


Abstract
Background: Cancer antigen CA72-4 is a tumor marker found to be elevated in a variety of human adenocarcinomas. Using the DRG TM-CA72-4, we quantified the elevation of CA72-4 compared to current United States Food And Drug Administration-approved tumor markers in various cancer types. Materials and Methods: We conducted a prospective, single-center study enrolling 96 patients between March 2013 and August 2016 with different locally advanced, unresectable or metastatic cancer known to express CA72-4. Quantification of CA72-4 was performed according to the manufacturer's instructions using the DRG TM-CA72-4 enzyme-linked immunosorbent assay kit and the positivity rates were calculated. Results: CA72-4 expression varied with tumoral site of origin, with the highest positivity rates found in pancreatic and ovarian malignancies. Correlation with clinical activity was also noted in some patients. Conclusion: CA72-4 may have a potential role as an adjunct to conventional biomarkers in disease monitoring of pancreatic, ovarian and colorectal carcinomas.
In the management of metastatic and recurrent cancer, it is vital to assess response to antitumor therapy. The most commonly used methodology is by serial measurement of tumor size on physical examination or imaging studies employing the response evaluation criteria in solid tumors (RECIST) criteria. As an adjunct to direct measurement of lesions, several tumor markers including carcinoembryonic antigen (CEA), cancer antigen 19-9 (CA19-9) and cancer antigen 125 (CA125) have obtained United States Food and Drug Administration (FDA) approval for the monitoring of various gastrointestinal and gynecologic malignancies. These tumor markers along with cancer antigen 27-29 (CA27-29) used in the monitoring of breast cancer are proteins shed by cancer cells and are readily measured in the laboratory using antibodies.
The utility of serial measurement of CA19-9, CEA, and CA125 in predicting treatment response in pancreatic, colon and ovarian cancer has been validated in multiple studies (1-4). Frequent serial measurements can easily be obtained and have the potential of alerting the clinician to the need for timely assessment of a patient for treatment failure, allowing for earlier intervention. In addition, tumor markers may at times have greater accuracy in assessing response since imaging studies using RECIST criteria are not totally reliable as they do not always differentiate viable tumor from residual fibrosis or scarring. Nevertheless, their usefulness in tumor monitoring has been limited by their inconsistent and variable elevation in various malignancies, the need for a relatively large tumor burden to cause an elevation, frequent false-positive elevations in non-malignant conditions, and by lack of conviction by the oncological community to accept an increase or decrease in the tumor marker as a surrogate for disease progression or response. Thus, there remains and unmet need for development of new biomarkers for assessment of tumor burden and response to therapy. While rapidly-evolving research utilizing analysis of circulating tumor DNA as well as proteomics is underway, we continue to rely on traditional techniques such as measuring of concentrations of abnormal proteins shed by various cancer types.
In addition to the conventional tumor markers CEA, CA27-29, CA19-9 and CA125 there is another tumor marker, tumor-associated glycoprotein 72 (TAG-72) developed years ago used world-wide which never gained US FDA approval. This is a 48-kDa mucin-like glycoprotein complex, identified with the monoclonal antibody B72.3, a murine antibody raised against a membrane-enriched fraction from a human breast carcinoma liver metastasis (5). CA72-4 antigen is an antigenic determinant of the TAG-72 glycoprotein, which is also recognized by the B72.3 and CC-49 monoclonal antibodies (6). This antigen has been found in a variety of human adenocarcinomas including colorectal, gastric, ovarian, breast, and lung, however, it is rarely expressed in benign and normal adult tissues (7-9).
While CA125, CEA and CA19-9 currently are standard tumor markers for ovarian, gastrointestinal (i.e. stomach, colon and small bowel) and pancreatic cancer, respectively, CA72-4 remains a potentially superior biomarker for these types of cancer.
The DRG TM CA72.4 enzyme-linked immunosorbent (ELISA) kit is a solid-phase sandwich assay, utilizing CC-49 antibody, developed by DRG International (New Jersey, USA) and validated as a standalone assay to be employed in the individual hospital and laboratory setting. Using the DRG TM CA72-4 ELISA assay, the current study aimed to i) quantify the rate of elevation of the tumor marker CA72-4 in each cancer type compared to the rate of elevation of other current FDA-approved tumor biomarkers, and ii) correlate levels of CA72-4 to clinical outcomes in patients with measurable disease.
