


Abstract
Colorectal cancer is the most common cancer of the gastrointestinal system and has a marked preference to metastasize to distant organs. In this study, we investigated whether levels of circulating serum pro-angiogenic cytokine such as chemokine (C-X-C motif) ligand 1 (melanoma growth-stimulating activity, alpha; CXCL1) and vascular endothelial growth factor (VEGF) have a role in favoring the colonization of metastatic cells at preferential sites and determined their prognostic significance in a cohort of 103 patients with metastatic colorectal cancer. Importantly, we found that the presence of elevated circulating levels of VEGF and CXCL1 are predictive of liver and lung metastasis, respectively. Moreover, the presence of a high serum VEGF level represents a negative prognostic factor for patients with liver metastases, with a worse prognosis than patients with lung metastasis. This suggests an additional role for circulating cytokines as a predictive tool for cancer prognosis and diagnosis, as well as for assessment of tumor sensitivity to anticancer therapy.
Similarly to other types of tumor, colon cancer also metastases to preferential organs. More than 70% of patients with colorectal cancer have liver metastases. The lung is the second most important organ for colorectal carcinoma metastasis, and 20 to 30% of all distant colorectal carcinoma metastases are found primarily in the lung (1, 2). According to ‘the seed and soil theory’, postulated by Stephen Paget in 1889, there is a propensity for certain tumors to seed to particular organs (3, 4). A tumor cell becomes metastatic by establishing interactions with homeostatic factors in a target organ, thus promoting cell survival, angiogenesis and tumor growth. These steps are mediated by specific adhesive interactions between cancer cells and the host organ microvasculature (5, 6). Recent studies have demonstrated the presence in the target organs of specific molecules that include chemokines, growth factors and adhesion molecules that interact with receptors or ligands present on tumor cells that together contribute to the formation of organ-specific metastasis (7-9).
The formation of new blood vessels is determined by the secretion of pro angiogenic factors by tumor cells. Vascular endothelial growth factor (VEGF) is the most important modulator of tumor angiogenesis and performs important activities including reducing the functions of the biological barrier and regulating endothelial sprouting (10, 11). It also increases vascular permeability and, through VEGF–vascular endothelial growth factor receptor (VEGFR) interactions, allows the mobilization and recruitment of endothelial cells within tumors. Many published studies show that VEGF plays an important role in the development of colon cancer, especially in the stimulation of angiogenesis (12, 13). Given that VEGF is expressed in various types of tumors, determination of circulating levels of VEGF could provide a diagnostic method of great use in patients with cancer (14). An increase in VEGF expression in tumour tissue or blood compartments (i.e. serum or plasma) has been found in solid and hematological malignancies of various origins and is associated with metastasis formation and poor prognosis (15, 16). By multivariate analysis of molecular markers for detection of liver metastases after surgery in patients with colorectal cancer, it was demonstrated that a combination of markers such as carcinoembryonic antigen (CEA), epidermal growth factor receptor (EGFR) and VEGF could be an effective method for predicting liver metastases in patients with colorectal cancer (17).
Chemokines such as chemokine (C-X-C motif) ligand 1 (melanoma growth-stimulating activity, alpha; CXCL1) are intricately associated with cellular transformation, tumor growth and increase of invasive potential (18, 19). Many chemokines, including CXCL1, are strong inducers of chemotaxis and there are several lines of evidence showing that they play a role in tumor progression, for example, by increasing metastasis formation in preferential target organs (20-23). In this study, we investigated whether levels of circulating serum cytokine such as CXCL1 and VEGF have a role in favoring the colonization of metastatic cells to preferential sites and determined their prognostic significance in patients with metastatic colorectal cancer.
Patients and Methods
Patients and blood samples. The group of patients examined in this study is the same as reported in a previous work (24). In short, in this analysis,103 patients, 65 male and 38 female, with median age 65 (range=39-82) years who underwent curative hepatic and pulmonary metastases from colorectal cancers treatable with resection or tumor ablation were enrolled in this prospective study at the Giovanni Paolo II National Cancer Institute, Bari Italy. Patients with synchronous liver or lung metastases were included if the resection of metastases was performed together with that of the primary tumor.
