


Abstract
Aim: We previously found that low-dose X-ray treatment after systemic administration of acridine orange (AO), which is known to have a low toxicity in animals, inhibited tumor growth in experimental studies using mouse osteosarcoma. In this pilot study, we planned to verify the toxicity of intravenous injection of low-dose AO in humans and investigate the anticancer effect of radiation after systemic AO administration (iAOR) for human cancer. Patients and Methods: Eight patients with terminal cancer were treated with iAOR. Results: None of the patients exhibited an adverse effect from AO injection. Three out of the five patients who received a full course of iAOR exhibited clinical or image-based responses, whereas two patients did not. Conclusion: The systemic administration of AO was confirmed not to be toxic in humans, and iAOR was suggested to be potentially effective against radioresistant cancer.
Based on intensive basic in vitro and in vivo research studies (1-3), we have established acridine orange (AO) therapy, including photodynamic surgery, photodynamic therapy (PDT), and radiodynamic therapy (RDT) after local administration of AO in patients with malignant musculoskeletal tumors, with the aim of reducing the surgical margin and obtaining better limb function without an increased risk of local recurrence and poor prognosis. Over 200 patients have been treated since 2009 in a multi-institutional study group in Japan. The clinical outcomes showed excellent limb function with a local recurrence rate similar to that following a wide resection (4-9). We also found that low-dose X-ray treatment after systemic administration of AO inhibited tumor growth in both in vitro and in vivo studies using a mouse osteosarcoma model (10). Therefore, we hypothesized that AO might also be effective for killing cancer cells after excitation with radiation energy in humans.
We previously performed in vivo experimental studies examining AO toxicity after intravenous injection and found that the median lethal dose (LD50) of AO was 30 mg/kg and that a 1 mg/kg injection was nontoxic in mice (11, 12). Other animal studies have also demonstrated that low-dose AO is nontoxic and is not carcinogenic (13-23).
Therefore, in this pilot study, we planned to verify the toxicity of intravenous injection of low-dose AO in humans and to investigate the anticancer effect of radiation after systemic AO administration (iAOR) for human cancer.
Patients and Methods
Eight patients were treated. Most of the patients had terminal clinical stage with local recurrence and invasion or multiple metastases after intensive chemotherapy, radiotherapy, or surgery. Two patients (cases 2 and 8) had a performance status (PS) of 1, four patients (cases 1, 4, 5 and 7) had a PS of 3, and two patients (cases 3 and 6) had a PS of 4. Two patients had sarcomas, two had pancreatic cancer, and one patient each had intrahepatic cholangiocarcinoma, renal, lung, and parotid cancer. After a full explanation of the study concept and risk, all the patients and their families agreed to participate in this trial, which was approved by the Institutional Review Board committee of our hospital (Certificate No. 13, Takai Hospital).
Patients received an intravenous infusion of 100 ml of AO solution (Sigma Aldrich Co. St. Louis, MO, USA) at a concentration of 0.5 or 1 μg/ml (0.5 or 1 mg/kg) diluted in saline over the course of 1 hour under vital monitoring. At 2 hours after the end of the infusion, the target cancer lesions were irradiated with 3 or 5 Gy of X-rays using a linear accelerator. The treatment was repeated at a one-week interval three times over 3 weeks in four patients. One patient (case 1) received an additional course of treatment because of a good response. One patient (case 6) was treated only once because of cancer-induced irritable pain arising from the huge size of the recurrent pelvic tumor mass, and two patients were treated only twice, one because of fatal radiation-induced pneumonitis (case 5), and one due to cancer-induced peritonitis with a large intraperitoneal recurrent tumor (case 3) (Table I).
Patient profiles.
Relationship between acridine orange (AO) dose and toxicity in all patients.
Results
Although none of the patients experienced significant symptoms after AO infusion (Table II), two patients had slight nausea, one had discomfort, and two patients had pain after radiation. One patient (case 5) died of radiation-induced pneumonitis. He had multiple pulmonary metastases of undifferentiated pleomorphic sarcoma and had been treated with a maximum dose of proton beam therapy and intensive chemotherapy prior to undergoing iAOR.
