


Abstract
Background: In the seventh edition of the Union for International Cancer Control (UICC) TNM classification, supraclavicular lymph node (SCLN) in regard to thoracic esophageal cancer (EC) is regarded as a distant organ, therefore, if resectable, SCLN metastasis is considered a candidate for systemic chemotherapy. The purpose of this study was to clarify the survival outcome in patients with resectable thoracic EC with SCLN metastases (M1LYM) treated with curative intent. Patients and Methods: Clinical outcomes in patients with resectable thoracic EC with SCLN metastases (M1LYM) treated by esophagectomy or definitive chemoradiotherapy (dCRT) were retrospectively analyzed. Results: A total of 102 patients were divided in three groups: Surgery with perioperative therapy, n=45; surgery alone, n=19; and dCRT, n=38. Overall, median progression-free survival and median survival time were 9.3 and 26.7 months, respectively. The median survival time was 27.5 months in the group treated with surgery with perioperative treatment, 50.6 months in those treated with surgery alone, and 22 months in the dCRT group. No significant survival difference was seen among the three groups. Conclusion: Over 30% of patients with resectable M1LYM treated with curative intent achieved long-term survival.
Although perioperative chemotherapy or chemoradiotherapy before or after surgery is a standard treatment for advanced resectable esophageal cancer (EC), definitive chemoradiotherapy (dCRT) is performed alternatively as an optional treatment (1). Clinical outcomes of local treatment such as surgery for EC generally depend on the clinical stage. Surgical outcomes with or without perioperative chemotherapy or chemoradiotherapy for patients with supraclavicular lymph node (SCLN) metastases were thought to be dismal in Western countries (2). Thus, in the seventh edition of the UICC TNM classification, SCLN metastases of thoracic EC are regarded as distant metastases (3). Therefore, according to the National Comprehensive Cancer Network guidelines (4), thoracic EC with SCLN metastases (M1LYM) is considered a candidate for systemic chemotherapy in Western countries.
In contrast, the Japanese multi-institutional nationwide registry of EC showed that 14.5% of patients who underwent esophagectomy had SCLN metastases histologically, which means some SCLN metastases can be recognized as being resectable, similarly to other regional nodes (5). Moreover, previous reports indicated that some patients with SCLN metastases who underwent esophagectomy achieved long-term survival, and SCLN metastases had little prognostic impact for EC (5, 6). Thus, in the 10th edition of the Japanese classification of EC (7), as SCLNs are regarded as regional lymph nodes in thoracic EC, M1LYM is usually treated with curative intent in Japan.
While the therapeutic value of adding local treatment (surgery or radiotherapy) in M1LYM judged by pre-treatment imaging to be resectable remains controversial, prognosis should be anticipated for determining the treatment strategy, whether local or systemic therapy. The purpose of this study was to clarify the survival outcome of patients with clinically judged resectable M1LYM treated with curative intent (esophagectomy with/without perioperative treatment, or dCRT).
Patient characteristics.
Patients and Methods
Patient selection. We retrospectively analyzed patients with resectable M1LYM, detectable by imaging before treatment, who were initially treated by esophagectomy with/without perioperative treatment, or with dCRT at the National Cancer Center Hospital (NCCH). Clinical data for this study were extracted from our database of consecutive patients. Clinical staging was determined at a multidisciplinary team conference based on the findings of upper gastrointestinal endoscopy (UGI), endoscopic ultrasonography, and cervico-thoracic-abdominal thin-slice computed tomography. Neck ultrasonography and 18F-fluorodeoxyglucose positron-emission tomography were performed if necessary. Patients with cervical or abdominal EC, histology other than squamous cell carcinoma (SCC), unresectable (T4) disease, simultaneous advanced malignancies, or without detailed follow-up data were excluded. Surgical resectability was reviewed by two EC surgeons. This retrospective study was approved by the Institutional Review Boards of NCCH (2012-268).
