


Abstract
Aim: The Montgomery-Asberg Depression Rating Scale (MADRS) is one of the most widely used examiner rating instruments for screening, diagnosis and measuring the severity of depression. However, the long-term predictive value of the MADRS in patients admitted to the breast cancer diagnosis unit (BCDU) is unknown. Patients and Methods: In the Kuopio Breast Cancer Study women with breast symptoms were evaluated for the total MADRS score before any diagnostic procedures. The relapse-free survival (RFS) was calculated from the time of diagnosis to the time of first relapse including local relapse, contralateral breast cancer (BC) or metastatic disease. The overall survival (OS) was assessed as the time from the date of diagnosis to the date of last follow-up or death of the patient. The effect of the MADRS on the RFS and on the OS were calculated by Kaplan–Meier survival analysis and the difference between groups was assessed by the log-rank test. The RFS and OS were estimated for the study groups with the low MADRS score (<25) versus the high MADRS score (≥25). The end-point of our study was to determine differences in long-term outcome and in MADRS score in breast cancer (BC), benign breast disease (BBD) and healthy study subjects (HSS). Results: In the Cox proportional hazard model the total MADRS score significantly predicted the 25 year RFS and OS in the HSS, BBD and BC groups combined (HR=2.26, p=0.006; HR=2.46, p=0.008, respectively), and in the Kaplan–Meier survival analysis with the log-rank test the total MADRS score predicted the 25 year RFS and OS in the HSS, BBD and BC groups combined (p=0.005; p=0.006, respectively). Conclusion: The moderate/severe depression (MADRS) can affect the quality of life and outcome among patients admitted to the BCDU.
Breast cancer (BC) is a common malignancy in females accounting for 15-20% of all cancer cases in women and over a half a million women die every year from BC. The worldwide differences in BC incidence are almost four-fold, the highest rate is in Western Europe, 96/100,000 of population, whereas in Africa the rate is 27 cases per 100,000 population population (1). In 2014, 5008 Finnish women were diagnosed with BC (2). A substantial number of well-established or suggested prognostic factors have been elaborated in the literature (3), but only very few are used in clinical decision-making in the treatment of BC. The therapy of BC is based on tumor diameter, nodal status and sex steroid receptor content (3-5). Although, the prognosis of BC has improved gradually due to adjuvant hormonal therapy and chemotherapy, still too many BC patients experience a recurrence and therefore it would be of great importance to identify predictive factors to find the most effective treatment for each patient. In addition, subjects diagnosed with BC are confronted with a stressful situation that can result in anxiety, depression and other forms of psychological morbidity. The three recent papers indicated that 20-40% of patients with BC reported significant distress during the first year after diagnosis (6-8), although psychological distress is often unrecognized and untreated in cancer patients (9).
The Hamilton Depression Rating Scale (HAMD) and the Montgomery-Asberg Depression Rating Scale (MADRS) are the most widely used examiner-report psychometric questionnaires, which health care professionals and researchers use to measure the severity of depression in a variety of settings (10-11). Earlier, we assessed the depression and hopelessness in among patients admitted to the Breast Cancer Diagnosis Unit (BCDU) and the results indicated a highly significant agreement between different psychometric inventories and depression scores and hopelessness measures (12-16). In addition, many studies have investigated the relationship between psychological factors, stress, adverse life events, social support, emotional control and risk of BC (17-36). However, there is no prospective study on whether the moderate/severe depression (MADRS) can affect the quality of life and outcome among patients admitted to the BCDU. Therefore, we carried-out a prospective study to examine the association between the MADRS, and relapse-free survival (RFS) and overall survival (OS) in 25-year cohort in Finland.
Characteristics of the study participants. Results are shown for the patients with breast cancer (BC), for those with benign breast disease (BBD) and for the healthy study participants (HSS).
Patients and Methods
The Kuopio BC Study (KBCS) was a multidisciplinary cooperative project conducted by different departments of the University of Kuopio and Kuopio University Hospital, and included all women who were referred to the hospital for breast examination between April 1990 and December 1995. The KBCS followed the protocol of the International Collaborative Study of Breast and Colorectal Cancer coordinated by the European Institute of Oncology in Milan, and was initiated as a SEARCH program of the International Agency for Research on Cancer. The collaborative study is based on the assumption that BC and colorectal cancer may have common risk factors. Study centres for the BC study are situated in Canada, Finland, Greece, Ireland, Italy, Russia, Slovakia, Spain and Switzerland (38). The study participants showed BC symptoms (a lump in the breast or in the axilla, pain in the breast, bleeding from the nipple, nipple discharge or skin dimpling), or an abnormality of the breast and the indications for referral in this study were in line with our previous investigations in a BC Diagnostic Unit (BCDU) in Finland (39, 40).