All the patients except for one died from their disease (n=5), from another disease (n=1), or from radiation pneumonitis (n=1) within 6 months of iAOR (Table I). Five out of the eight patients (cases 1, 2, 4, 7 and 8) received three or more treatments. Two out of these five patients (cases 1 and 8) showed a significant reduction in tumor size, as detected using computed tomography.
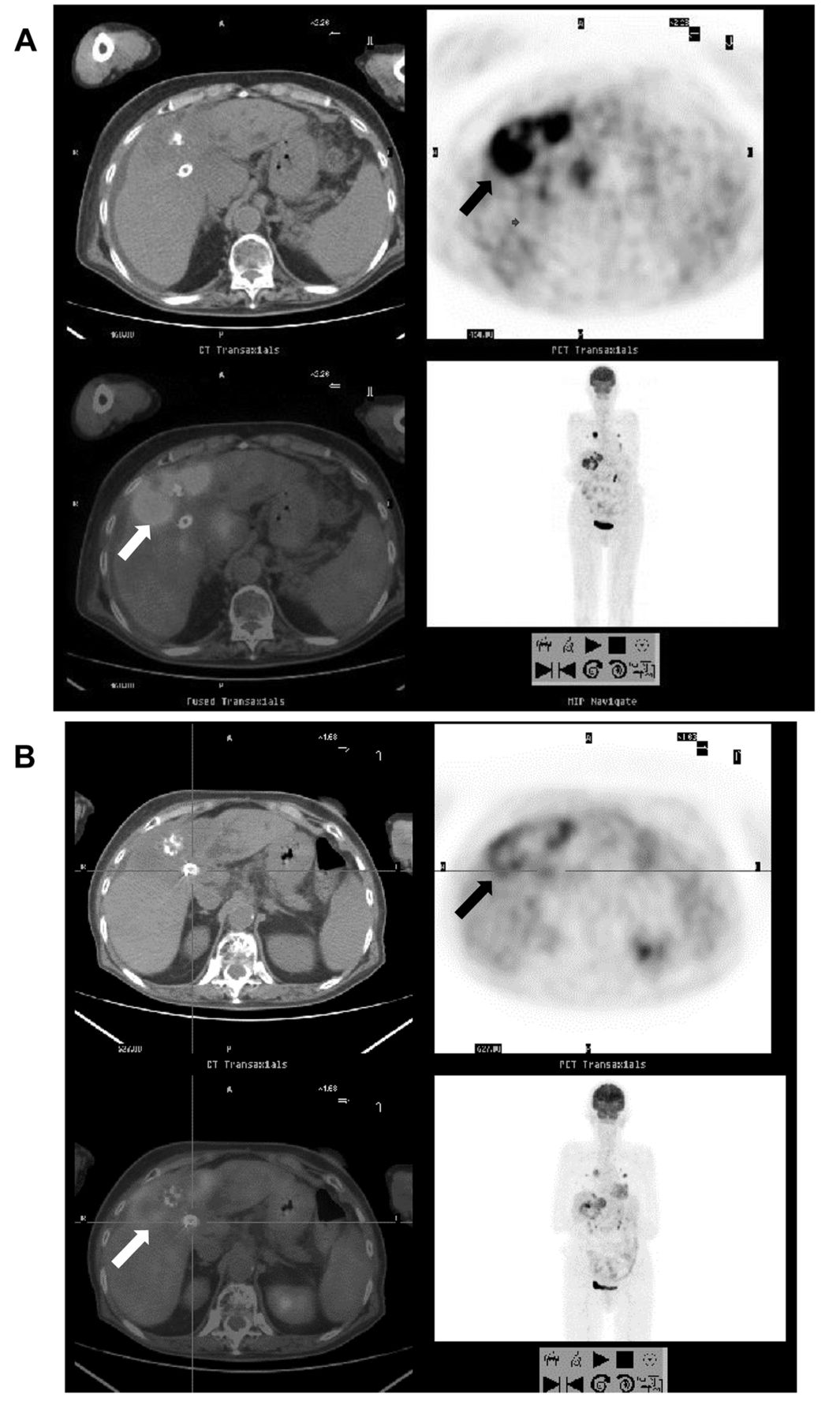
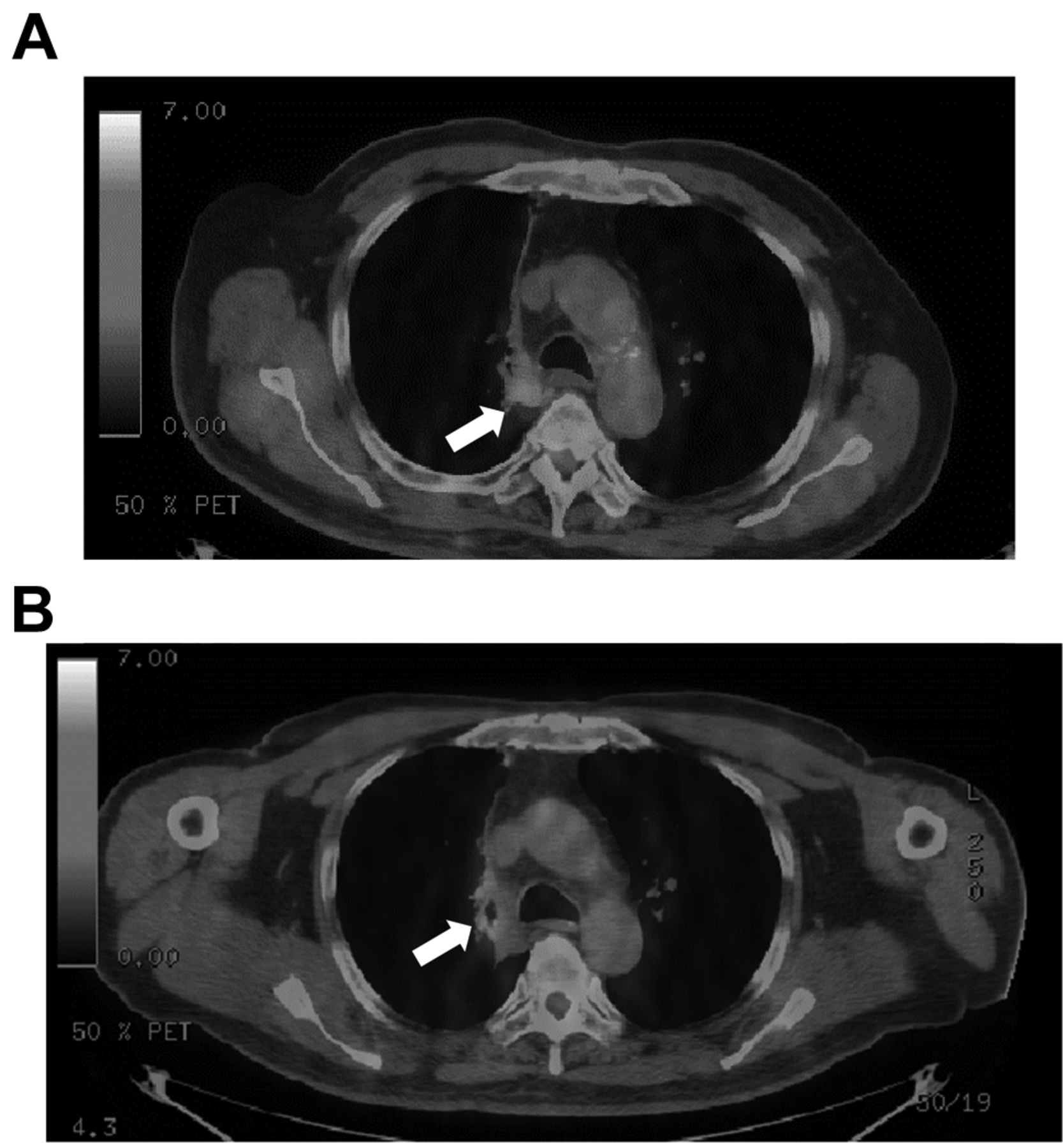
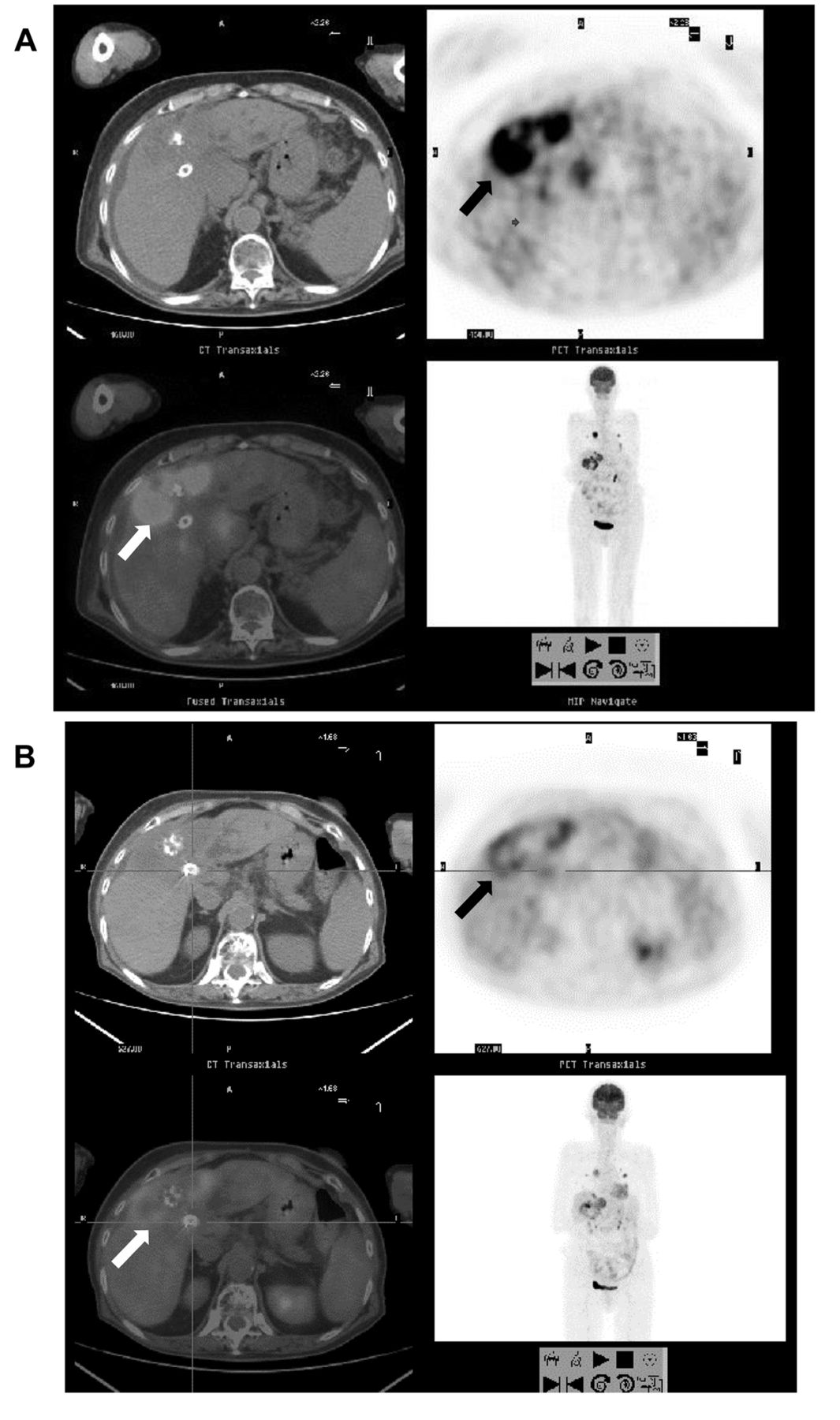
