


Abstract
Patients with brain metastases (BRM) generally have a poor prognosis with infrequent long-term outcomes. Four patients treated by stereotactic radiosurgery (SRS) for BRM between 2000 and 2010 with a minimum follow-up of 10 years are described. The mean age was 43.5 years, and these individuals exhibited good performance status at the time of diagnosis of intracranial disease. BRM was solitary or multiple, and the primary malignant tumor originated from the thyroid gland, lung, mediastinum or large intestine. Progression of the original and secondary tumors subsequent to diagnosis and SRS was not observed. Radioimaging of the brain obtained 9 years later in one of the patients who was asymptomatic at follow-up revealed white matter changes; BRM in this individual was treated by tumor resection and cranial irradiation prior to SRS. We contend that extended longevity is not precluded when standard management of BRM is practiced in selected cases.
Neoplastic spread to distant sites is always indicative of progression of underlying disease, limiting the chances for survival. Brain metastases (BRM) represent an important cause of morbidity and mortality. The aim of therapeutic intervention in patients with BRM is improved quality of life and longevity. Very few studies of individuals with BRM have described extended prognosis (1). Thus, we report our four cases of prolonged (>10 years) survival after radiosurgery of BRM.
Patients and Methods
This retrospective study is an Institutional Review Board-approved outcome study (#644). From March 2000 to October 2010, 132 patients underwent gamma knife radiosurgery (GKRS) for BRM that had been identified via imaging or documented histologically. Of these, 11 were excluded because they were lost to follow-up. A determination of longevity periods was performed of the remaining 121 individuals. Twenty-nine patients (24%) survived for 3 months or less following radiosurgery. Survival ranged from 4 to 36 months in 82 patients (68%). Ten individuals (8%) had lifespans between 37 and 144 months; four patients in this subgroup who were followed for a duration exceeding 120 months are the subjects of this report (Table I).
Results
The mean age was 43.5 years and included three men and a woman. The primary malignant tumors of the thyroid gland, mediastinum, lung and colon, which were stable or under control, preceded BRM GKRS by an average of 62.8 months (range= 1-237 months). BRMs were manifested clinically as headache episodes, memory impairment and functional hemiparesis. Metastatic disease in the brain was solitary or multiple, and the intracranial locations were in the frontal, parietal, temporal and occipital lobes. The Eastern Cooperative Oncology Group performance status scores at the time of GKRS were 1 or 2. Prior to craniotomy and tumor debulking followed by radiosurgery (in case 2), the patient received fractionated whole-brain external beam radiotherapy of 30 Gy given in 10 fractions; the other three individuals did not receive cranial irradiation. The mean target volume for radiosurgery was 9.9 cm3 (range=5.9-14.6 cm3), while the mean target size was 1.7 cm (range=1.5-2.9 cm). The average number of isocenters used was three (range=1-7 isocenters). The margin dose varied between 14 and 16 Gy. There was no occurrence of later BRM progression requiring repeat GKRS. At 108 months following radiosurgery, previous cranial surgery and whole-brain irradiation in case 2, magnetic resonance imaging (Figure 1) revealed grade 2-3 periventricular white matter changes according to the University of Virginia grading system (2). The leukoencephalopathy was not associated with clinical neurological decline, although, admittedly, a formal neurocognition evaluation was not performed.
Details of long-term survival after gamma knife radiosurgery (GKRS) of brain metastases.
Discussion
Only about 1.2% of all patients with BRM live 10 years or longer (1). This retrospective review of cases reflects clinical experience in the treatment of adults with BRM using GKRS at a single institution over a 10-year time period. Our study confirms some clinical findings observed in a prior investigation (1), that may partially explain the prolonged survival of the studied individuals. Firstly, long-term survival was most common among individuals younger than 60 years. Secondly, the performance status at the time of BRM detection had generally been satisfactory and the primary neoplasm was controlled. Thirdly, metastatic disease in the brain was often solitary. The onset of BRM varied from as early as 1 month to as late as 232 months after the diagnosis of the primary malignancy. Fourthly, management of secondary spread to the brain involved metastatic tumor resection and stereotactic radiosurgery (3).
Studies have validated the link between white matter changes, seen via magnetic resonance imaging, and decreased neurocognitive function (4-8). Although radiation-induced leukoencephalopathy is known to increase steadily over time, it is not yet clear to what extent such white matter changes impact on neurological function (2). Neurocognition and quality of life are critical to defining successful outcome of applied therapy and should be assessed as part of long-term care of patients with BRM (1). These endpoints are challenging to study as emphasized in the small number of patients who become long-term survivors. Reported 5-year survival rates following stereotactic radiosurgery have ranged from 3% to 21% (3, 9-12).
The heterogeneous clinicopathological features of individual patients and additional unidentified factors (e.g. biological differences between tumor types) preclude an adequate explanation for the prolonged lifespan in this case series. The challenge for oncologists will be in the identification of this subgroup of patients. From this perspective, we can only speculate that aggressive therapy may be warranted when known favorable clinical features (e.g. good performance status, younger age, absence of disseminated cancer and the presence of oligometastases) are present in individuals with BRM.
