


Abstract
Background/Aim: To maximize success rate for development of HER2-targeted therapeutics, patient-derived xenograft (PDX) models reflecting HER2-positive gastric cancer (HER2+ GC) patients were established. Materials and Methods: GC tissues obtained from surgery of GC patients were implanted into immune-deficient mice, and tumor tissue of HER2+ PDXs were verified of the patient-mimic HER2 expression by immunohistochemistry and explored for the feasibility by testing with Herceptin, the approved therapeutics and novel HER2 antibody therapeutics being developed. Results: We obtained 5 cases of HER2+ GC PDX models reflecting patient's GC tumor, consisting of 2 cases of HER2 3+ and 2 cases of HER2 2+. Novel HER2 antibody displayed significantly improved anti-cancer efficacy in combination with Herceptin. Conclusion: The HER2+ GC PDX models were successfully established to be utilized for preclinical evaluation of HER2-targeting drugs and combined therapies for GC treatment, as an ideal platform of personalized tools for precision therapy.
- Patient-derived xenograft
- gastric cancer
- human epidermal growth factor receptor 2
- personalized treatment
Conventionally, cancer cell lines and xenograft models have been used for drug screening and optimization of drug candidates for development of therapeutics. Nonetheless there have been huge efforts to develop effective treatment using those models, most novel anticancer agents have failed to reach clinical trials. According to the reports, cultured cell lines and xenografts cannot replicate identical primary tumor microenvironment including heterogeneity (1). Consequently, investigators evaluate patient-derived xenograft (PDX) models as personalized tools, to reflect the clinical relevance in various solid tumors including breast, ovarian, pancreatic, prostate, gastric cancer (2). PDX models maintain morphology, heterogeneity, and molecular properties of primary tumors (3, 4), which permit evaluation of tumor progression and response to therapy (5-7).
Gastric cancer (GC) is one of the most frequent human malignancies and the second predominant cause of cancer-related mortality worldwide (8-11). Surgical resection is considered the mainstay of resectable GC with possibly curable disease. However, even after curative surgery, recurrence rates are still high (11). Overexpression and amplification of the human epidermal growth factor receptor 2 (HER2) in variable cancer (12, 13) including GC that was first described in 1986, occurs in approximately 20% of GC (14-16). HER2 is associated with poor prognosis and recognized as a new diagnostic factor and novel therapeutic target in GC (15).
Trastuzumab (Herceptin), the monoclonal antibody against HER2 was shown to improve significantly the median overall survival after trastuzumab plus chemotherapy, compared to chemotherapy alone (13.8 vs. 11.1 months) in the Trastuzumab for Gastric Cancer (ToGA) trial (17-19). However, the overall tumor response rate of trastuzumab plus chemotherapy was reported to be 47% (19). For HER2-targeted therapy, diagnosis of HER2 status is required, but unfortunately HER2 scoring for diagnosis in patients is still controversial (20-22). Herein, we showed generation and characterization of patient-derived xenograft models accurately reflecting HER2+ GC patient. Moreover, we demonstrated the value of the HER2+ GC PDXs as clinically-relevant tools by evaluating novel HER2 antibody (Ab) with traditional HER2-targeting therapy such as trastuzumab and 1A12 (23, 24).
Materials and Methods
Patient and tumor samples. All animal experiments were performed following the protocol approved by the Institutional Animal Care and Use Committee of the Asan Institute for Life Sciences. Human gastric adenocarcinoma tissues were excised from five patients during surgery. A part of fresh specimen was transferred to medium-containing antibiotics immediately after surgical resection under sterile conditions, and transported to an animal facility within 2 h for implantation into mice. The other part was frozen in liquid nitrogen or fixed in 4% formaldehyde and embedded in paraffin at 56°C for histological evaluation.