Data collection and statistical analyses. Performance status (PS) was evaluated according to the Eastern Cooperative Oncology Group criteria (24). Clinical staging was classified according to the seventh edition of the UICC-TNM classification (3). A clinical complete response (cCR) after dCRT was defined according to the Response Evaluation Criteria in Solid Tumours (RECIST) guideline version 1.1 (25), when (i) no residual tumor was detected by UGI and CT, and (ii) no malignant cells were detected in biopsy specimens taken by UGI.
Overall survival (OS) was defined as the time from the date of initiating the first treatment to death (all causes) or was censored at the last date of confirmed survival. Progression-free survival (PFS) was defined as the time from the date of initiating the first treatment to the date of the first progression or death (all causes), whichever came first, or was censored at the last date of confirmed no progression. For patients who underwent salvage esophagectomy for non-progressive remnant disease after dCRT, incomplete (R1/2) surgery or disease recurrence after curative (R0) surgery were defined as PFS events. Locoregional relapse was defined as recurrence inside of the surgical field for patients who underwent esophagectomy, and recurrence inside of the radiation field for patients who received dCRT.
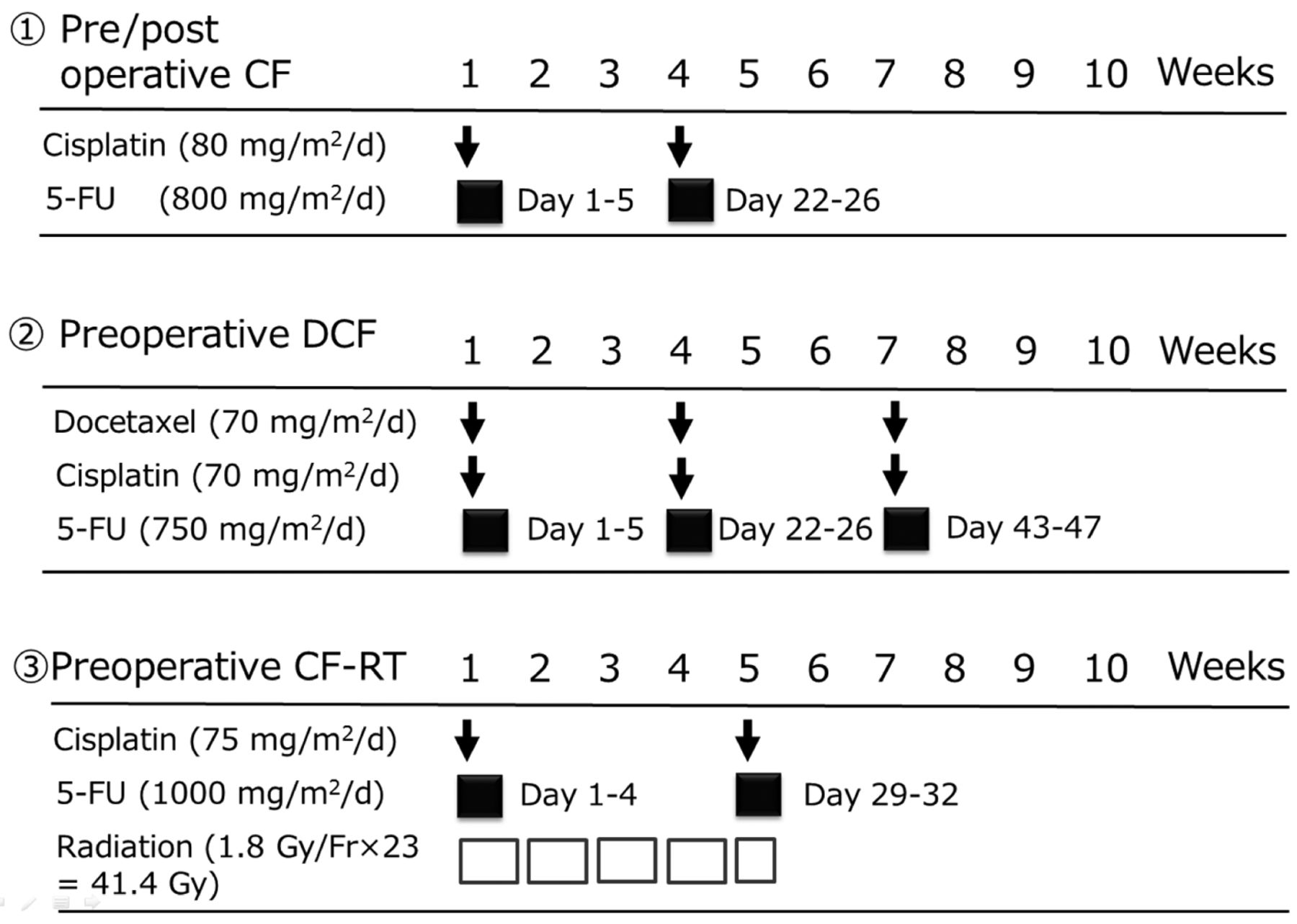
Regimens for perioperative treatment. 5-FU: 5-Fluorouracil.