This prospective case–control study was approved by the Kuopio University Hospital Board on Research Ethics (approval number 14/12/1989) and was conducted in accordance with the Declaration of Helsinki. All study subjects gave written informed consent to participate in this study. One hundred and fifteen women participated and were interviewed (to determine the level of emotional depression) by a psychiatrist (P.O.) before any diagnostic procedures, so neither the interviewer nor the patient knew the diagnosis at the time of the interview. The interviews were recorded and the ratings were completed before the final diagnosis. The clinical examination, mammography and biopsy showed BC in 34 (29.6%) patients, BBD in 53 (46.1%) patients and 28 (23.4%) HSS (Table I).
Montgomery-Asberg Depression Rating Scale (MADRS). Montgomery and Asberg introduced in 1979 an inventory (MADRS) for rapid screening of depression (11). The examiner (P.O.) completed the MADRS with 10 variables and the MADRS was used as a continuos variable in this study. The questionnaire items measuring depression in the MADRS test are following; 1. apparent sadness, 2. reported sadness, 3. inner tension, 4. reduced sleep, 5. reduced appetite, 6. concentration difficulties, 7. lassitude, 8. inability to feel, 9. pessimistic thoughts, 10. suicidal thoughts. Each MADRS item yields a score of 0 to 6 and the MADRS test with ten variables ranges from 0 to 60 and was rated as follows: grade I, score 0 (n=0), no depression; grade II, score 1-6 (n=25), few depression; grade III, score 7-19 (n=30), mild depression; grade IV, score 20-34 (n=38), moderate depression; and grade V, score 35-60 (n=22), severe depression. In the present study the total MADRS score was used as a continuous variable with the cut-off point 25 for the total MADRS score.