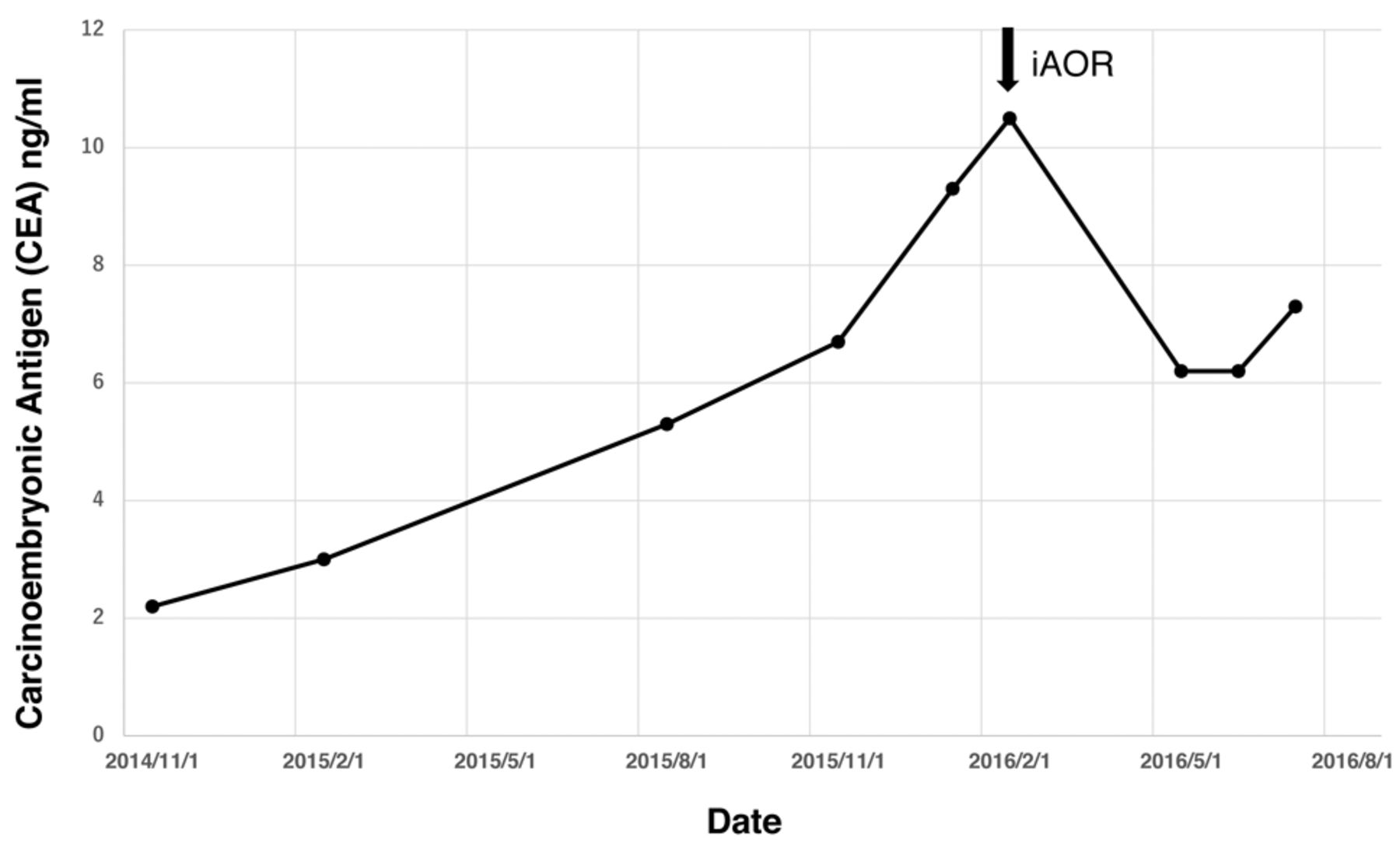
One patient (case 1) with recurrent intrahepatic cholangiocarcinoma and multiple pulmonary metastases after chemotherapy and ordinary radiotherapy showed an improvement in severe ascites, serious leg edema, and icterus after iAOR treatment. She had been unable to walk, but was able to resume walking with a cane after the therapy. Hemoptysis and severe coughing caused by lung metastasis also disappeared. A positron-emission tomography fused with computed tomography (PET-CT) demonstrated a decrease in 18F-fluorodeoxyglucose (FDG) accumulation in both the liver and lung lesions (Figures 1 and 2). The serum bilirubin level also decreased markedly (Figure 3). One patient with parotid cancer (case 7) and serious invasion to the cerebellum showed an improvement in facial nerve palsy after treatment (Japanese clinical facial nerve palsy recovery scale: from 10/40 to 18/40). The patient had been unable to walk because of vertigo, but was able to resume walking with a cane after treatment. Although magnetic resonance imaging findings showed a slight decrease in tumor size that was suggestive of tumor necrosis, the change was not significant (Figure 4). One patient with lung cancer recurrence (case 8), probably in the lymph nodes, showed a decrease in FDG accumulation on PET-CT after iAOR (Figure 5). The serum carcinoembryonic antigen level also decreased after therapy (Figure 6). The two patients with pancreatic cancer did not show a reduction in tumor size, and their diseases progressed (cases 2 and 4).