A total of 69 patients (67%) had liver metastases, while 34 (33%) had lung metastases; 30 patients (29.1%) had synchronous metastasis, while 73 patients (70.9%) had metachronous metastasis. Only five patients (4.8%) had synchronous presentation of liver or lung metastasis. A total of 47 patients (45.6%) had solitary metastasis and 58 patients (56.3%) had unilobular distribution of metastasis. The clinical characteristics of patients (age, sex, therapeutic interventions, etc.) were obtained from medical records. In accordance with national and institutional standard procedures, all patients received systemic therapy: 35 patients underwent neoadjuvant chemotherapy, and 68 patients received neoadjuvant bevacizumab treatment. Blood samples were taken on the day of diagnosis from newly diagnosed patients with synchronous metastasis or from patients who developed metastases metachronously after R0-resection of the primary tumor. For analysis of cytokines, 5 ml of peripheral blood were collected in a vacutainer system and serum was immediately separated from the cellular fraction by centrifugation at 1,500 × g for 10 min and frozen at −20°C. Blood samples from 50 healthy individuals were used as negative controls. Written consent was obtained from all patients prior to enrolment in the study and the Ethical Committee of the Institute approved the protocol in accordance with the ethical guidelines of the 1975 Declaration of Helsinki.
CXCL1 and VEGF enzyme-linked immunoassay (ELISA). Serum samples from patients and healthy donors were assayed for levels of CXCL1 and VEGF by a sandwich ELISA assay (Quantikine Human CXCL1 and VEGF Immunoassay; R&D Systems, Inc., Minneapolis, USA) according to the manufacturer's recommendations. The absorbance of the solution produced was measured at 490 nm and was directly proportional to the amount of CXCL1 and VEGF present in the sample. A standard curve was constructed by plotting the mean absorbance value measured for each standard versus its corresponding concentration. The minimal detection limit was 10 pg/ml for CXCL and 1.5 pg/ml for VEGF.