Statistical analysis. Significance of the results was calculated with the SPSS/PC statistical package (SPSS Inc., Chicago, IL, USA). Correlations and differences between the study groups (BC, BBD and HSS groups) were measured with the two-sided chi-square test and non-parametric Kruskal–Wallis variance analyses. The data on relapse-free survival (RFS) and overall survival (OS) were collected and inspected from Kuopio University Hospital registry. The RFS was calculated from the time of diagnosis to the time of first relapse including the local relapse, the contralateral BC or the metastatic disease. The OS was assessed as the time from the date of diagnosis to the date of last follow-up or death of the patient. The effect of the MADRS on the RFS and on the OS were calculated by the Kaplan-Meier survival analysis and the difference between the groups was assessed by the log-rank test. The RFS and OS was estimated for the HSS, BBD and BC groups with the low MADRS score (<25) versus the HSS, BBD and BC groups with the high MADRS score (≥25). The p-values and the hazard ratios (HRs) and their 95 % confidence intervals (CI) were calculated from the Cox proportional hazard models. The p-value 0.05 was considered to be statistically significant.

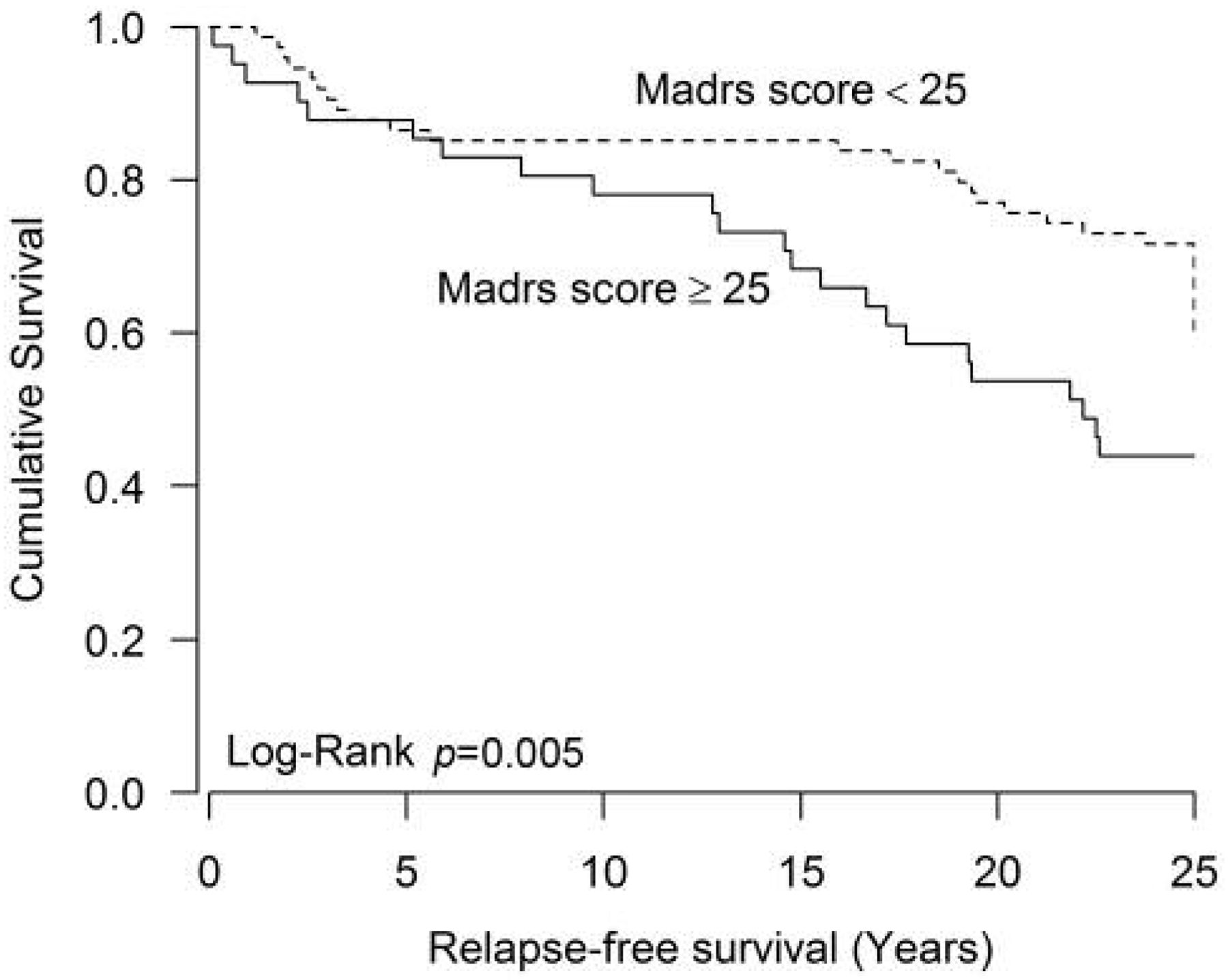
Kaplan-Meier survival curves for relapse-free survival (RFS) for patients with breast cancer (BC), those with benign breast disease (BBD) and for the healthy study participants (HSS) groups combined (n=115) according to total MADRS score. The total MADRS score was a continuous variable for the study patients. The MADRS score had a statistically significant effect on RFS (p=0.005) by the log-rank test.
Results
The study groups did not differ in terms of demographic variables or surgical data. The demographic characteristics and surgical data are presented in Table I with p-values. Although the patients in the BC group were slightly older than those in the BBD and HSS groups (51.5 versus 47.5 and 45.7 years, respectively), the age difference was not statistically significant (p=0.12). The majority of the patients (85/115, 74%) were married or living in a steady relationship. The mean MADRS score values were quite similar in the HSS, BBD and BC groups (p=0.780, Table I) and the groups differed only slightly from each other as to the factors of the reproductive life of the women (Table I).