Materials and Methods
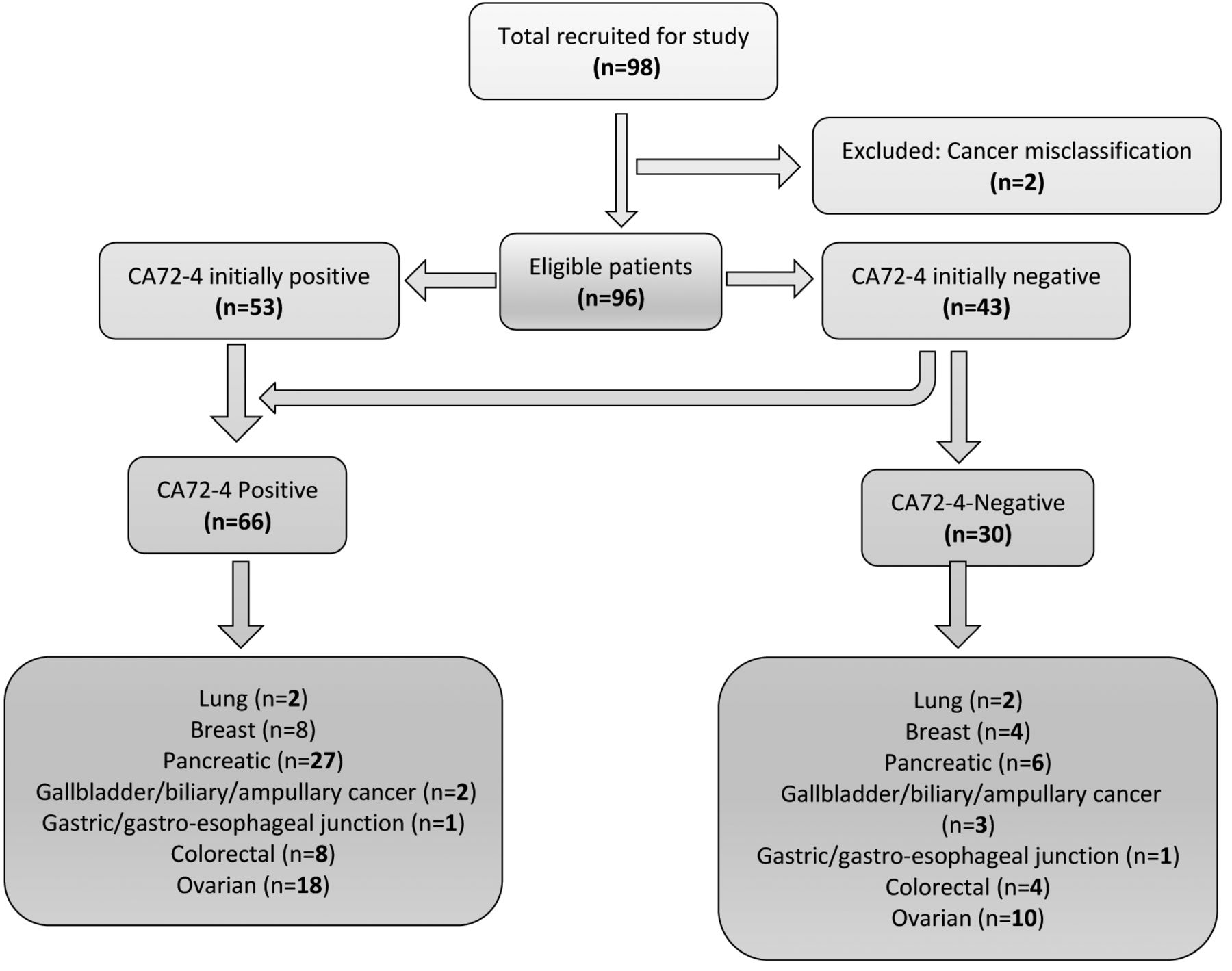
Study participants. We conducted a prospective, single-center study involving 96 patients with different histologically confirmed, primary locally advanced or metastatic cancer with measurable disease that were known to express CA72-4 (Figure 1). Patients were enrolled between March 2013 and August 2016. Informed written consent was obtained from all individuals prior to enrollment in the study and the study was approved by the Institutional Review Board (#12040).