Statistical analysis. The association between serum levels of CXCL1 and VEGF with clinical characteristic of patients was analyzed with unpaired t-test and ANOVA. Spearman's correlation was used for the correlation analysis, and the survival analysis was evaluated with Kaplan–Meier and log-rank test. Overall survival (OS) was defined as the time between the date of the blood sample draw and the date of death or the last follow-up examination. A p-value of 0.05 or less was taken to indicate statistical significance. All statistical analyzes were performed by Number Cruncher Statistical System-Power Analysis and Sample Size Software 2007 NCSS-PASS, (Statistical Analysis and sample Size – Power Analysis and Graphics, Kaysville, UT, USA).
Correlation between circulating cytokines and clinicopathological variables in patients with metastatic colorectal cancer.
Results
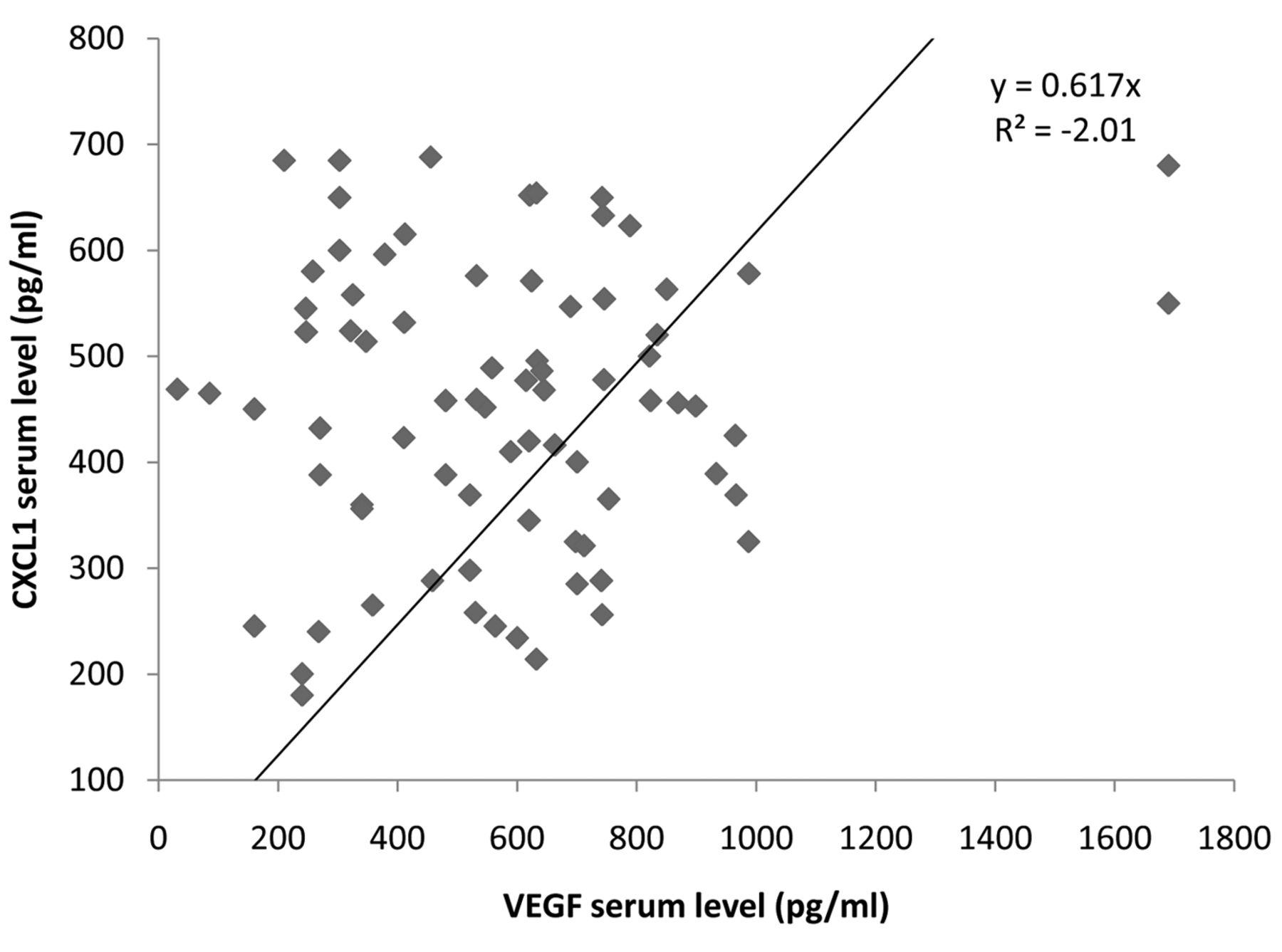
Association between circulating levels of cytokines and clinicopathological parameters. The serum levels (mean±SD) of CXCL1 and VEGF are reported in Table I. The mean values of these cytokines were much higher in patients than in healthy donors (p=0.0001, ANOVA). A significant association between female gender and circulating levels of VEGF was found (p<0.0001). Considering serum levels of the two cytokines according to metastatic site, we interestingly noted that higher serum levels of VEGF were associated with the presence of liver metastases (p=0.004), while higher levels of CXCL1 were associated with the presence of lung metastases (p=0.001). Lastly, levels of CXCL1, in contrast to VEGF, were inversely associated with synchronous metastases (p=0.008 for CXCL1 and p<0.0001 for VEGF).Therefore, we evaluated the correlation between these cytokines. As shown in Figure 1, in our analysis, we found significant positive correlation between CXCL1 and VEGF (Spearman correlation, p<0.0001).
