


Abstract
Background: Patients with ovarian cancer with high levels of heparin-binding epidermal growth factor-like growth factor have a poor prognosis. Here we assessed the pharmacokinetics and tumour-inhibiting effects of cross-reacting material 197, produced commercially as BK-UM, and examined the efficacy and safety of its intravenous (i.v.) administration. Materials and Methods: BK-UM was administered to rats, and its serum levels were measured. Ovarian cancer cell lines were either intraperitoneally (i.p.) or subcutaneously administered into mice, to establish a mouse model of ovarian cancer. BK-UM was then administered i.p. or i.v., and its tumour-inhibiting effects were examined. Results: Higher maximum serum concentration (Cmax) values resulted from i.v. administration, whereas longer time to maximum serum (Tmax) values resulted from i.p. administration. In the peritoneal dissemination model, i.p. administration inhibited tumour growth and increased survival rate, whereas in the subcutaneous model, i.v. administration significantly inhibited tumour growth compared to i.p. administration. Conclusion: Administration of BK-UM by i.v. is both efficacious and safe.
Ovarian cancer is a lethal gynecological malignancy that has an extremely poor prognosis due to the spread of cancer cells to the peritoneal cavity (1). Accumulating evidence indicates that the peritoneal fluid is a rich source of growth factors, termed ovarian cancer-activating factors (OCAFs), which promote the survival and proliferation of ovarian cancer cells (2). We reported that heparin-binding epidermal growth factor-like growth factor (HB-EGF) is the most widely expressed OCAF and plays a pivotal role in ovarian cancer progression (3, 4). Thus, we consider HB-EGF to be a therapeutic target for the treatment of ovarian cancer (5).
HB-EGF is an epidermal growth factor receptor (EGFR) ligand (6) that is initially synthesized as a transmembrane protein (pro-HB-EGF) and is then cleaved by a protease at the cell surface to yield the mitogenically-active soluble form of HB-EGF via ectodomain shedding (7). Because soluble HB-EGF is essential for the formation of some tumours, it may serve as a therapeutic target for many types of cancer, including ovarian (3, 8), gastric and breast cancer (4, 9, 10).
Pro-HB-EGF also functions as a diphtheria toxin (DT) receptor. Cross-reacting material 197 (CRM197), which was recently produced commercially as BK-UM, is a non-toxic mutant form of DT (11). BK-UM inhibits the mitogenic action of HB-EGF. It binds to both the pro- and soluble forms of human HB-EGF, thus inhibiting the binding of HB-EGF to EGFR (12). We reported that the intraperitoneal (i.p.) administration of BK-UM was effective in a mouse xenografted tumour model (13). However, no preclinical studies have investigated the effects of the intravenous (i.v.) administration of BK-UM. Therefore, this study aimed to evaluate the effects and safety of i.v. administered BK-UM.
Materials and Methods
Reagents. BK-UM was obtained from the Research Institute for Microbial Diseases, Osaka University (Osaka, Japan).
In vivo pharmacokinetic studies. Healthy male or female Sprague–Dawley rats (8-9 weeks of age) weighing 217-345 g were purchased from Charles River Laboratories Japan Inc. (Yokohama, Japan). The animal protocol was approved and designed according to the guidelines of the Animal Care Committee of TECHNOPRO R&D (Tokyo, Japan) (Approval No. 2014-0005). The rats were assigned randomly into two groups (males: n=7; females: n=7). The groups were administered 5 mg/kg or 50 mg/kg BK-UM i.v. or i.p. Blood samples (100 μl) were obtained from the tail vein of each rat at 1, 3, 6, 9, 24 and 48 h after i.v. or i.p. administration. Plasma samples were obtained after centrifugation for 15 min at 5,000 × g immediately after collection and stored at −80°C until analysis of BK-UM concentration. Plasma concentrations of BK-UM were determined by enzyme-linked immunosorbent assay (ELISA); ELISA plates (GREINER, Tokyo, Japan) were coated with an anti-DT monoclonal antibody to capture BK-UM (CRM197), followed by the addition of the diluted plasma sample obtained from each rat and a horseradish peroxidase-labelled monoclonal antibody against DT. The concentration of BK-UM was derived by parallel line assay method.