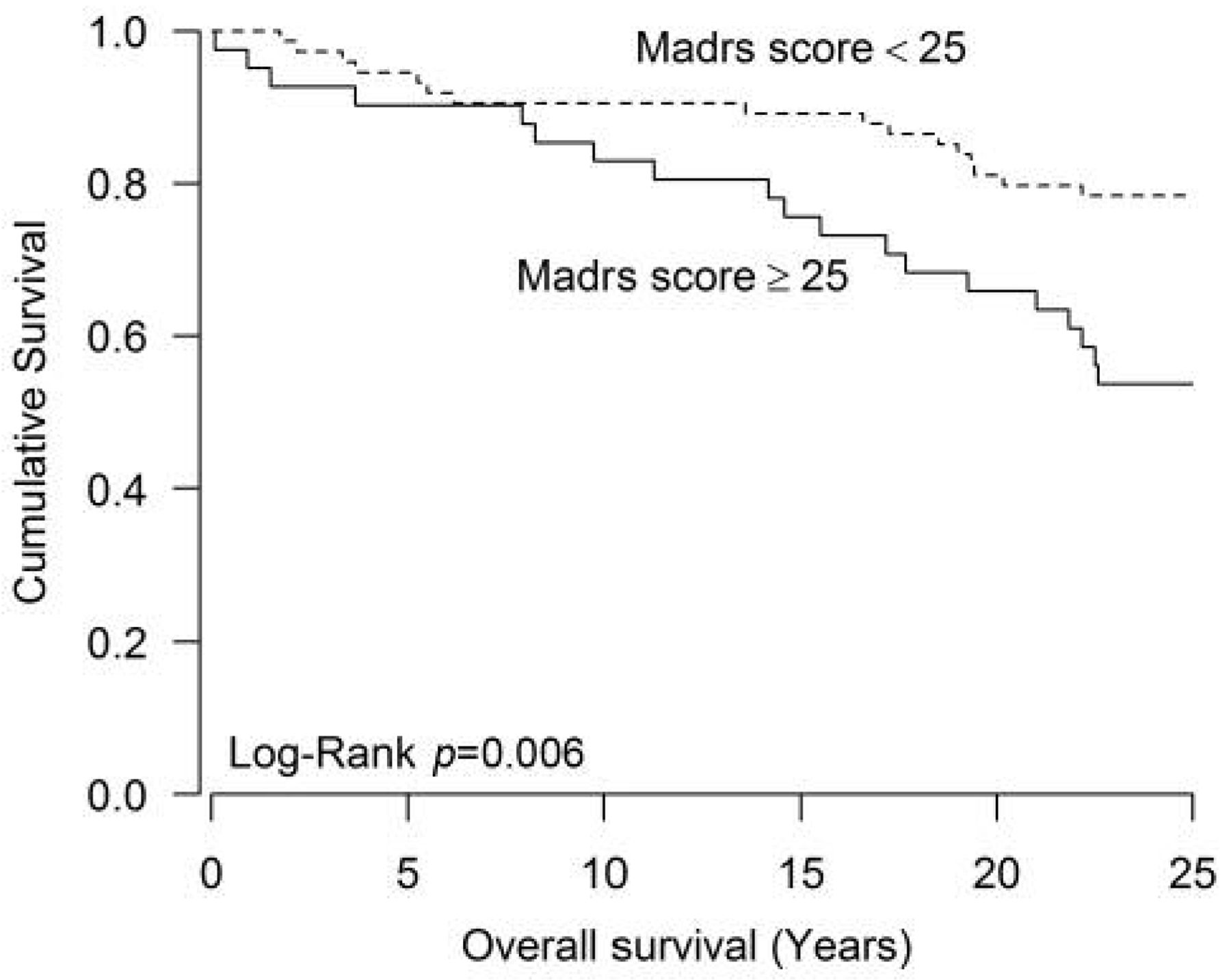
Kaplan-Meier survival curves for overall survival (OS) for patients with breast cancer (BC), those with benign breast disease (BBD) and for the healthy study participants (HSS) groups combined (n=115) according to total MADRS score. The total MADRS score was a continuous variable for the study patients. The MADRS score had a statistically significant effect on OS (p=0.006) by the log-rank test.
In Kaplan-Meier survival analysis with the difference between the groups assessed by the log-rank test, the low total MADRS score (<25) showed as a statistically significant favourable predictor of the RFS (the log-rank p=0.005, Figure 1) and the OS (the log-rank p=0.006, Figure 2). In the Cox regression analysis the low total MADRS score (<25) showed as a statistically significant favourable predictor of the RFS (HR=2.26, 95% CI=1.26-4.06, p=0.006, Table II) and the OS (HR=2.46, 95% CI=1.27-4.79, p=0.008, Table III) in the HSS, BBD and BC groups combined. A similar although statistically insignificant pattern was seen in the HSS and the BBD groups (Table II). The low total MADRS score (<25) versus the high total MADRS score (≥25) differed significantly in the 25-year relapse rate (29.7% vs. 56.1%, Table II). The low total MADRS score (<25) versus the high total MADRS score (≥25) differed significantly in the 25-year survival rate (21.6% versus 46.1%, Table III).
Discussion
BC is considered a hormone-dependent disease (3, 41, 42), because a number of BC risk factors are related to female hormones and to a women's reproductive life such as, low parity or nulliparity, no or little breastfeeding, early age at menarche, late age at menopause, late age at birth of first child, use of oral contraceptives and hormone replacement therapy, are known to be the main risk factors for sporadic BC (3, 41-47). Other life-style factors, such as obesity, smoking, alcohol consumption and lack of physical activity, appear to contribute to an increased risk for this malignancy, although the results concerning such factors are inconsistent (41-47). Although, there is no firm evidence for any mechanism through which psychological distress could affect the neoplasia, BC is a disease with great psychological impact and several mechanism have been suggested for possible psychological variables associated with BC risk (49).