Survival curves were drawn with the Kaplan–Meier method and compared by the log-rank test. Patient characteristics were compared with the Wilcoxon rank-sum test or Fisher's exact test, as appropriate. Univariate and multivariate analyses were performed with Cox regression models. From the clinical point-of-view, eight variables were included in the models: age, PS, tumor location, clinical T-stage, clinical N-stage, clinical presence of intramural metastases (cIM), leukocyte (WBC) count (>8,000/mm3), and albumin (≥4 g/dl). The proportional hazards assumption was confirmed by a score test (8). A two-sided p-value of less than 0.05 was deemed statistically significant. All statistical analyses were performed using SAS software (version 9.4; SAS Institute, Inc., Cary, NC, USA).
Results
Patient characteristics. Of 8467 patients with primary EC treated at NCCH from January 2001 to December 2012, data for 251 patients with SCLN metastases detectable by imaging without distant metastases were extracted. Of these patients, 149 were excluded because of cervical or abdominal EC in 48, histology other than SCC in 12, T4 disease in 79, simultaneous advanced malignancy in four, and due to lack of detailed follow-up data in six. Finally, a total of 102 patients were the subjects of our study. Patients were divided into three groups according to treatment modality: Surgery with perioperative therapy (S/Tx), surgery alone, and dCRT. There was no difference in the patient characteristics among the three groups (Table I).
