


Abstract
Aim: To find new predictive factors for the efficient use of immune checkpoint inhibitors in patients with non-small-cell lung cancer (NSCLC). Patients and Methods: In this multicenter retrospective cohort study, we evaluated consecutive patients treated with nivolumab between January and October 2016 after second-line systemic chemotherapy. The endpoint was progression-free survival (PFS), as defined by Response Evaluation Criteria in Solid Tumors version 1.1. Results: A total of 189 patients were included in the study. Sixty-four percent had received two or more prior systemic therapies. In Cox proportional hazard analyses, Eastern Cooperative Oncology Group Performance Status of 2 or more, lactate dehydrogenase (LDH) ≥217 mg/dl, and carcinoembryonic antigen ≥13.8 ng/ml were independently associated with inferior PFS. LDH was not associated in the sensitivity analysis. Conclusion: In patients with NSCLC treated with nivolumab, worse pretreatment performance status, and higher carcinoembryonic antigen were associated with inferior PFS.
Nivolumab has favorable effects on overall survival compared to docetaxel, which has been the standard of care in second-line chemotherapy for advanced non-small cell lung cancer (NSCLC) (1, 2). Some patients have shown responses to nivolumab lasting for years (3).
Although immune checkpoint inhibitors (ICIs) such as nivolumab have a clear efficacy, they are associated with high cost (3). Programmed cell death-ligand 1 (PD-L1) is a promising biomarker which can be used to select patients who could benefit from ICI therapies (4). However, administration of ICIs for selected patients using PD-L1 as a biomarker is not cost effective even in developed countries (3, 5).
Several factors such as the mutation burden, lactate dehydrogenase (LDH) level, performance status (PS), and neutrophil/lymphocyte ratio (NLR) have been explored to predict the efficacy of ICIs. However, all of them have limited predictive value (6-9).
Hence, we evaluated the predictive values of pretreatment serum markers in patients previously treated with nivolumab for advanced NSCLC in usual clinical settings.
Patients and Methods
Study design and patients. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement during all stages of design, implementation, and reporting (10).
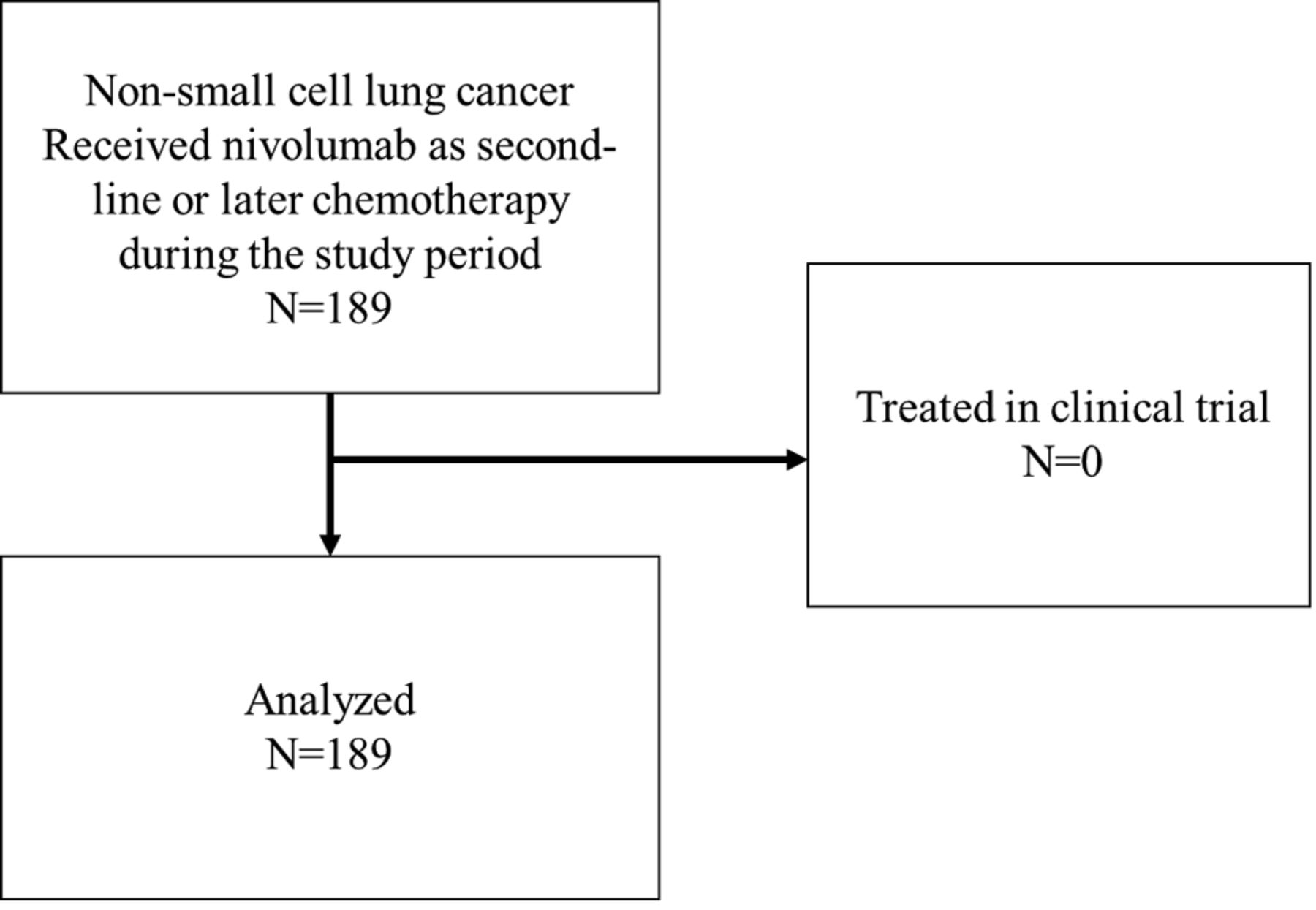