Generation of gastric cancer PDX model. Five cases of gastric adenocarcinoma specimens were implanted to 6-week-old NOD-SCID mice (Charles River Laboratories, Wilmington, MA, USA) for the first passage. To produce the GC PDX models, a piece of tumor tissue in 3×3×3 mm3 size was implanted subcutaneously (s.c.) into flank. After about 3 months, when the tumor size reached to 500 mm3, the mice were anesthetized via an intra-peritoneal injection of a 40 mg/kg zoletil (Virbac, Virbac laboratories BP 27-06511 Carros, France) and 5 mg/kg Rumpun (Bayer, Korea, South Korea), and the tumors were surgically removed. The tumor was implanted again into male athymic nude mice (BALB/c-nude; 6 weeks old; Japan SLC, Hamamatsu, Japan) for amplification. After four consecutive passages in male athymic nude mice, the xenograft was considered to be used for examination of in vivo therapeutic efficacy, and full characterization including histopathological analysis, HER2 expression by IHC assays, genomic mutation detection.
Assessment of morphology and immunophenotype. To assess histological homogeny and maintenance of HER2 expression, the PDX tumor tissues of all passages were harvested, fixed in 4% paraformaldehyde, embedded in paraffin and sliced for histological analysis. The sections at a 5 micron thickness were observed under a microscope (DP71; Olympus, Tokyo, Japan) after staining with hematoxylin and eosin. For immunohistochemistry against HER2, immunohistochemical staining was done with anti-HER2/neu (4B5) (#790-4493; Roche, Republic of Korea), and analyzed under a microscope. The tumor tissues were counter-stained with hematoxylin, and then reviewed by pathologist to confirm the homogeny and scoring HER2 expression.
Patient profiles.
In vivo efficacy of Herceptin and new HER2 targeting antibody. The mice-bearing xenograft tumors grown to from 80 to 120 mm3 were pair-matched according to tumor volume into the number of experimental groups (n=5 or 7/group). The single or repeated dose of Herceptin (Trastuzumab, Roche, Republic of Korea), Perjeta (Pertuzumab, Roche, Republic of Korea) and 1A12, novel HER2 antibody (provided AbClon) (23, 24) were intravenously (i.v.) administrated through tail vein at 10 mg/kg, respectively, once a week for four weeks. The tumor volume and body weight were monitored during whole period of experiment. Tumor volume was calculated using the formula volume=(length × width2) × 0.5. The results were expressed as the mean±standard deviation. Relative tumor growth inhibition was calculated as T/C=(Ti-T0/Ci-C0), Ti and Ci represent tumor size of treatment and control group at the end of experiments respectively; T0 and C0 represent tumor size at initiation of experiments respectively (25). Objective response was defined by Response Evaluation Criteria In Solid Tumors (RECIST) as complete response; CR (disappearance of all target lesions), partial response; PR (at least a 30% decrease in longest diameter of target lesions), stable disease; SD (neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD), and progressive disease; PD (at least a 20% increase in target lesions) (26).
Statistical analysis. All data are presented as mean±SE from at least three separate experiments. The statistical analyses were performed using SPSS v12.0.1 software (SPSS). Mean values were calculated using T-tests and analysis of variance with Bonferroni correction. All p-values <0.05 were considered to represent significant differences.
Results
Establishment of PDX models and phenotypic comparison. All GC patients' samples were viable and led to growth in SCID mice after subcutaneous implantation, and continued to grow in nude mice after the second generation. Five GC tissues were used for this study and assessed after H&E staining and HER2 expression. Four male patients and one female patient, aged from 50 to 79 were collated (Table I). It was confirmed by immunohistochemical analysis that amplified tumor tissues formed in mice revealed the identical characteristics with original tumors. As shown in Figure 1, the xenograft tumor (Figure 1, right panel) had similar morphological features and HER2 expression to the original tumor (Figure 1, left panel). Two cases (11C94 and 12C63) were scored as strongly positive (3+) for HER2 staining and three cases were scored as moderately positive (2+). In addition, we identified via H&E staining that morphology of successive transplanted tumors tissue were identical (Figure 2) and finger printing via Next Generation Sequencing (NGS) shown matching rate of above 80% between original patient tissues and p5 PDX tissues (data not shown).