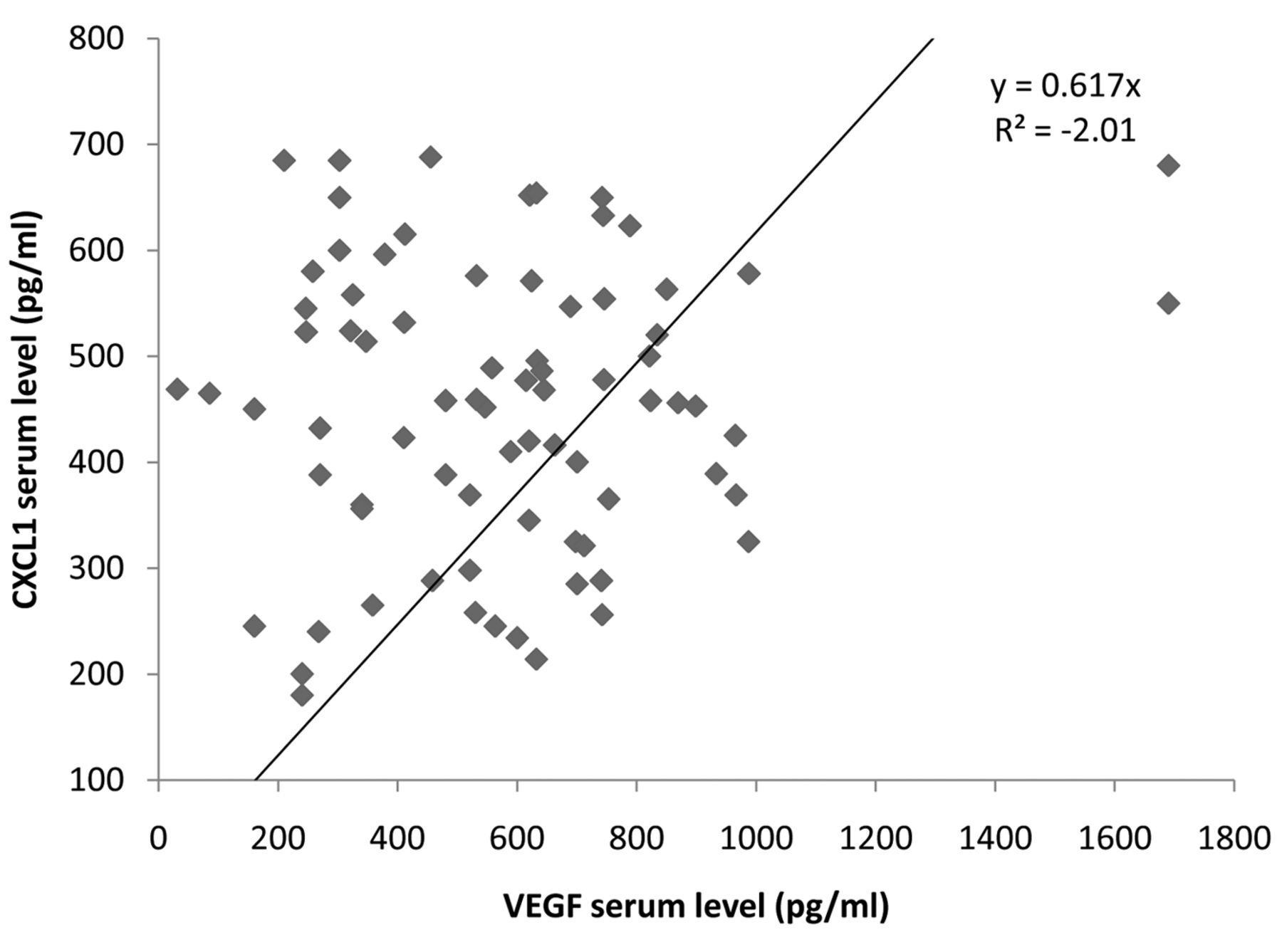
Scatter plot showing the correlation between serum levels of vascular endothelial growth factor (VEGF) and chemokine (C-X-C motif) ligand 1 (CXCL1). Spearman correlation, p<0.0001.
Higher serum VEGF is associated with worse prognosis in patients with liver metastasis. For patients overall, the median OS was 24 months as shown in Table II. Multiple variables such as gender, time of metastasis and metastatic site affecting survival were examined by univariate analysis using the log-rank test. Univariate log-rank analysis showed that shorter survival was observed in males than in females (20 vs. 26 months, respectively, p<0.004). Moreover, patients with metachronous metastases had a poorer prognosis compared with patients with synchronous metastasis, with median OS of 20 months versus 25 months (p<0.003). Finally, a shorter survival was associated with hepatic metastasis, with a median OS of 17 versus 24 months (p=0.02) for patients with pulmonary metastasis.
We, therefore, established a cutoff value for CXCL1 (410 pg/ml) and VEGF (500 pg/ml) by receiver operating curve analysis. Considering survival according to the two cytokines, patients with VEGF higher than the cutoff value of ≥500 pg/ml had a worse prognosis than patients with lower values (17 vs. 25 months, p<0.0001). Furthermore, patients with values of CXCL1 higher than the cutoff of ≥410 pg/ml had a worse prognosis than patients with lower values (22 vs. 26 months, p=0.02).
Mean (range) overall survival (OS) in correlation to gender, time of metastasis, metastatic site and serum vascular endothelial growth factor (VEGF) and chemokine (C-X-C motif) ligand 1 (CXCL1) levels.