Blood serum was collected from patients undergoing treatment at 3- to 4-week intervals for CA72-4 measurement along with other FDA-approved markers for site-specific malignancies. Patients with the following characteristics were included in the study: 18 years of age or older, de novo or previously diagnosed metastatic or recurrent non-surgically resectable carcinomas of the ovaries, non-squamous lung carcinoma, adenocarcinoma of the pancreas, stomach, breast, gallbladder, biliary, ampullary, colorectal, gastric, gastro esophageal junction or esophagus (Table I). Only patients with a detectable level of CA72-4 at enrollment or who developed a detectable level during the first four consecutive blood draws were followed in the study. Patients with more than four consecutive negative CA72-4 determinations were excluded from subsequent CA72-4 blood draws, and classified in the CA72-4-negative group but were followed clinically and with established tumor markers as correlates based on clinical indication (e.g. CA19-9 for pancreas, CA27-29 for breast and CEA for gastric cancer).
Demographics and enrollment data.
Quantification of CA72-4 in blood serum. Briefly, whole blood was collected via venipuncture and allowed to clot. Serum was separated by centrifugation at room temperature within 1 h collection or sooner and samples frozen at −20°C for further processing. Quantification of CA72-4 was performed using the DRG TM-CA 72-4 ELISA kit according to the manufacturer's instructions. A five-point calibration curve was generated for each ELISA plate, with both a low and high control included in each run to ensure reliability of the assay results. The limit of detection of the assay was 0.8 U/ml. Calibrators, controls, and each patient sample were tested in duplicate on the ELISA plate in order to calculate the within-run mean, standard deviation, and coefficient of variance for each of the patient samples. Twenty microliters of appropriate sample (calibrator, control, or patient) was added to each well on the antigen-coated plate, placing sample duplicates horizontally next to their matched pair. After all samples to be tested were transferred to the plate, 100 μl of enzyme conjugate was added to each well using a multi-channel pipette. Sample and conjugate were mixed within each well for a minimum of 10 sec, followed immediately by 2-h incubation at room temperature. At the completion of the first incubation period, the plate was washed five times with 400 μl of diluted wash solution per well. After washing of the plate, 100 μl of substrate was added to each well and plates were incubated further for 30 min at room temperature to allow for color development within the wells. At the end of the second incubation period, 100 μl of stop solution was added to each well and the absorbance was read on a spectrophotometer at 450 nm. Results were calculated using a 4-parameter Marquardt curve fit based on the mean absorbance reading per sample pair. Positivity was defined as a value greater than 0.8 U/ml or 4.0 U/ml based on systematic review of prior studies (10-12). Established levels of tumor markers CEA, CA19-9, CA27-29 and CA125 were determined according to existing commercial laboratory methods.
Results
A total of 96 patients were enrolled in the study over a 4-year period. The median age of patients with positive and negative CA72-4 assays were 65.5 versus 65.0 years, respectively (p=0.34). Of all CA72-4-positive patients, 33% were male, and of the negative patients, 40% were male (p=0.53).

Study design.
Using 0.8 U/ml as a cut-off for positivity for CA72-4 in our assay, we found that 55.2% (53/96) of the patients were positive and 44.8% (43/96) were negative for this tumor marker at the time of enrollment. Using the previously reported level of 4 U/ml as the cut-off for positivity reduced the positivity rate to 33.3% (32/96) and increased negativity to 66.7% (64/96) at enrollment. Using 0.8 U/ml as a cut-off, 30.2% (13/43) of the CA72-4-negative patients developed detectable levels of CA72-4 in their serum during the initial four blood draws versus 16/64 (25.0%) using 4 U/ml as a cut-off.