Cells and cell culture. A human ovarian cancer cell line, ES-2, was obtained from the American Type Culture Collection (Manassas, VA, USA). Cells were cultured in RPMI-1640 medium supplemented with 10% fetal bovine serum (ICN Biomedicals, Irvine, CA, USA), 100 U/ml penicillin G and 100 μg/ml streptomycin (Invitrogen, Carlsbad, CA, USA) in a humidified atmosphere with 5% CO2 at 37°C.
In vivo antitumour effects of BK-UM in the peritoneal dissemination model. ES2 cells expressing firefly luciferase (ES2-Luc cells) were used for the peritoneal dissemination model. Subconfluent cells were detached from culture plates with trypsin–EDTA. A total volume of 250 μl containing 1×107 cells suspended in serum-free RPMI-1640 was i.p. administered to 5-week-old female NOD/SCID mice (Charles River Laboratories Japan Inc., Yokohama, Japan). To assess the inhibitory effects of BK-UM on tumour growth, 50 mg/kg BK-UM or saline as control was administered i.v. or i.p. to tumour-bearing mice (n=6 per group) for 5 days. The inhibitory effects of BK-UM were assessed using the IVIS imaging system weekly (IVIS Lumina LT, SPI, Tokyo, Japan) after an i.p. administration of luciferin (Dojindo, Kumamoto, Japan). Each image was displayed as a pseudo-coloured photon image superimposed on a grayscale anatomical image. To quantify the amount of emitted light, regions of interest (ROI) were defined. Survival curves were also assessed using Kaplan–Meier method.
In vivo antitumour effects of BK-UM in the subcutaneous model. Subconfluent ovarian cancer cells were detached from plates with trypsin–EDTA. A total volume of 250 μl containing 1×107 cells suspended in serum-free RPMI-1640 was subcutaneously administered to either 5-week-old female NOD/SCID or 5-week-old nude mice (Charles River Laboratories Japan Inc.). To assess the inhibitory effects of BK-UM on tumour growth, 50 mg/kg BK-UM was administered i.v. or i.p. to tumour-bearing mice on two different treatment schedules after the tumour reached an estimated volume of greater than 100 mm3. The first treatment schedule was daily administration of 50 mg/kg BK-UM or saline as control for 5 days. The second treatment schedule was weekly administration of 50 mg/kg BK-UM or saline as control for 4 weeks. There were six mice in each goup. The tumour volume was estimated weekly based on two-dimensional tumour measurements as follows: tumour volume (mm3)=(length×width2)/2. The animal protocol was approved and designed according to the guidelines of the Animal Care of Fukuoka University (Approval No. 1306662) and our Ethics Committee.
Statistical analysis. The statistical significance of differences among the groups was assessed using the Mann–Whitney U-test. A p-value less than 0.05 was considered statistically significant.
Results
Intravenous administration of BK-UM increases Cmax and shortens Tmax. Rats were given BK-UM by either i.p. or i.v. administration, and blood was collected from the tail vein after 1, 3, 6, 9, 24 and 48 h. Serum concentrations of BK-UM were measured by sandwich ELISA. At a dose of 5 mg/kg, the maximal blood concentration (Cmax) was 1.05 U/ml after i.p. administration and 5 U/ml after i.v. administration (Figure 1A). At a dose of 50 mg/kg, the Cmax was 19.5 U/ml after i.p. administration and 107.5 U/ml after i.v. administration (Figure 1B). Furthermore, at a dose of 5 mg/kg, the Tmax was 3 h after i.p. administration and 1 h after i.v. administration. At a dose of 50 mg/kg, the Tmax was 6 h after i.p. administration and 1 h after i.v. administration (Figure 1A). Thus, i.p. administration resulted in a longer, dose-dependent Tmax, whereas i.v. administration resulted in a higher, dose-dependent Cmax.
In the peritoneal dissemination model, BK-UM was efficacious, independently of the route of BK-UM administration. To assess efficacy based on the route of BK-UM administration in the peritoneal dissemination model, mice were first subjected to an i.p. administration of ES-2-Luc cells, 50 mg/kg BK-UM was then delivered via either the i.p. or i.v. route for 5 consecutive days and the results were compared with the controls. To assess the tumour-inhibiting effects of BK-UM, the IVIS imaging system was used to quantify disseminated lesions from ROI. Furthermore, survival rates were calculated.