Positron-emission tomography (PET) (right; upper: axial slice, lower: whole body) and PET-computed tomography (CT) (left; upper: CT, lower: fusion with CT and PET) images of lung metastatic lesion (arrow) before (A) and after (B) first therapy with radiotherapy after intravenous administration of acridine orange in case 1 with intrahepatic cholangiocarcinoma.

Positron-emission tomography (PET) (right; upper: axial slice, lower: whole body) and PET-computed tomography (CT) (left; upper: CT, lower: fusion with CT and PET) images of liver recurrent lesion (arrow) before (A) and after (B) first therapy with radiotherapy after intravenous administration of acridine orange in case 1 with intrahepatic cholangiocarcinoma.

Sequential changes in serum-bilirubin after radiotherapy after intravenous administration of acridine orange in case 1.
In our evaluation of the antitumor effect of iAOR in this initial study, three out of the five cases who completed the treatment (cases 1, 7 and 8) showed a clinical or imaging-based response, while the remaining two (cases 2 and 4) did not. The response rate was 60%.
Discussion
Toxicity and carcinogenicity of AO. Since AO is mutagenic in bacteria (24, 25), it might also be carcinogenic in humans. However, several studies investigating the carcinogenicity of AO (13, 14, 22) did not provide any evidence to suggest such carcinogenicity. Therefore, the International Agency of Research on Cancer of the World Health Organization (15) and other sources such as those of the Pesticide Action Network Pesticides Database (16) and Thermo Fisher Scientific (17) do not classify AO as a carcinogen. There are some medical reports, in addition to ours, on the application of AO in human clinical studies. Two Japanese articles reported the use of local/oral AO administration for the diagnosis of cervical cancer or gastric cancer and neither described any serious complications of such therapy (18, 19). Recently, a study reported by an Italian group applied our method of AO-RDT to a patient with synovial sarcoma and showed good local control without any complications (20). In 2009, a group from the USA also applied AO to some patients with ovarian disease in a clinical study of confocal laser laparoscopic biopsy under Food and Drug Administration (FDA) approval (21). The FDA in the USA approved the application of AO in specific clinical studies after investigating the acute and chronic toxicity and carcinogenicity of AO using mice (22). In our human sarcoma studies using the local administration of AO, we treated more than 200 patients over 15 years, with none of the patients developing secondary cancer from the AO exposure site. Therefore, we believe that the risk of carcinogenesis induced by AO in our patients was at least not any greater to that associated with most other known anticancer agents.

Positron-emission tomography-computed tomography of recurrent lung cancer (lymph node: arrow) before (A) and after (B) radiotherapy after intravenous administration of acridine orange in case 8.
Sequential changes in serum carcinoembryonic antigen (CEA) after radiotherapy after intravenous administration of acridine orange in case 8.
Regarding the acute toxicity of AO, our study in mice revealed that the LD50 of AO following intravenous administration was 28-30 mg/kg (11, 12). The toxicity of 0.1 μg/ml of AO administered by intravenous injection has been investigated in dogs, with no significant adverse effects recognized (23). None of the above clinical or experimental reports have shown evidence of any serious complications caused by AO administration.
In this study, the intravenous administration of 1 mg/kg of AO by drip infusion for 1 hour did not cause any serious acute symptoms after any of the 23 treatment sessions. This strongly suggests that the intravenous infusion of a low concentration of AO may be safe for humans.
