nga Chamaraux-Tran is an IGBMC International Ph.D. Program fellow supported by LabEx INRT funds. The Authors declare receiving funds from the charity Seins et Vie and the Société Française d'Anesthésie-Réanimation (SFAR).
Conflict of Interest
G.P. Joshi is a consultant for Pacira, Baxter, Mallincrodt and Merck Pharmaceuticals. The others Authors declare that they have no conflict of interest in regard to this study.
Ethical Approval
All applicable international, national, and institutional guidelines for the care and use of animals were followed. All animal experiments were carried out according to the revised European Community directive (2010/63/EU, September 24, 2010) on the protection of animals used for scientific purposes and with an ethical agreement (no. 38.2012.01.046) according to the French transposition of the European Community directive. This article does not include any studies with human participants performed by any of the Authors.
Presentation
Preliminary data for this study were presented as a poster presentation at the 2014 and 2015 American Society of Anesthesiologists Annual Meeting, and as oral communication at the 2014 and 2015 French Society of Anesthesia and Intensive Care Annual Congress.
- Received October 4, 2017.
- Revision received October 29, 2017.
- Accepted November 1, 2017.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Sodium channel-inhibiting drugs and cancer-specific survival: a population-based study of electronic primary care data
- Sodium channel-inhibiting drugs and cancer-specific survival: a population-based study of electronic primary care data
- The Effect of Lidocaine and Bosutinib on 4T1 Murine Breast Cancer Cell Behaviour In Vitro