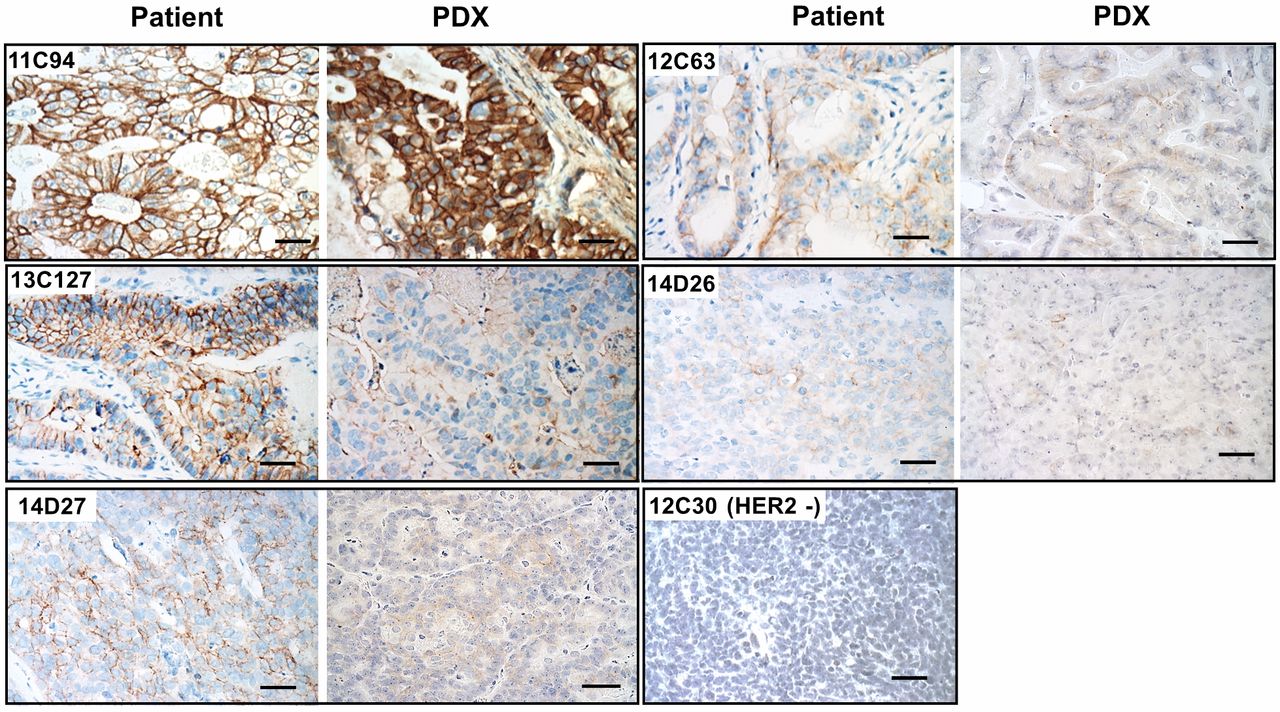
Immunophenotypic comparison of patient and PDX tumors. HER2 expression was performed by immunohistochemical analysis. HER2 expression was maintained in PDX tumor compared with primary tumor from patient. DAB images of immunohistochemically stained HER2 was obtained under a microscope. Scale bar, 10 μm.

Histological morphology of PDX tumor between P3 and P5. Histological features were identical between P3 and P5 in PDX tumors. Histological evaluation of PDX tumor was attended by hematoxylin & eosin (H&E) and analyzed under a microscope. Scale bar, 10 μm.

Trastuzumab anticancer efficacy in HER2+ GC PDX. Tumor growth delay curves. Mice bearing HER2+ GC patient's tumor of 5 cases were intravenously administrated with Herceptin at dose of 10 mg/kg once a week for four weeks. Tumor volumes and body weights were monitored during the experimental course. Tumor was removed at the end point and measured its weight. Data are represented as mean±standard deviation.