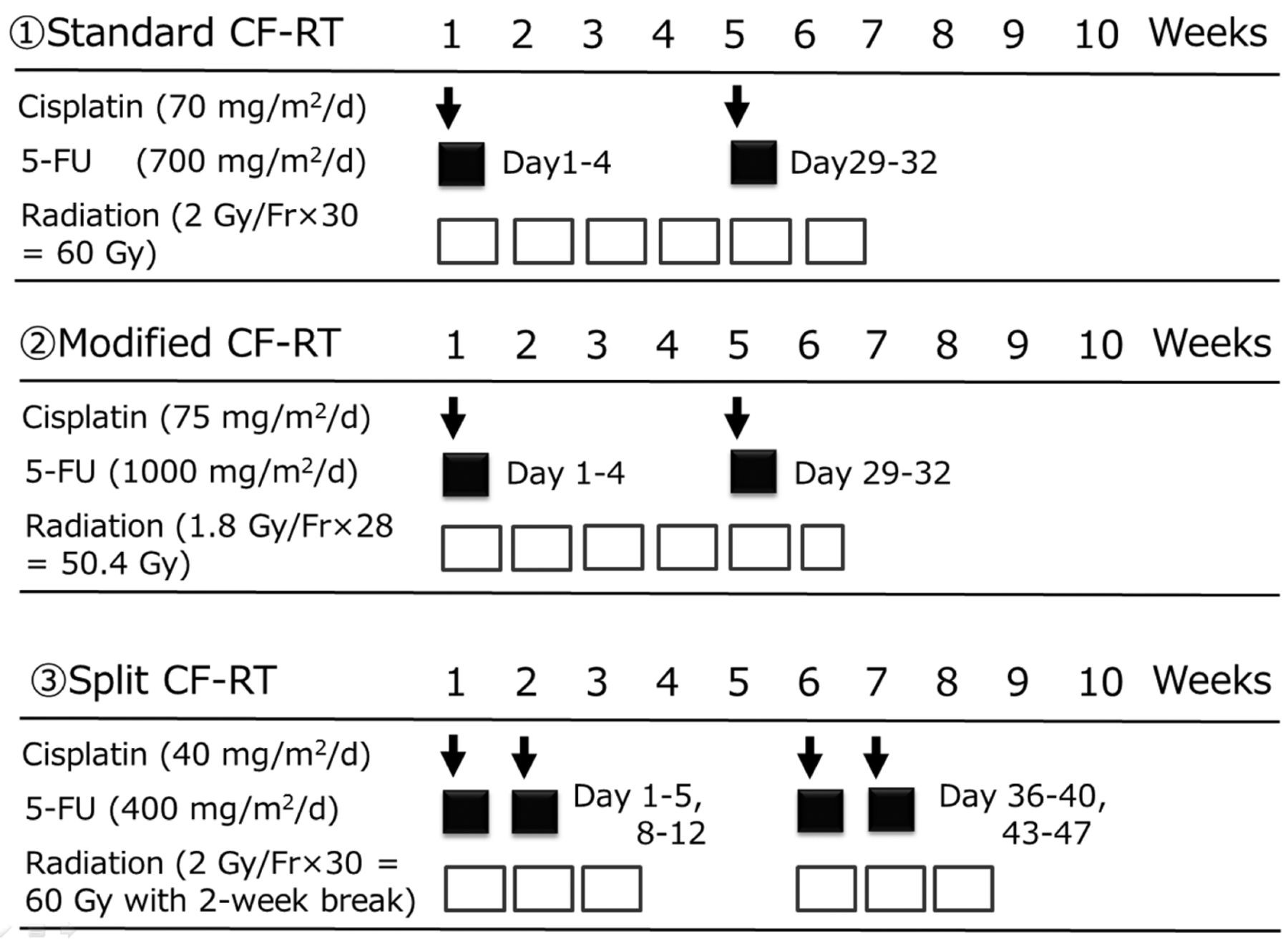
Sixty-four (62.7%) of the 102 patients underwent surgical treatment. Thirty-five (54.7%) out of these 64 patients comprised the S/Tx group (Figure 1): preoperative cisplatin plus 5-fluorouracil (CF) in 25 patients, preoperative docetaxel, cisplatin plus 5-fluorouracil (DCF) in six, preoperative CF-radiotherapy in two, and other regimens in two patients. Ten patients (15.6%) received postoperative CF. Nineteen patients (29.7%) underwent surgery without perioperative treatment. In four out of the 45 patients in the S/Tx group, and in one of 19 patients in the surgery-alone group, esophagectomy was performed with macroscopic residual tumor (R2). Another 59 patients who underwent curative esophagectomy underwent bilateral cervical neck lymphadenectomy. Hence, 38 out of the 102 patients received dCRT (Figure 2): standard CF-radiotherapy in 27 patients modified CF-radiotherapy in five, split CF-radiotherapy in two, and other regimens in four patients. Twenty (52.6%) of these patients achieved cCR.
Twenty-eight patients without preoperative treatment (10 in the S/Tx group and 18 in the group treated with surgery alone) underwent bilateral neck lymph node dissection. Pathological SCLN metastases were observed in 25 out of 28 patients, the positive predictive value of clinical diagnosis for SCLN metastases was 89.3%.

Regimens for definitive chemoradiotherapy. 5-FU: 5-Fluorouracil.