A comparison of ROI values did not reveal significant differences in tumour-inhibitory effects in either group regardless of the BK-UM delivery route. However, in both BK-UM-treated groups, tumour growth was significantly inhibited compared with controls (Figure 2). In addition, no significant differences in survival rates were observed between the i.p. and i.v. groups. However, both routes of administration significantly prolonged survival time compared to controls (Figure 2C).
In the subcutaneous tumour model, i.v. administration of BK-UM inhibited tumour growth more than i.p. administration. To assess efficacy based on the route of BK-UM administration in the subcutaneous tumour model, ES-2 cells were subcutaneously transplanted into mice and BK-UM was administered via either the i.p. or i.v. route at a dose of 50 mg/kg once a day for 5 days or once a week for 4 weeks. In the daily-treated group, both i.p. and i.v. administration significantly inhibited the tumour growth compared to controls. However, no significant differences in tumour growth were observed between i.p. and i.v. administration (Figure 3A). In the weekly-treated group, i.v. administration significantly inhibited tumour growth compared to i.p. administration and controls (Figure 3A). Despite slight differences in the treatment schedule, i.v. administration had a higher tumour-inhibitory efficacy. Neither abnormal behaviour nor abnormal weight loss were observed after i.p. or i.v. administration of BK-UM in either the daily or weekly group (Figure 3B).
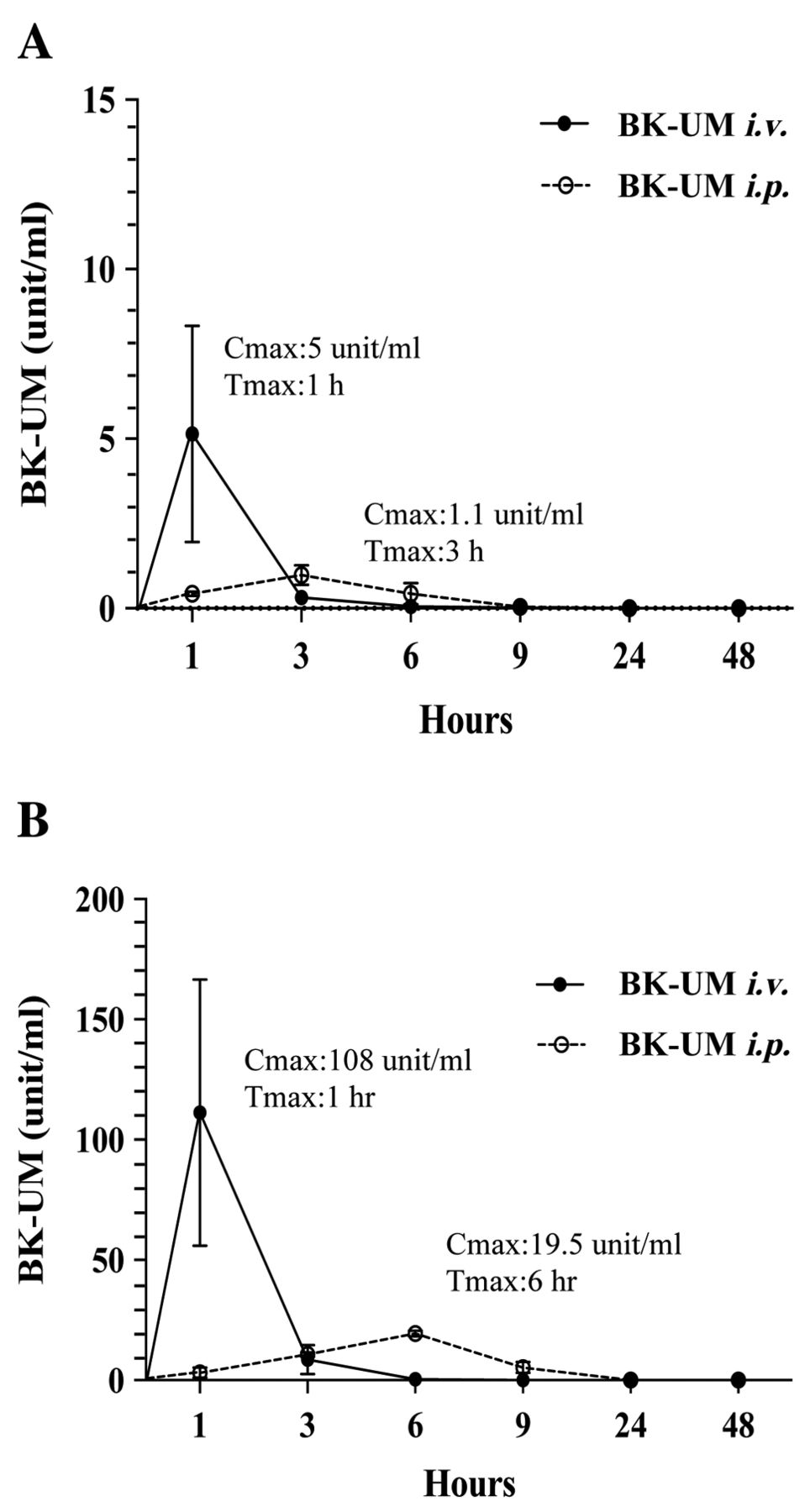
Pharmacokinetic assessment of BK-UM. Comparison between i.v. and i.p. administration of 5 mg/kg (A) and 50 mg/kg (B) BK-UM to rats (n=7 per group). Data represent the mean±standard error.