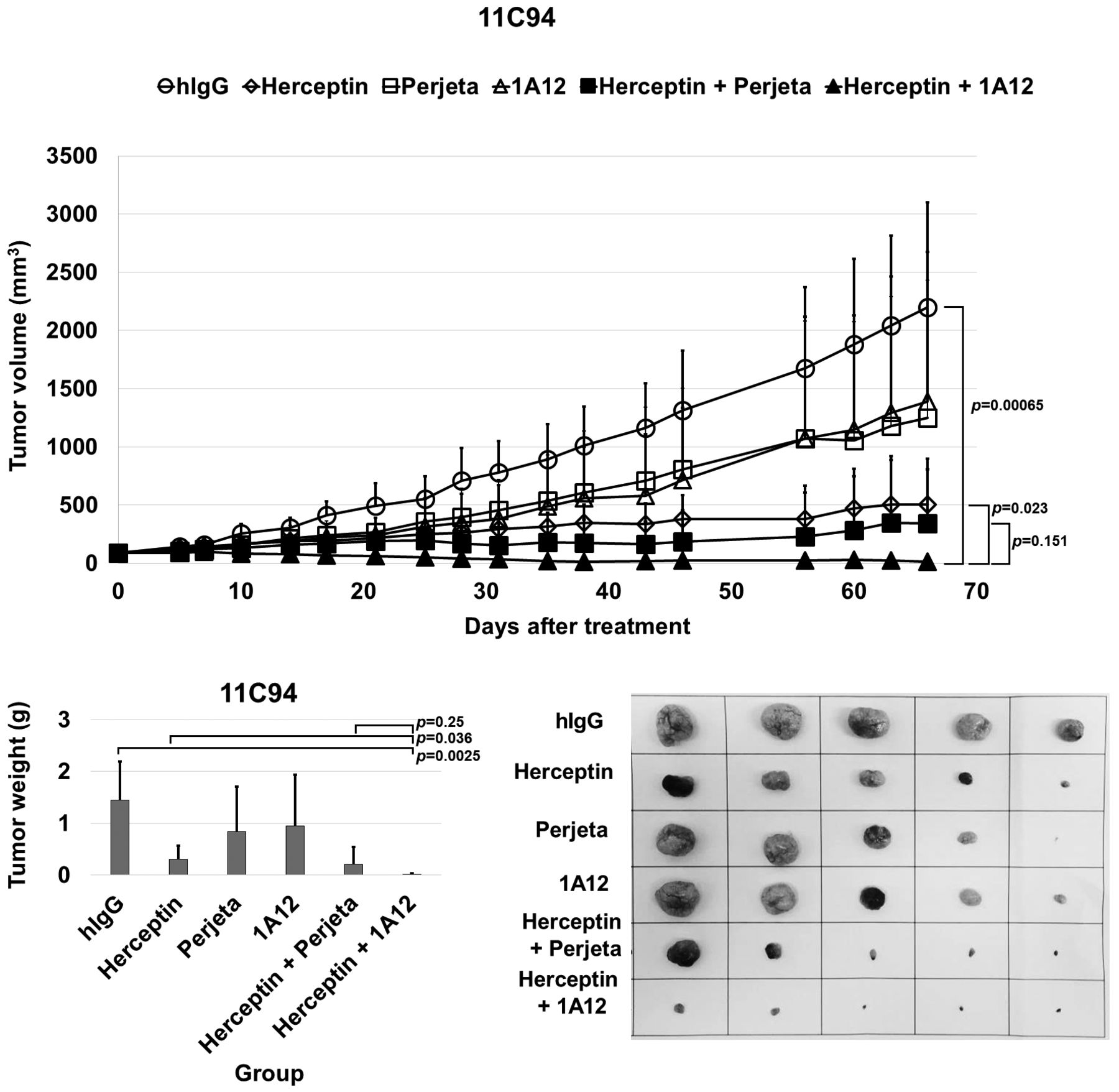
1A12 anticancer efficacy in IHC 3+ case. Tumor growth delay curves. Mice bearing HER2+ (IHC 3+) GC patient's tumor was intravenously administrated with Herceptin, Perjeta and 1A12 at dose of 10 mg/kg once a week for four weeks. Tumor volumes and body weights were monitored during the experimental course. Tumor was removed at the end point and measured its weight. Data are represented as mean±standard deviation.