Site-specific data for each cut-off are presented in Table II. Using 0.8 U/ml as a cut-off, the highest rate of positivity for CA72-4 was found in pancreatic cancer (82%, 27/33), while currently established FDA markers such as CA19-9 were positive in 84.8% (28/33) of patients while using 4U/ml, this rate dropped to 58% (19/33). Lowest rates of positivity did not differ when using 0.8 U/ml or 4 U/ml as cut-off: 1/2 patients with gastric/gastroesophageal junction tumors, 2/5 with gallbladder/biliary tract tumors, while CA72-4 positivity in lung cancer decreased from 2/4 for 0.8 U/ml to 0/4 for 4 U/ml, although very few patents were enrolled with these types of cancer. Other sites of high positivity included ovarian at 64.3% (18/28) for 0.8 U/ml versus 57% (16/28) for 4 U/ml cut-offs, however, this included both mucinous and non-mucinous subtypes. Total positivity for CA72-4 amongst all patients across all categories was 68% (66/96) at 0.8 U/ml and 50% (48/96) for 4 U/ml.
Discussion
Tumor biomarkers play a crucial role in monitoring of response to therapy and in post-treatment surveillance of various gastrointestinal and gynecological malignancies (13). While the clinical value of FDA-approved tumor markers such as CEA, CA19-9 and CA125 has been established, adequate data to support FDA approval of CA72-4 as a potential biomarker are lacking and its measurement is only considered experimental and investigational. Here, we briefly review the nature of currently validated tumor markers and discuss the potential role of CA72-4 within the armamentarium.
CEA. A 180-kDa oncofetal cell-surface-anchored glycoprotein, CEA was first isolated in 1965 by investigators at McGill University from human colon tissue extracts (14). The glycoprotein, with a half-life of approximately 7 days, was found to be expressed in gastrointestinal and mucosal tissue during fetal development but only minimally expressed in adult tissue (15, 16). Further studies showed that it was also overexpressed in adenocarcinomas of varying origin including gastric, hepatic, lung, pancreatic, ovarian and prostate (17-24). In colon cancer, the specificity and sensitivity of CEA has been shown to vary with advancing tumor stage, with specificity ranging between 37% and 86% in advanced disease, providing a useful means of monitoring disease (25-27). CEA may also be elevated in benign conditions such as inflammatory bowel disease, pancreatitis and in smokers, limiting its utility in early-stage cancer and in patients with such conditions (28-31).
Disease distribution data for CA72-4 using 0.8 and 4 U/ml as cut-offs for positivity.
CA125. Encoded by the MUC16 gene, CA125 is a member of the mucin family of glycoproteins and is normally expressed in developing fetal epithelial lining of the body cavities and the female reproductive tract. The protein was first discovered by Dr. Robert Bast and other investigators at Harvard Medical School in 1981 after murine monoclonal antibodies were found to have reactivity with human epithelial ovarian carcinoma but not with non-malignant human tissues (32). CA125 is also associated with malignancies of the endometrium, fallopian tube, breast, lung, esophageal, gastric, hepatic and pancreatic cancers (33-37). Elevations in CA125 have also been observed in non-malignant conditions such as during menses, late pregnancy, episodes of serosal irritation such as endometriosis, benign follicular ovarian cysts, and conditions associated with inflammation such as pelvic inflammatory disease, peritonitis, ascites, pericarditis and pleural effusions (38). CA125 expression has been found to be positive in up to 83% of patients with advanced epithelial ovarian cancer but only in 50% of patients with stage 1 disease, thus limiting its role in ovarian cancer screening in the general population.
CA19-9. CA19-9 has been validated as a serum tumor marker for patients with advanced pancreatic cancer. However, elevations have also been demonstrated in malignancies of the esophagus, stomach, gallbladder, biliary tract, and pancreas (39). Using 37 U/ml as cut-off for the upper limit of normal, sensitivity and specificity of 81% and 90% respectively have been reported in patients with pancreatic cancer with specificity increasing to almost 100% when a cut-off of 1,000 U/ml was used (3). Values over 1,000 U/ml also had implications in management and predicting response to therapy. For example, patients with a CA19-9 level greater than 1,000 U/ml at time of diagnosis were more likely to have unresectable disease (40). Biomarker analysis in large phase 3 pancreatic cancer trials showed that a decrease in CA19-9 by at least 90% correlated with increased survival (41-43). Prognostication studies by Reni et al. showed that the basal value of CA19-9 in advanced pancreatic disease correlated with survival (44, 45). Outcome analysis of CA19-9 nadir as a response to therapy affected overall survival, with patients showing survivals of 6.5, 10 and 16.7 months for an increase or decrease in CA19-9 of <50%, decrease by 50-89%, and greater than 89% decrease, respectively. Additionally, a more recent study has also suggested that a decrease in CA19-9 by 8 weeks may be more predictive of survival compared to radiological response, making reliable tumor marker measurement an important tool in the management of patients (41).