Analyses of survival data and prognostic factors. For the whole patient cohort, the median follow-up of survivors was 39.8 (range=9.4-136.7) months. The median PFS for the whole cohort was 9.3 months (1/3/5-year PFS: 43.6/33.6/25.6%), for the S/Tx group 9.1 months (1/3/5-year PFS; 43.3/32.1/25.7%), for the group treated with surgery alone 25.1 months (1/3/5-year PFS: 63.2/47.4/41.4%), and for the dCRT group 8.5 months (1/3/5-year PFS: 34.2/28.4/17.8%) (Figure 3). The median OS was 26.7 months (1/3/5-year OS: 81.1/44.8/34.8%) for the whole cohort, 27.5 months (1/3/5-year OS: 88.8/49.2/43%) in the S/Tx group, 50.6 months (1/3/5-year OS: 78.9/52.6/46.8%) in the surgery-alone group, and 22 months in the dCRT group (1/3/5-year OS: 73.2/35.1/20.5%) (Figure 4). The surgery-alone group survived longer than the S/Tx and dCRT groups, although no significant survival difference was observed among the three groups by log-rank test (Figure 3: p=0.2823; Figure 4: p=0.1383). Moreover, in the subsets classified by tumor location, no significant survival difference was observed.
A multivariate analysis indicated that the depth of the primary lesion (clinical T3), advanced age (≥65 years old), and high WBC count (>8,000/mm3) were independently associated with poor OS (Table II), whereas depth of primary lesion was independently associated with poor PFS (Table III) in patients with resectable M1LYM who were treated with curative intent.
Two patients who underwent esophagectomy (3.1%; 2/64) died within 30 days after surgery due to surgical complications (sepsis and suffocation by tracheal stenosis). On the other hand, no treatment-related death and severe late toxicities were observed in the dCRT groups.
Recurrence pattern and treatment after initial treatment relapse. In the S/Tx group, 24 out of 41 patients (53.7%) experienced recurrence after curative surgery. Among these, locoregional relapse after R0 resection was observed in eight patients (33.3%), distant relapse in six (25%), and both local and distant relapse in nine (37.5%) (recurrence site of one patient was unknown). In the group treated with surgery alone, nine out of 18 patients (50%) experienced recurrence: local in six (67%) patients, distant in two (22%), and both local and distant in one (11%). In the dCRT group, 20 patients achieved cCR, and nine patients (45%) experienced recurrence: local in four (44%), distant in three (33%), and both local and distant in one (11%) (recurrence site of one patient was unknown).
Twenty-two out of 28 patients who experienced relapse after the initial treatment (recurrence: 24, non-curative resection: four) in the S/Tx group and five out of 10 patients who experienced relapse after the initial treatment (recurrence: nine, non-curative resection: one) in the surgery-alone group received antitumor treatment. Eleven of them received CRT and one of them was alive without additional treatment. In the dCRT group, 12 out of 27 patients who experienced relapse after the initial treatment (recurrence after cCR: nine, non-CR: 18) received antitumor treatment. Four of them underwent salvage esophagectomy, two for locoregional relapse and two for remnant tumor, and one remained alive without a second relapse.

Progression-free survival of patients according to therapy. dCRT: definitive chemoradiotherapy; S alone: surgery alone; S/Tx: surgery plus perioperative therapy.
Discussion
In Japan, radical esophagectomy with extended lymphadenectomy has been performed for thoracic EC (9). From this precedent, detailed distribution of lymph node metastasis has been obtained, and 15-20% of surgical cases with thoracic EC with SCC histology have SCLN metastases (5, 6, 10). One report showed patients with pathologically confirmed M1LYM did not have a worse prognosis than those with TNM-N3 who underwent esophagectomy with extended lymphadenectomy (5-year OS; M1LYM: 26.5 months, TNM-N3: 17.6 months) (6). Another study reported that the survival of patients with pathologically confirmed M1LYM who underwent esophagectomy was not too bleak (5-year OS: 24.1%) and SCLN metastases was not a prognostic factor in multivariate analysis. Additionally, they noted SCLN had characteristics similar to other regional lymph nodes in terms of prognosis (5). In our study, over 30% of patients with resectable M1LYM treated with curative intent achieved long-term survival. Our 5-year survival rates seem to be better than those of the previous reports (2, 11). Locoregional treatment with curative intent was applied even for local failure after initial treatment. Previous reports showed that 10-20% of patients with local failure after initial surgery achieved cCR or long-term survival after dCRT (12, 13). It is speculated that the sequence of locoregional treatments for local failure, salvage esophagectomy or chemoradiotherapy, might contribute to favorable clinical outcomes. Compared with survival data of historical cohorts (14-17), our study shows that the clinical outcomes of patients with resectable M1LYM treated with curative intent are closer to those of localized disease rather than those of systemic disease (Table IV).