Total MADRS score versus the relapse-free survival (RFS) for the HSS (n=28), BBD (n=53) and BC (n=34) groups and for the study groups combined. The p-values and hazard ratios (HRs) and their 95% confidence intervals (CI) were calculated from the Cox proportional hazard models.
Total MADRS score versus the overall survival (OS) for the HSS (n=28), BBD (n=53) and BC (n=34) groups and for the study groups combined. The p-values and hazard ratios (HRs) and their 95% confidence intervals (CI) were calculated from the Cox proportional hazard models.
Althought the MADRS test is a widely used examiner-rating instrument in depression, the long-term predictive value of MADRS in patients admitted to the BCDU is unknown. The patients who have their diagnosis visit to a BCDU seem to be anxious and psychological distress can arise in the time between lump discovery, follow-up appointments due to abnormal findings, and diagnosis, regardless of whether the diagnosis is a BBD or BC (50, 51). Various factors like the status of social support, marital status, educational level, and the personal psychiatric history may affect on psychological distress in BCDU patients (51-53). Some studies report an association between psychological distress and clinical variables, such as type of treatment and cancer stage. In particular, studies suggest that younger cancer patients have an increased risk for psychological distress (54).
Beck depression inventory (BDI) and MADRS are the most widely used rating instruments for screening, diagnosis and measuring the status of depression. BDI is a patient-rated scale and we have earlier shown that the patient-rated depression in BDI could significantly effect the long-term outcome of women in BCDU (37). The MADRS is a ten-item examiner-rated test, which health care professionals and researchers use to detect depression in normal populations and in different psychiatric patient cohorts. The MADRS was designed in 1979 by British and Swedish researchers as an adjunct to the Hamilton Rating Scale for Depression (HAMD). The MADRS gives more weight to cognitive features of depression, while the HAMD focuses more on the somatic symptoms. There is, however, a high degree of statistical correlation between scores on the two measures (55, 56). Muller et al. (57) estimated the MADRS cut-off scores for moderate and severe depression in relation to the Hamilton Depression Rating Scale (HAMD) and best separation between moderate and severe depression was achieved with a MADRS score of 31 (sensitivity 93.5%, specificity 83.3%). Higher MADRS score indicates more severe depression, and each item yields a score of 0 to 6. The overall score ranges from 0 to 60. However, the definition of moderate and severe depression is still a matter of debate (58, 59), and reliable and clinically useful gradations based on empirical data are required, since there is evidence that different new antidepressants show distinct efficacy depending on the severity of illness (58-60).
From the methodological point of view, the limitation of our study is its small sample size of 115 patients. However, this research question is very specific and therefore we did not expect high number of patients. This could be taken in account when planning new scientific studies of the depression scoring in long-term outcome in the BC patients in the future. In all the study groups, the study subjects were assessed by a psychiatrist; i.e. all ratings of an individual patient were carried out by the same rater and the MADRS score was used as a continuous variable with the cut-off point 25 for the total MADRS score. Therefore, it is unlikely that there is a study bias from the MADRS scoring between the three study groups. Other methodological point, which needs to be further discussed is the possible downsides of MADRS test when used in patients regarding its longer-term predictive capability. HAMD and MADRS differ in their coverage/number of depressive items and the symptoms of atypical depression like hypersomnia or appetite/weight increase are not included. Symptoms of motor retardation are not covered by the MADRS (61).The most frequently used depression rating scales (HAMD, BDI and MADRS) are still considered as ‘gold standards’. However, the ability of each scale to differentiate between healthy (HSS), benign (BBD) and breast cancer patients (BC) and to detect changes during treatment or follow-up may differ in various stages of BC. Therefore, BC patients should have regular follow-up visits in order to identify mental health problems well in time (62).
In conclusion, the results suggest that the MADRS score used as a continuous variable with the cut-off point 25 for the total MADRS score significantly correlates to the 25-year RFS and OS in the HSS, BBD and BC groups.
Acknowledgements
This study was funded by the Heikki, Aino and Aarne Korhonen foundation, Paavo Koistinen Foundation, and EVO funds from Kuopio University Hospital. Our special thanks are due to Ms Anna-Kaisa Lyytinen, R.N. for help in data collection.
Footnotes
Conflicts of Interest
None.
- Received March 2, 2017.
- Revision received March 15, 2017.
- Accepted March 20, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}