Discussion
In the present study, both i.v. and i.p. delivery of BK-UM induced significant antitumour effects in mice harbouring either ES-2-Luc cell tumours disseminated into the peritoneal cavity or ES-2 cell xenografts. In addition, both i.v. and i.p. administrations of BK-UM were found to be safe without apparent side-effects, such as weight loss.
As higher Cmax values resulted from the i.v. administration compared to those from the i.p. administration of BK-UM, efficacy is expected to be demonstrated at lower drug doses with the i.v. route. However, if blood concentrations become too high due to factors such as repeated administration, side-effects are expected. Administration i.p. resulted in lower Cmax and longer Tmax values than i.v. administration, i.p. administration would be expected to be superior to i.v. administration with regard to side-effects as a variety of drug concentrations and treatment schedules can be utilized.
Regarding the observed antitumour effects, different results were obtained in the peritoneal dissemination and subcutaneous tumour models. Administration i.p. was more efficacious than i.v. in the peritoneal dissemination model because the administered BK-UM came directly into contact with the tumour and inhibited the proliferation of disseminated lesions, possibly inhibiting the production of ascites. On the other hand, i.v. administration was superior in the subcutaneous tumour model on a weekly treatment schedule as a systemic administration method. Although i.p. administrations were efficacious on a weekly schedule, higher concentrations and longer times may be required to reach subcutaneously transplanted tumour cells through the circulatory system. i.p. administration of BK-UM may be suitable for the ascites and tumour dissemination characteristics of ovarian cancer patients, whereas i.v. administration may be suitable for cancer patients with distant metastases.
Although we have already reported the safety of i.p. administration of BK-UM in a study of side-effects, the safety of i.v. administration is yet to be assessed (13). In this study, regardless of the drug delivery route or treatment schedule, no apparent side-effects of sudden death, abnormal behaviour or weight loss were observed and both routes of administration were safely utilized.
Conclusion
Administration of BK-UM by i.v. route is both efficacious and safe for the treatment of ovarian cancer.