A retrospective cohort study was performed. The cohort included patients with pathologically proven NSCLC (11) who had received nivolumab (3 mg/kg intravenously every 2 weeks) as second-line or later treatment between January and November 2016 at five tertiary hospitals in Japan. December 2015 was the date of approval of nivolumab in Japan. Those who received nivolumab as part of a clinical trial were excluded from our cohort. The end date for the observation period for this study was December 2016.
Definitions of prognostic variables. Data on demographics including age, sex, comorbidity, number of prior systemic chemotherapy, histological type, PS, smoking history, and each of the serum markers [NLR, LDH, carcinoembryonic antigen (CEA), and fragments of cytokeratin-19 (CYFRA)] at the time of first administration of nivolumab were extracted from the chart review. CEA and CYFRA were measured by chemiluminescent enzyme immunoassay. Epidermal growth factor receptor (EGFR), and anaplastic lymphoma kinase (ALK) status were available only if such profiling had been performed as part of the routine clinical care. We defined cut-offs based on previous studies or median values (8, 9, 12, 13).

Study flow chart.
Definition of study endpoint. Progression-free survival (PFS) as defined by Response Evaluation Criteria In Solid Tumors (RECIST) version 1.1 (14) was used as the endpoint. We chose this endpoint because the treatment line for each patient was very different, and the observation period was limited. At each hospital, computed tomographic (CT) scans were performed every 6 to 8 weeks in routine care. Two researchers evaluated the endpoints independently and any disagreements were resolved by discussion.
Statistical analyses. Background information was summarized using summary statistics. PFS was estimated using the Kaplan–Meier method. Cox proportional hazards models were used to assess the impact of pretreatment markers on PFS. We used multiple imputations to handle missing data assuming they were randomly missing. Twenty datasets were imputed by normal regression and estimates from these datasets were combined using Rubin's rule (15). We conducted a sensitivity analysis of the complete-case data set. We used Stata® ver. 13.1 (Stata Corp., College Station, TX, USA).
Ethical considerations. This study was performed according to the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects from the Japanese Ministry of Health, Labour and Welfare. The protocol for the study was approved by the Ethics Committee of each hospital and requirement for informed consent was waived. The protocol was registered in the University Hospital Medical Information Network Clinical Trials Registry with the number: UMIN000022014.