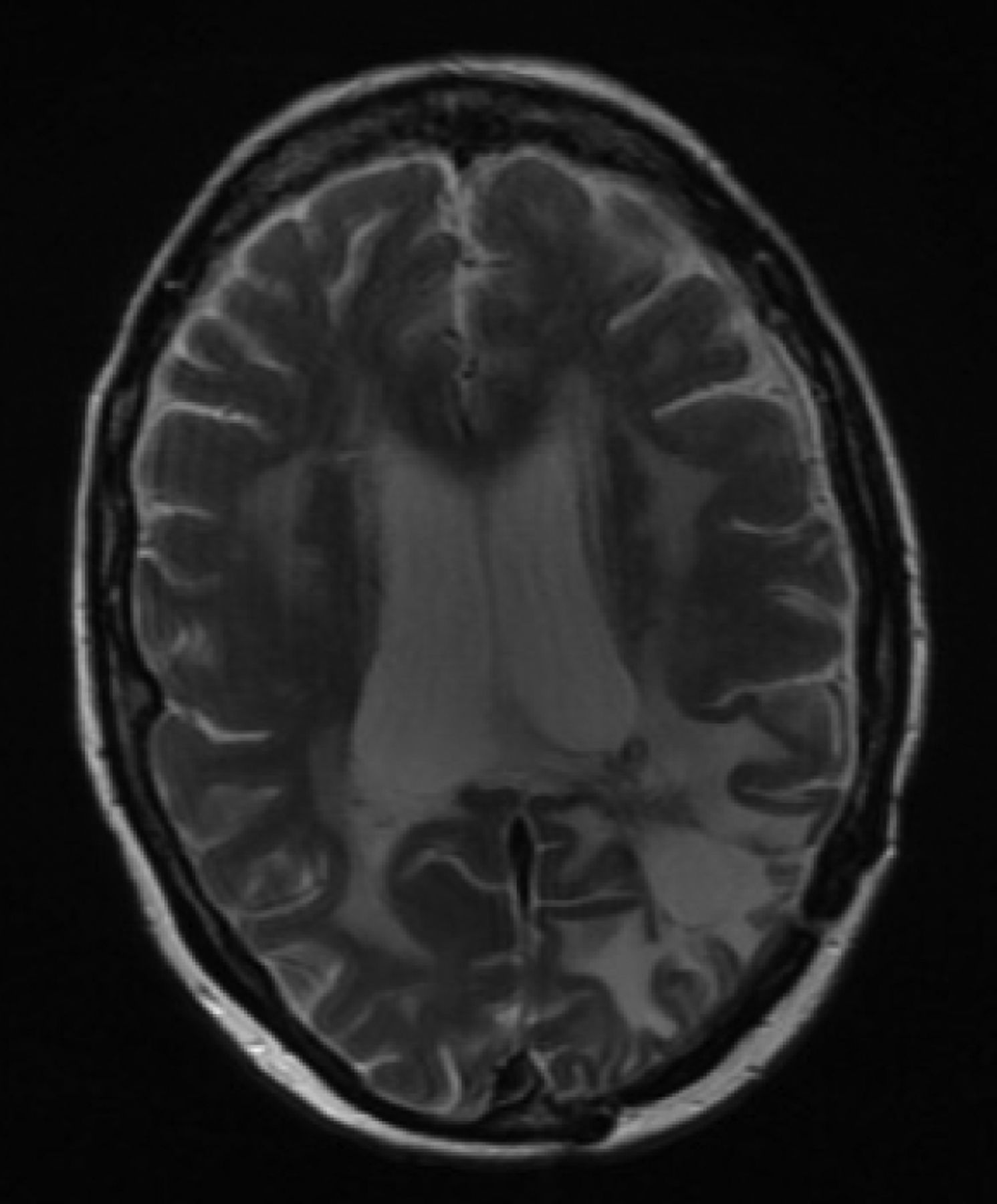
Axial T2-weighted magnetic resonance imaging at 108 months after whole-brain irradiation and radiosurgery (in case 2) shows moderately severe periventricular white matter changes.
The limitations of this report (e.g. the retrospective design, small sample, and the absence of a neurocognition evaluation in our patient with post-radiosurgery radiographic leukoencephalopathy) notwithstanding, our finding of extended longevity in these patients underscores the worthwhile practice of modern day management of BRM using GKRS. Despite the usefulness of multiple relevant prognostic factors (13, 14), the generation of evidence-based guidelines is essential to assist practitioners in utilizing available prognostic indices towards patient care decision making (15).
- Received June 16, 2017.
- Revision received July 9, 2017.
- Accepted July 11, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Established Serum Biomarkers Are Prognostic Factors in Patients With Oligometastatic Cancer and Brain Involvement
- Confirmatory Analysis of QUARTZ Study Results: Survival Prolongation After Whole-brain Radiotherapy
- Serum Lactate Dehydrogenase Contributes to Prognostic Assessment in Patients With Oligometastatic Cancer and Brain Involvement
- Patterns of Treatment and Outcome in Patients With 20 or More Brain Metastases
- Validation of a Survival Score for Patients Receiving Radiosurgery or Fractionated Stereotactic Radiotherapy for 1 to 3 Brain Metastases