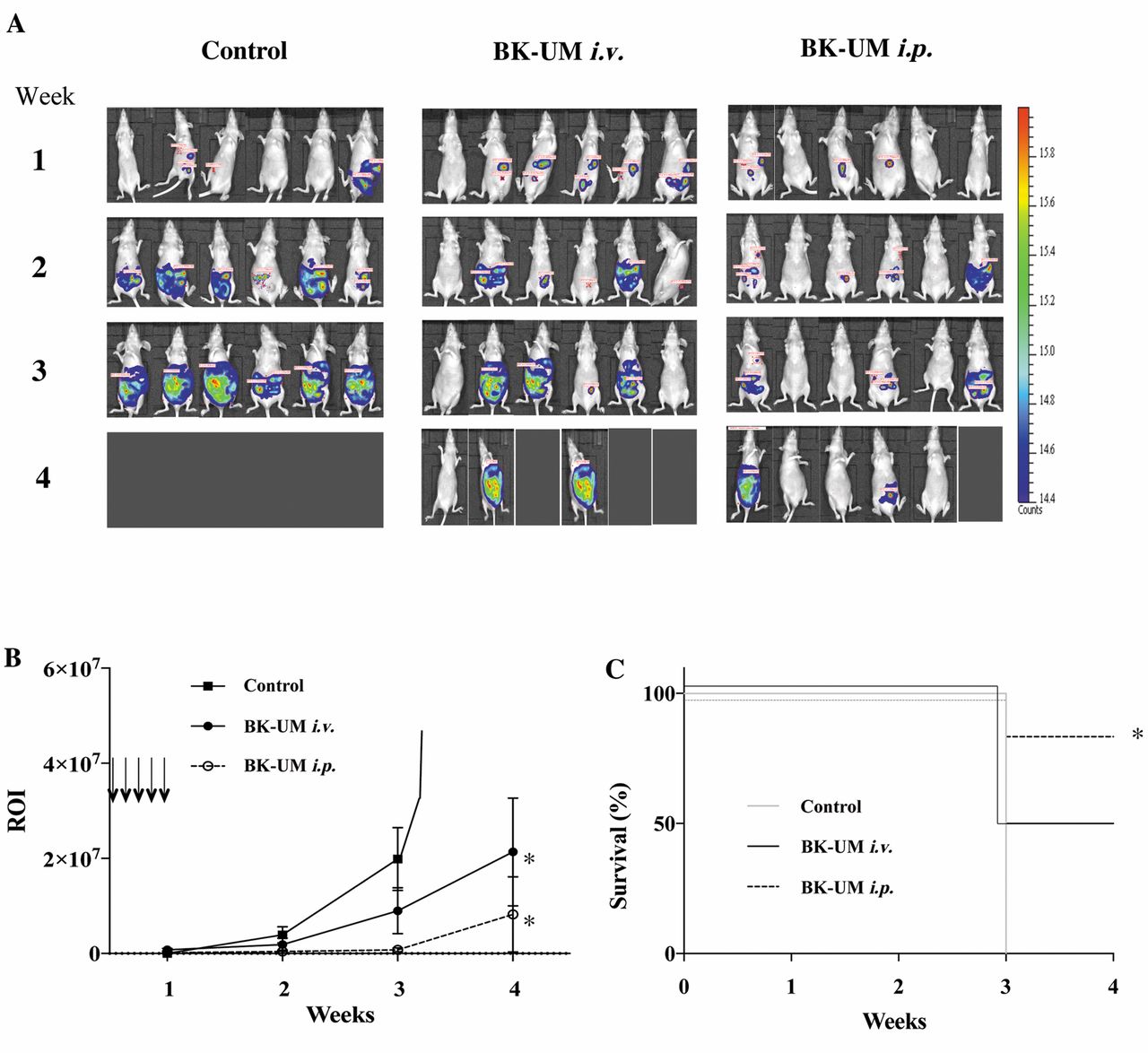
Antitumour effects of BK-UM in the peritoneal dissemination model (n=6 per group). A: Images of tumour-bearing mice as captured using the IVIS imaging system from 1 to 4 weeks, and the regions of interest (ROI) are shown in colour. Red indicates high, whereas blue indicates low. B: Graph comparing values for ROIs. Arrowheads indicate the time points of BK-UM administration. Data represent the mean±standard error. C: Survival curves for the different groups of mice. *Significantly different compared to controls at p<0.05.

A: Comparison of antitumour effects of BK-UM (A) and bodyweight of mice (B) in the subcutaneous tumour model following a daily treatment schedule (upper panel), and weekly treatment schedule (lower panel). Arrowheads represent the time points of BK-UM administration. Data represent the mean±standard error. *Significantly different compared with controls at p<0.05.
Acknowledgements
This work was supported in part by a Grant-in-Aid for Young Scientists (B) (no. 227790536) Challenging Exploratory Research (no. 26670731), Scientific Research (B) (no. 26293362), Scientific Research (C) (no. 23592470) and funds from the Central Research Institute of Fukuoka University (141011), The Center for Advanced Molecular Medicine, Fukuoka University from the Ministry of Education, Culture, Sports, Science and Technology (Tokyo, Japan), a Grant-in-Aid from the Kakihara Science and Technology Foundation (Fukuoka, Japan) and Princess Takamatsu Cancer Research Fund to S. Miyamoto.
Footnotes
↵* These Authors contributed equally to this study.
Conflicts of Interest
The Authors declare that they have no conflicts of interest in regard to this study.
- Received May 9, 2017.
- Revision received May 29, 2017.
- Accepted June 6, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}