Despite the usefulness of CA19-9 in monitoring pancreatic and biliary cancer, its overexpression in benign inflammatory conditions such as choledocholithiasis, acute and chronic pancreatitis, diverticulitis, Hashimoto's thyroiditis, rheumatoid arthritis and non-inflammatory conditions such as obstructive jaundice, ovarian cysts and heart failure may result in high false-positive rates of 10-30%, limiting its usefulness in metastatic disease in patients with these conditions (46). Other limitations of CA19-9 include its dependence on fucosyltransferase for synthesis, an enzyme absent in up to 5% of the population, which is also required for human blood group Lewis antigen synthesis. As a result, measuring CA19-9 in patients with Lewis-null blood type may result in a potential false-negative result, further limiting its usefulness (47).
CA72-4. The tumor marker CA72-4 was first described by Dr. Jeffrey Schlom in the early 1980s as a novel antigen reactive to murine antibodies produced by mice that were immunized with membrane-enriched fractions of human metastatic mammary carcinoma cells (5). Of these, several monoclonal antibodies, including B72.3, were identified to have preferential binding to human carcinoma cells with sparing of normal adult tissues (5).
The advancement of monoclonal antibody testing in the late 1980s allowed continued development of novel identification techniques that facilitated further detection and characterization of CA72-4 (48). Initial studies showed elevation of CA72-4 in the sera of up to 40% of patients with colorectal and 42.6% of patients with gastric cancer, with increased levels being significant correlated with advanced stages of disease (12, 49). Additionally, it was found that approximately 50% of patients with colon cancer with undetectable CEA levels were in fact positive for CA72-4. Longitudinal studies of postoperative patients that did not have initial elevation of CEA in blood showed there to be an early rise in CA72-4 before clinical manifestation of recurrent disease (50). In 1994, study to further characterize the utility of CA72-4 by investigators at Massachusetts General Hospital showed that CA72-4 was differentially expressed in both benign and malignant pancreatic cystic lesions (51). Of 19 patients with uncharacterized pancreatic cysts, fluid aspirations revealed that intra-cystic CA72-4 levels were elevated in all five patients with cystadenocarcinomas, with a mean CA72-4 level of over 10,000 U/ml, compared to 3.8 U/ml in patients with pseudocysts, <3 U/ml in tuw serous cystadenomas and 44.2 U/ml in those with benign mucinous cystic neoplasms. CA72-4 in pancreatic cyst fluid was seen as a promising new marker for the differentiation of mucinous cystadenocarcinomas from pseudocysts, with intermediate CA72-4 levels suggesting the presence of benign mucinous cystic neoplasms (51). More recently, pre-operative evaluation of CA72-4 in patients with gastric cancer showed a correlation between serum CA72-4 levels and presence of lymph node metastasis, while elevations in peritoneal fluid corresponded with both T and N stage of disease (52), (53) suggesting a possible role in the staging of certain gastrointestinal malignancies.
Despite these early studies indicating a possible role of CA72-4 in the monitoring of advanced disease, testing for CA72-4 has not been widely adopted in the United States. Studies conducted on Japanese and East Asian patients with gastrointestinal malignancies combining CA72-4 with CEA and CA19-9 has shown useful disease correlation, with sensitivity of up to 74% without impairing specificity (54). Detectable levels of CA72-4 have also been found in patients with tumor of multiple origins including cancer of the lung (36%), ovary (24%, of which more than half had stage IV disease), and colon (40%) (50). Sensitivity of up to 40% in patients with colorectal and gastric carcinomas and 50% in ovarian cancer, with an overall specificity of over 95%, have been reported (55). Additionally, mathematical models combining pre-operative serum tumor biomarker measurements have shown a further increase in sensitivity and specificity in the detection of early-stage ovarian cancer, demonstrating clinical value in combinational analysis of multiple biomarkers in patients with ovarian cancer (56). Measurement of CA72-4 has also shown good correlation with disease burden and is predictive of disease recurrence (50).