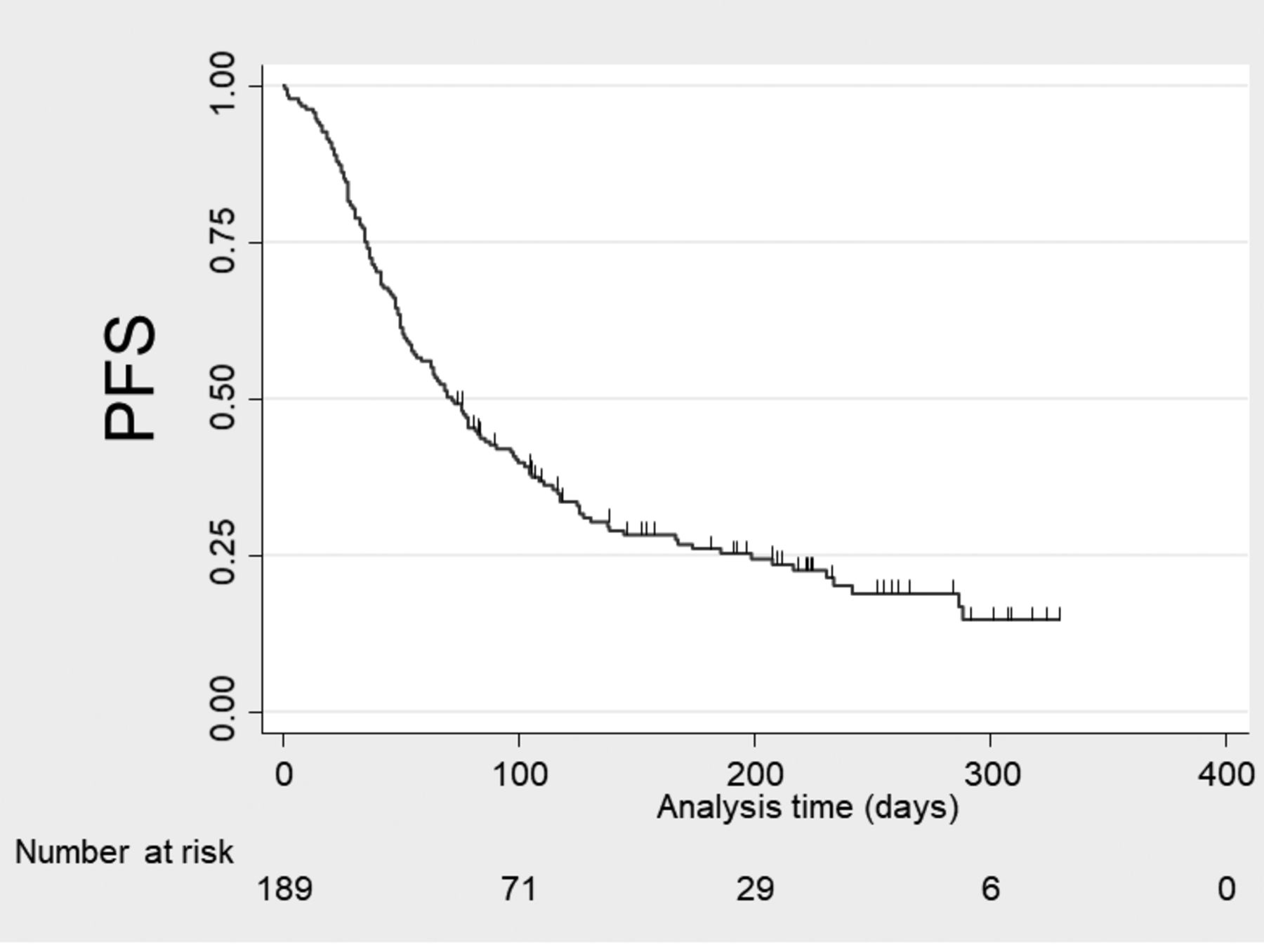
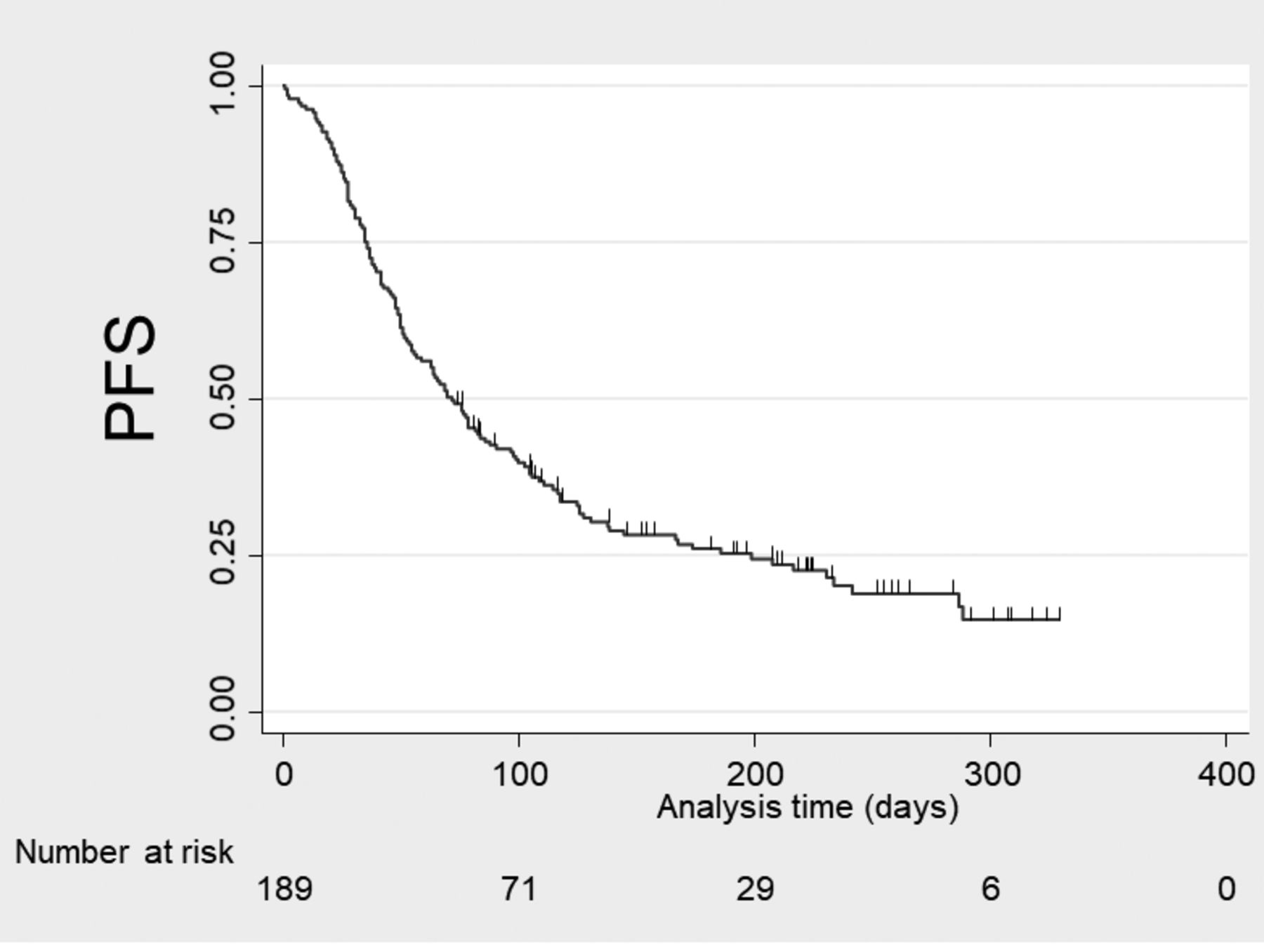
Kaplan–Meier survival curve for progression-free survival (PFS) of patients treated with nivolumab for non-small cell lung cancer.
Results
Characteristics. We included 189 patients with advanced NSCLC treated with nivolumab. No patients were excluded (Figure 1). Baseline characteristics are summarized in Table I. The median age of the patients was 69 (range=38-88) years; 26% were women, and 64% had received two or more prior systemic therapies. They received a median of five cycles (interquartile range=3-8) of nivolumab treatment.