Effect of iAOR on human cancer. We previously performed in vitro and in vivo studies examining the cytocidal effect of a combination therapy of low-dose radiation and systemic AO administration on mouse osteosarcoma cells (10). Before the experimental study, we expected that AO could be excited by X-ray radiation and would kill osteosarcoma cells via active oxygen, which is the same mechanism as that used in PDT, because X-rays are composed of photons with a high energy and a very short wavelength. The results revealed that AO in combination with low-dose X-rays (5 Gy) killed osteosarcoma cells through the induction of apoptosis in vitro and inhibited tumor growth through the induction of tumor necrosis in vivo. This effect was inhibited by L-histidine, an inhibitor of active oxygen. Therefore, we concluded that AO has a tumor cytocidal effect when combined with X-ray radiation as well as light beams. We called this method radiodynamic therapy (RDT). Another group from the USA also reported that AO with 3 Gy of irradiation was significantly inhibited tumor cell growth in a radio-resistant chondrosarcoma cell line (26).

Magnetic resonance imaging findings of brain-invading lesion (arrow) of case 7 with parotid carcinoma before (A) and after (B) radiotherapy after intravenous administration of acridine orange.
In this human cancer study, we observed a mild anticancer effect of iAOR in three out of the five cases; one patient had recurrent cholangiocarcinoma after intensive chemotherapy and radiotherapy, one had brain-invading parotid cancer, and one had recurrent lung cancer after intensive chemotherapy, radiotherapy and surgery. However, in two patients with pancreatic cancer, no response was detected. Therefore, we cannot conclude that iAOR is an effective therapy against all human cancers types, although it does have the potential to kill cancer cells in humans, as suggested by the three severe cases that showed a mild response.
At present, we are examining the total dose of AO and the frequency or speed of injection based on an in vivo study in mice. A radiation intensity of 5 Gy delivered as one shot during three sessions over 3 weeks is quite low, compared with typical radiotherapy for cancer treatment. The optimal dose and frequency of AO injection and radiation treatment should be investigated.
Interaction between AO and radiation through autophagy. Autophagy has been recently demonstrated to be related to radioresistance and chemoresistance (27). Radiotherapy and chemotherapy activate autophagy in cancer cells, and autophagy accelerates DNA repair after DNA damage (25, 29) (Figure 5). In autophagy, autophagosomes form autolysosomes after the fusion of lysosomes to digest damaged proteins, lipids and DNA or RNA to supply amino acids, fatty acids and nucleic acids as recycled sources of cell components. The proteins P62 and LC3 II, which work to form autophagosomes, also have an important role in DNA repair (27) (Figure 7). Therefore, the inhibition of autophagy increases radiosensitivity and chemosensitivity. Since the fusion of lysosomes is a critical process of autophagy, the destruction of lysosomes inhibits autophagy. AO selectively accumulates in acidic lysosomes of cancer cells and destroys lysosomal membranes through the oxidation of activated oxygen produced by excited AO after light or X-ray exposure (PDT or RDT). In iAOR, the combination of AO and radiation destroys the lysosomes of cancer cells and inhibits the formation of autolysosomes, resulting in the inhibition of autophagy. X-ray radiation damages the DNA of cancer cells. Therefore, radioresistant cancer cells cannot repair their DNA and ultimately die because of apoptosis (Figure 8). Indeed, in this clinical study, two out of the three cases that responded to iAOR were radioresistant, since they had recurrent lesions after radiation therapy.