In our study, more cases achieving long-term survival were observed in the surgically-treated groups (5-year OS: 43% in the S/Tx group and 46.8% in the group treated with surgery alone) than in the dCRT group (5-year OS: 20.5%). There was no significant survival difference according to treatment by univariate analysis. It is inappropriate to compare survival by treatment modalities because selection bias might exist. Nineteen patients were treated with surgery alone, not a standard treatment for advanced thoracic EC. Seventeen of these patients underwent surgery before March 2008, confirming the result of a randomized controlled trial for the efficacy of neoadjuvant strategy (JCOG9907) in Japan (15). These 17 patients did not receive adjuvant CTx for the following reasons: poor PS after surgery in six, two or less pathologically positive lymph nodes in 10, and patient refusal in one case. Another two patients did not receive neoadjuvant CTx because of renal impairment and patient refusal.

Overall survival of patients according to therapy. dCRT: definitive chemoradiotherapy; S alone: surgery alone; S/Tx: surgery plus perioperative therapy.
In our study, multivariate analysis demonstrated that a clinical depth of T3 was an independent negative prognostic factor, consistent with reports from both Japan and Western countries (18, 19). Recently, Yokota et al. showed that a preoperative clinical depth of T3 and low serum albumin (<4.0 g/dl) are independent prognostic factors for patients undergoing preoperative chemotherapy for advanced thoracic esophageal SCC, based on data from JCOG9907 (20). Our study also revealed that a clinical depth of T3 was one of the most powerful prognostic factors in patients with resectable M1LYM, but no prognostic value of serum albumin was shown. On the other hand, a high WBC count (>8,000/mm3) was a poor prognostic factor in our study. A previous report proposed C-reactive protein (CRP) as a useful prognostic factor of inflammation in EC (21). Similarly to CRP, a high WBC count is considered to reflect systemic inflammation. In our study, patients with a high CRP level tended to have poor survival. However, since CRP was not assessed in approximately one-third of the patients in the pretreatment examination, CRP was excluded from our analysis.
Potential weaknesses of our study are its retrospective nature, the limited sample size, and the lack of histological diagnosis for SCLN metastases. Although further validation of our data is required in a prospective cohort, it is difficult to conduct a randomized controlled trial because of the limited number of patients with resectable M1LYM. Moreover, SCLN metastases were determined only by imaging examination. Confirmatory diagnosis of lymph node metastasis should be performed through a histological approach (e.g. fine-needle aspiration). However, the positive predictive value of clinical diagnosis for SCLN metastases was high (89.3%) in patients who underwent surgery without preoperative treatment. In addition, clinical staging was determined at a multidisciplinary team conference, and the judgement of clinical SCLN metastases in all groups was made using the same criteria, thus the rate of true SCLN metastases among the three groups can be considered similar.
Univariate and multivariate analyses of overall survival with Cox proportional hazards models.
In our study, almost all cases received neoadjuvant CF as a preoperative treatment. Although in Western countries, preoperative CRT is a standard treatment for resectable locally advanced EC (22, 23), the efficacy of preoperative CRT for resectable M1LYM is still unclear. Further investigation of appropriate preoperative approaches for resectable M1LYM is also warranted.
In conclusion, our study indicates that over 30% of patients with resectable M1LYM treated with curative intent achieved long-term survival.
Univariate and multivariate analyses of progression-free survival with Cox proportional hazards models.
Comparison of survival data in this study with those in historical cohorts.
Acknowledgements
The Authors thank Ms. Emiko Usami for data collection. There was no grant support for this study.
Footnotes
Conflicts of Interest
The Authors have no conflict of interest in regard to this study.
- Received March 13, 2017.
- Revision received April 5, 2017.
- Accepted May 5, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.