In our study, we employed an ELISA-based method that can be used in an outpatient laboratory or hospital setting to reliably measure the CA72-4 level of patients with various malignancies. While several ELISA-based assays for detection of CA72-4 are already currently available and in active clinical use, it has only garnered approval in countries outside of North America. Our study supports the potential use and role of CA72-4 in disease monitoring and surveillance in various gastrointestinal and gynecologic malignancies, particularly of pancreatic and ovarian origin, in a North American population. We found that the rate of positivity of CA72-4 in pancreatic cancer at a level of detection cut-off of 0.8 U/ml, was comparable to the FDA-approved CA19-9 in our cohort, 82% versus 85% respectively, using the CC-49 antibody ELISA assay. Increasing the detection threshold to 4 U/ml as described in previously reported studies reduced the positivity rate to 58%. We also found that CA72-4 was elevated in approximately 64% of those with advanced ovarian malignancies, while corroborating existing positivity rates of approximately 80% for CA125 in the same population.
A specific example of concordance of the CA72-4 level with CA19-9 in clinical outcome and response to therapy is illustrated by a 60-year-old patient with metastatic pancreatic cancer. This patient initially exhibited a decline in both CA19-9 and CA72-4 levels, this correlated with clinical and radiological response after initiation of systemic chemotherapy. Both biomarkers remained stable for approximately 6 months, after which an increase in CA72-4 (0.8 U/ml to 4.6 U/ml) and CA19-9 (177 U/ml to 1734 U/ml) was detected, indicating disease progression. A continued rise in both biomarkers was noted, with CA72-4 and CA19-9 levels peaking at 15 and 30 times their baseline level, respectively, at the time of death. While clinical outcomes in our study were based on investigator's assessment, future studies with standardized measures such as RECIST criteria, and health-related quality of life instruments may ensure more accurate results.
Another example of utility of CA72-4 is in patients with pancreatic cancer who do not express CA19-9. This is exemplified by a 67-year-old with widespread metastatic pancreatic cancer with a normal level of CA19-9 despite huge tumor burden. This patient continued to have a normal level of CA19-9 throughout her clinical course which correlated with the level of CA72-4. Interestingly, she was found to be blood type A-positive, an unexpected finding since fucosylation that is required for CA19-9 production as well as Lewis antigen synthesis is not known to be affected in patients of this blood group.
On a cautionary note, CA72-4 may be transiently and falsely elevated in some patients with biliary obstruction. An example of this was that of a patient with advanced pancreatic cancer causing biliary obstruction with a marked elevation of CA19-9 at presentation. The patient underwent biliary stent placement followed by chemotherapy, with resultant decrease in CA19-9. Three months later, an abrupt increase in CA72-4 level (2 U/ml to 14.53 U/ml) was noted. Abdominal imaging revealed stent migration causing recurrent biliary obstruction which required stent exchange. A decrease in CA72-4 was observed with continued normalization of values. Interestingly, the patient's CA19-9 level was unaffected and continued to decline in the setting of biliary obstruction, reinforcing the importance and potential value in combination testing of CA19-9 and CA72-4 in patients prone to biliary obstruction.
In conclusion, through this prospective study we demonstrated that the level of tumor marker CA72-4 varies in different metastatic cancers of gastrointestinal and gynecologic origin, with the highest positivity rates found in pancreatic, ovarian and colorectal carcinomas. This multiyear study, despite its limited sample size, demonstrates that CA72-4 has meaningful correlation with disease activity and may potentially be a useful adjunct to conventional biomarkers in monitoring of various gastrointestinal and gynecologic malignancies.
Acknowledgements
The methodology for the ELISA assay used in the study was developed by DRG International, Inc (NJ, USA). The study was supported in part by DRG International, who provided us with the ELISA Kits, reagents, ELISA Instrument, and gave financial support for technician time to run the assays.
Footnotes
This article is freely accessible online.
Conflicts of Interest
The Authors have declared no conflict of interest or financial disclosures in regard to the study.
- Received May 1, 2017.
- Revision received May 16, 2017.
- Accepted May 19, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.