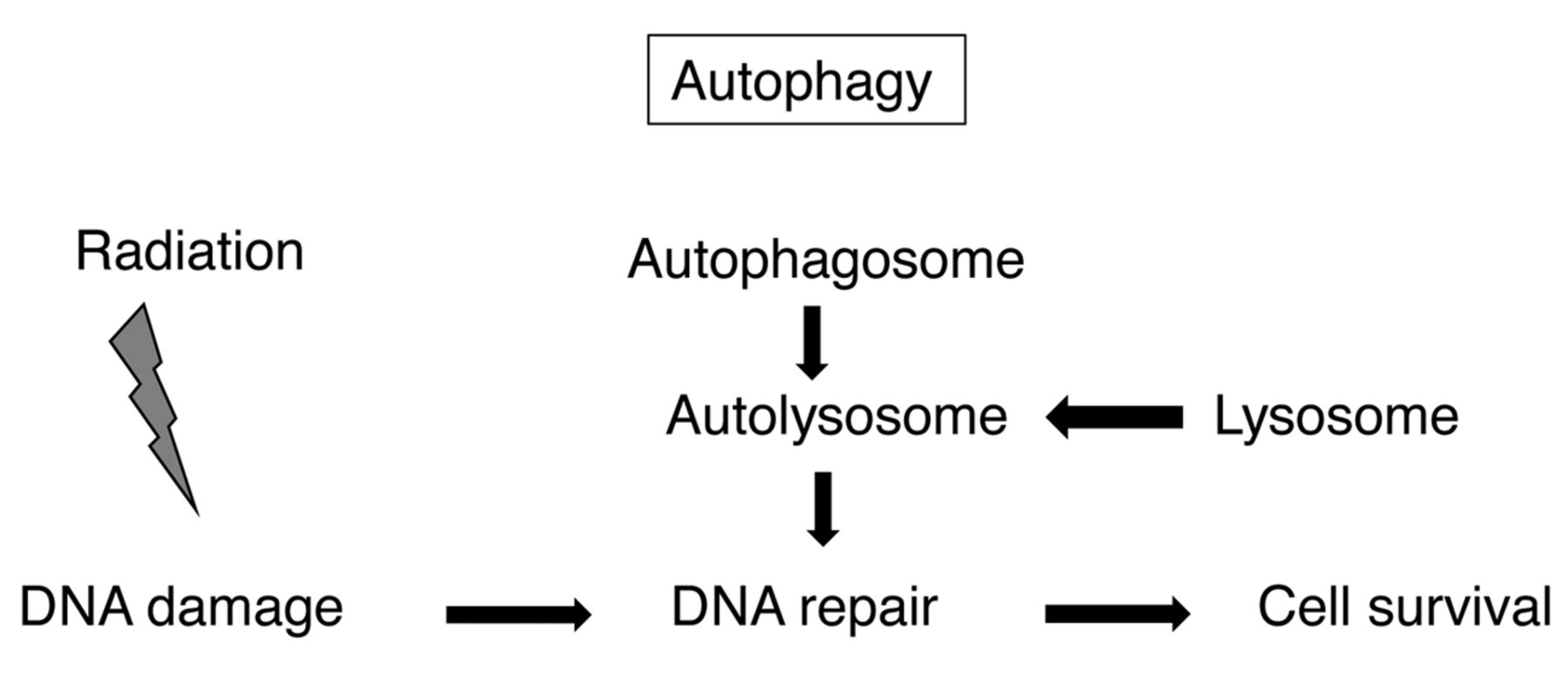
Mechanism of radioresistance related to autophagy.

Mechanism of radiotherapy after intravenous administration of acridine orange effect on radioresistant cells.
Chloroquine was recently reported as an autophagy inhibitor that enhances the radiosensitivity of cancer (30). Clinical studies using combination therapy with radiation and chloroquine or hydroxychloroquine for patients with brain metastasis or glioblastoma are presently underway at several institutions (31, 32). Chloroquine is a well-known fluorescent dye that accumulates in acidic lysosomes, similarly to the mechanism observed for AO (33). Therefore, the effect of chloroquine on the inhibition of autophagy probably resembles that of AO.
Conclusion
This pilot clinical trial showed that the intravenous infusion of AO is not toxic in humans. Patients with cholangiocarcinoma, parotid cancer and lung cancer, but not those with pancreatic cancer, responded to iAOR. This was the first trial of the systemic administration of AO in humans, providing evidence of the safety of AO. It also suggests that iAOR might be effective against radioresistant cancer.
AO is characterized by its selective accumulation in cancer cells, a strong cytocidal effect with light and X-ray irradiation, and the emission of fluorescence in response to blue light. We therefore believe that PDT and RDT involving the systemic administration of AO may become an innovative anticancer option, although more intensive clinical studies are needed.
Acknowledgements
This study was partially funded by a grant from the Italian Association for Cancer Research (#15608 to NB).
Footnotes
Conflicts of Interest
The Authors do not have any conflicts of interest to report in regard to this study.
- Received October 13, 2017.
- Revision received November 2, 2017.
- Accepted November 13, 2017.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}