Survival analyses. The median follow-up time was 5.5 months. Forty-six (24%) patients were censored. The median progression-free time was 2.4 months (Figure 2). Both univariate and multivariate analyses showed that PS of 2 or more, LDH ≥217 mg/dl, and CEA ≥13.8 ng/ml were associated with decreased PFS (Table II). In the sensitivity analysis performed via complete-case multivariate analysis, PS of 2 or more, presence of targetable driver mutation, and CEA ≥13.8 ng/ml were associated with decreased PFS (Table III).
Discussion
Our findings reveal that a high serum level of CEA and a poor PS were associated with a decreased PFS in patients with advanced NSCLC previously treated with nivolumab. Some previous studies have also shown the association between a high serum level of CEA and poor prognosis in patients with advanced NSCLC (16, 17). To the best of our knowledge, this is the first report of a serum tumor marker predicting the effectiveness of ICIs in patients with advanced NSCLC.
Squamous cell histology (vs. non-squamous histology) is reported as a predictive factor for ICIs (18). In this study, we analyzed tumor markers and histology simultaneously. High CEA was associated with decreased PFS, but squamous cell histology was not. This discrepancy suggests a predictive role for CEA which reflects the proportion of the histological subtype (19).
High serum LDH was associated with decreased PFS in the main analysis, but not in the sensitivity analysis. We used multiple imputations because the missing values were thought to be lost at random. Multiple imputations have been recommended for handling missing data (20). It is also reported to reduce bias from missing data and improve the precision of estimates (20). LDH has been reported as a predictive marker in patients with NSCLC treated with pembrolizumab (18). However, the predictive value of serum LDH needs further investigation.
In contrast, targetable driver gene mutations, smoking history, and NLR were not predictive factors. One reason could be the difference in the target population from those of previous studies. In this study, more than half of the patients had received three prior systemic chemotherapies, while prior studies that reported the predictive value of these factors included patients who had received fewer than two prior systemic chemotherapies (8, 21). Heavily treated cancer is known to accumulate mutations (22), which is an important predictive factor for response to ICIs (23) and could have acted as an unmeasured confounding factor.
Our study had several limitations. Firstly, the expression of PD-L1 in tumor tissues was not evaluated, although nivolumab was reported to have significant efficacy in a subset of patients with PD-L1-negative patients with NSCLC (2). Moreover, the expression of PD-L1 can change during chemotherapy (24, 25). Because PD-L1 expression with treatment is likely to be different from that at the time of diagnosis, the evaluation of serum markers which can easily be made during the course of treatment is important. Secondly, the timing of the CT scans was not predefined due to the retrospective nature of the study. At each hospital, CT scans were taken every 6 to 8 weeks in routine care. Finally, even with the careful use of the RECIST criteria, misclassification can occur (26). We believe that the evaluation by two independent observers would have reduced the information bias in this study.
In conclusion, CEA is a predictive marker of PFS in patients with advanced NSCLC treated with nivolumab. Patients with high CEA and worse PS should not be treated with nivolumab. A larger study with fewer missing values is needed to verify the reproducibility of our present findings.
Patient characteristics (n=189).
Unadjusted and adjusted hazard ratio for progression-free survival of patients treated with nivolumab for non-small cell lung cancer.
Unadjusted and adjusted hazard ratio for progression free survival (complete-case analysis)
Acknowledgements
The Authors thank Ms. Michie Kashiwabara and Ms. Misayo Ata for helping with the chart review, and Dr. Akira Hagiwara for interpreting the computed tomography data.
Footnotes
Funding Sources
This work was supported in part by a grant from the Hyogo Prefectural Amagasaki General Medical Center's fiduciary funds (for English editing).
Conflicts of Interest
D. Fujimoto and K. Hirano received honoraria from Ono Pharmaceutical Company and Bristol-Myers Squibb. K. Tomii received honoraria from Boehringer Ingelheim. H. Yoshioka received honoraria from Eli Lilly, Chugai Pharma, Boehringer Ingelheim, Taiho Pharmaceutical, Pfizer, AstraZeneca, Bristo-Myers Squibb, Ono Pharmaceutical, and Takeda.
- Received October 24, 2017.
- Revision received November 9, 2017.
- Accepted November 10, 2017.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.