Discussion
Metastases are the result of a complex cascade of events that begins with the detachment of tumor cells from the primary site and their reaching distant organs where they proliferate and form secondary tumor foci. During their stay in the bloodstream, tumor cells undergo a series of events that are regulated by an interaction of molecules secreted by both tumor cells and host cells and that will define the phenotypic fate of tumor cells (25). The formation of microvessels around the tumor is mediated by the presence of various angiogenic growth factors secreted by tumor cells (23). VEGF is one of the most powerful endothelial growth factors and acts by stimulating mitogenesis of endothelial cells; it is also considered one of the strongest factors promoting angiogenesis in colorectal cancer (26). In patients with colorectal cancer, VEGF levels are enhanced and provide an index of disease spread and prognosis (27, 28). Several studies have shown that angiogenesis is a negative prognostic factor for both overall and disease-free survival in patients with colorectal cancer (29). Most malignant tumors display an organ-specific metastatic pattern. For example, colon cancer cells preferentially colonize the lungs and liver, where they will develop metastases (30, 31). In other organs such as bone or brain, it is rare to observe the presence of colorectal cancer metastasis.
In this study, we have shown that the presence of higher circulating levels of pro-angiogenic cytokines VEGF and CXCL1 may be useful predictors of occurrence of liver and lung metastases, respectively, in patients with colorectal cancer, confirming that colon cancer cells preferentially target the liver and the lung to establish secondary tumors. We have also shown that VEGF is a biomarker of adverse prognosis in those patients who developed liver metastases. In fact, our study has shown that the presence of a high serum VEGF level in patients with liver metastasis was associated with reduced survival rate compared to those who developed pulmonary metastases. From these data, we can hypothesize that during their time in the circulation, cancer cells undergo various transformations taking on various phenotypes that predispose them to colonizing certain organs rather than others. In this case, high circulating levels of VEGF in patients with liver metastases suggests that the liver is an organ where metastatic cells appear to be phenotypically more aggressive than those that have colonized the lungs.
Organoselectivity is mediated by molecular factors such as chemokines and cytokines that are released into the microenvironment both from host cells and cancer cells (32, 33). In fact, it is thought that it is precisely the interaction between the cytokine receptors present on tumor cells and the ligands of the target organs which modulates the organotropism of metastasis. Constitutive expression of CXCL1 and its receptor CXCR2 was reported to regulate cell proliferation and invasive phenotype in colorectal cancer cell lines (34). In a study by Massague et al. that compared the genetic pattern of breast cancer cell lines with weak or strong metastatic tropism for the lung, CXCL1 was certainly one of the genetic products that promoted pulmonary metastasis (35). In our study, we confirmed that the expression of chemokine CXCL1 facilitates cell seeding and outgrowth of metastases at distant sites. CXCL1 also plays an important role in the recruitment of cancer cells to the lung in patients with metastatic colon cancer (36). This could open up new treatment opportunities to destroy tumor metastases by creating drugs that target chemokines or their receptors. Although CXCL1 promotes tumor cell growth and is involved in angiogenesis of several cancer types in animal models, its role in human cancer needs to be clarified. Although correlations can be found between the primary tumors and their preferential metastatic sites, there is not yet a rationale underlying organ preference.
A genetic fingerprint indicating which genes play a significant role in the metastasis of primary tumors preferentially to specific organs has been identified (37). Deeper knowledge about the mechanisms that govern the link between genes and the fate of metastatic cells could present an opportunity for improved patient care and for the prevention of many deaths from cancer.
Footnotes
Conflicts of Interest
The Authors declared that they have no competing interests with regard to this study.
- Received June 9, 2017.
- Revision received June 30, 2017.
- Accepted July 6, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Vascular Endothelial Growth Factor Family and Head and Neck Squamous Cell Carcinoma
- Elevated Preoperative Serum Vascular Endothelial Growth Factor Does Not Predict Poor Outcomes in Curatively Resected Non-metastatic Colorectal Cancer Treated Without Neoadjuvant Therapy
- Cytokines in the Urine of AKI patients regulate TP53 and SIRT1 and can be used as biomarkers for the early detection of AKI
- Celecoxib as an adjuvant to chemotherapy for patients with metastatic colorectal cancer: A randomized controlled clinical study
- An Autocrine Role for CXCL1 in Progression of Hepatocellular Carcinoma
- Chemokine (C-X-C motif) ligand 1 is associated with tumor progression and poor prognosis in patients with colorectal cancer