Responses of individual GC PDX models to trastuzumab. To assess the PDX models as personalized tool, we evaluated in vivo anti-cancer effect of trastuzumab in all five HER2+ GC PDX models. The mice were i.v. injected with trastuzumab at repeated dose of 10 mg/kg once a week for four weeks. Two GC PDX models (IHC 3+) named 11C94 and 12C63 showed highly anti-cancer effect as 99.9 and 89.9% of tumor growth inhibition (TGI), respectively, whereas three GC PDX models (IHC 2+) named 13C127, 14D26, 14D27 did not reveal any therapeutic effect as 28.5, -20.5, 12.9% of TGI at the end point, respectively (Table II), (Figure 3). In addition, tumor volume and weight were dramatically decreased at the end point in two GC PDX models. As a result, HER2+ GC PDX according to HER2 expression was assessed with preclinical test of trastuzumab, and these results suggested that PDX model could be personalized tool for clinical relevance of novel drug candidate.
Evaluation of anti-cancer efficacy of new HER2 Ab in GC PDX models. Since we confirmed the feasibility of PDX models as personalized test, we next performed in vivo study of therapeutic effect by 1A12, novel HER2 antibody. The 1A12 bind to sub-domain IV of HER2-ECD (extracellular domain), and it has not overlap with epitope of trastuzumab. So, the 1A12 is developed by AbClon as combination therapy with trastuzumab for GC patient (23). The mice were i.v. injected with trastuzumab, perjeta and 1A12 at a repeated dose of 10 mg/kg once a week for four weeks. As shown in Figure 4 and Table III, TGI of Herceptin, Perjeta and 1A12-treated group were 80, 45, and 38%. The impact of trastuzumab plus 1A12 in 11C94, HER2+ (IHC 3+) GC PDX model was demonstrated, which remarkably increased TGI at 104% compared to conventional treatment (trastuzumab plus pertuzumab, TGI at 88%). Moreover, trastuzumab plus 1A12 resulted in CR of 60% (3/5) and PR of 40% (2/5) (Table III). Taken together, preclinical testing of novel candidate drug could be assessed via HER2+ GC PDX.
Tumor growth inhibition (TGI) of HER2+ GC PDX models.
Discussion
Recently, researchers have been developing PDX tumor models in variable cancer types because novel drug candidates proved of its efficacy in cancer cell line-based xenograft tumor models have been failed in clinical trials (1, 3, 4). In the present study, we established HER2+ GC PDX tumor models using gastric cancer tissues derived directly from patients and confirmed histological identity between original tumor of patient and PDX tumor tissue. Clinically, HER2+ GC occurs approximately 20%, and patients are diagnosed via histological methods (14, 15). All the established cases showed growth in athymic mice and maintenance of histological feature was confirmed by homology comparison. HER2 expression was analogous in PDX tumor with original tumors, also morphological feature was remained between generated PDX tumors. Furthermore, we evaluated HER2-targeting therapy using established HER2+ GC PDX model that result in difference of tumor growth inhibition according to HER2 scoring. Especially, HER2+ (IHC 3+) cases were revealed remarkable antitumor effect as low T/C value (Figure 3). In addition, we assessed 1A12 in vivo efficacy in HER2+ (IHC 3+), and demonstrated a dramatic tumor growth inhibition as CR with PR of 100 % (p=0.023, Herceptin vs. Herceptin plus 1A12) (Figure 4 and Table III). Taken together, our results suggest that HER2+ GC PDX could be a personalized tool and could improve preclinical testing for successful clinical trials of novel drug candidate.
Tumor growth inhibition (TGI) and RECIST in HER2+ (IHC3+) GC PDX.
Because of the lack of appropriate models for new drug development, we generated PDX models reflecting the patient's tumor microenvironment and examined it with the conventional treatments and novel drug candidate, while demonstrating the potential of PDX models for the development of personalized treatment. We strongly expect that the PDX models should be effectively utilized to predict anti-cancer agents responsiveness for precision medicine, ultimately leading to improved patient survival rates.
Acknowledgements
This research was supported by grants from the Korean Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by Ministry for Health and Welfare, Republic of Korea (HI06C0868 and HI15C0972), the National R&D Program for Cancer Control, Ministry of Health & Welfare, Republic of Korea (15201101), Korea Drug Development Fund (KDDF), Republic of Korea (KDDF-201408-02), and the grant (2017-445) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea.
Footnotes
Conflicts of Interest
The Authors disclose no conflicts.
- Received August 31, 2017.
- Revision received October 24, 2017.
- Accepted November 2, 2017.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}