


Abstract
Aim: To evaluate the clinical benefit from lateral lymph node dissection for middle and lower rectal cancer. Patients and Methods: A total of 229 patients who underwent bilateral lateral lymph node dissection during resection with curative intent for cT3-4 middle or lower rectal cancer from 2002 to 2013 were retrospectively reviewed. The index of estimated benefit from lymph node dissection for all, and each (common iliac, internal iliac and obturator), lateral lymph nodes were compared with the index for mesenteric lymph nodes (perirectal, intermediate and main lymph nodes). Results: The overall incidence of lateral lymph node metastasis was 14.0%. The index for all lateral lymph nodes (10.6) was lower than perirectal lymph nodes (45.3), but higher than intermediate lymph nodes (4.8). Conclusion: Lateral lymph node dissection provides considerable clinical benefit, similar to the benefit provided by intermediate lymph node dissection.
The incidence of lateral lymph node (LN) metastasis from locally advanced middle and lower rectal cancer is reported to be 14.6-20.1%. It is associated with increased local recurrence and poor overall survival (1-4). In Western countries, lateral LN metastasis is generally considered a metastatic disease and neoadjuvant chemoradiotherapy (CRT) combined with total mesorectal excision (TME) is widely used (5-7). On the contrary, the Japanese Classification of Colorectal Carcinoma (8) defines lateral LNs as regional LNs in the internal iliac (IILN), obturator (OLN) and common iliac (CILN) subregions. The Japanese Society for Cancer of the Colon and Rectum (JSCCR) Guidelines for the treatment of colorectal cancer (3) recommend mesorectal excision with lateral LN dissection (LLD) as standard treatment for locally advanced middle and lower rectal cancer. However, the prognostic benefit of LLD remains unclear.
In this study, the index of estimated benefit from LN dissection (IEBLD), unique method to assess the efficacy of LN dissection (9), was adopted to clarify the therapeutic value of LLD for locally advanced middle and lower rectal cancer.
Patients and Methods
Study design. A prospective colorectal database, which contains information on patients' characteristics, preoperative assessment, operative characteristics, postoperative complications, pathological characteristics and follow-up data, was used for analysis. From September 2002 to June 2013, a total of 389 patients who had been diagnosed with cT3-4 middle or lower rectal adenocarcinoma underwent mesorectal excision with LLD for curative intent at Shizuoka Cancer Center Hospital. First, 21 patients who received neoadjuvant CRT were excluded. Neoadjuvant CRT was used only when resection margin positivity was suspected based on preoperative computed tomography (CT) and magnetic resonance imaging (MRI) findings. Subsequently, 24 patients who had prior treatment for any pelvic malignancy, 33 patients with unilateral LLD and 82 patients with sampling of lateral LNs were excluded. Finally, 229 patients who underwent bilateral LLD were included in this study (Figure 1).
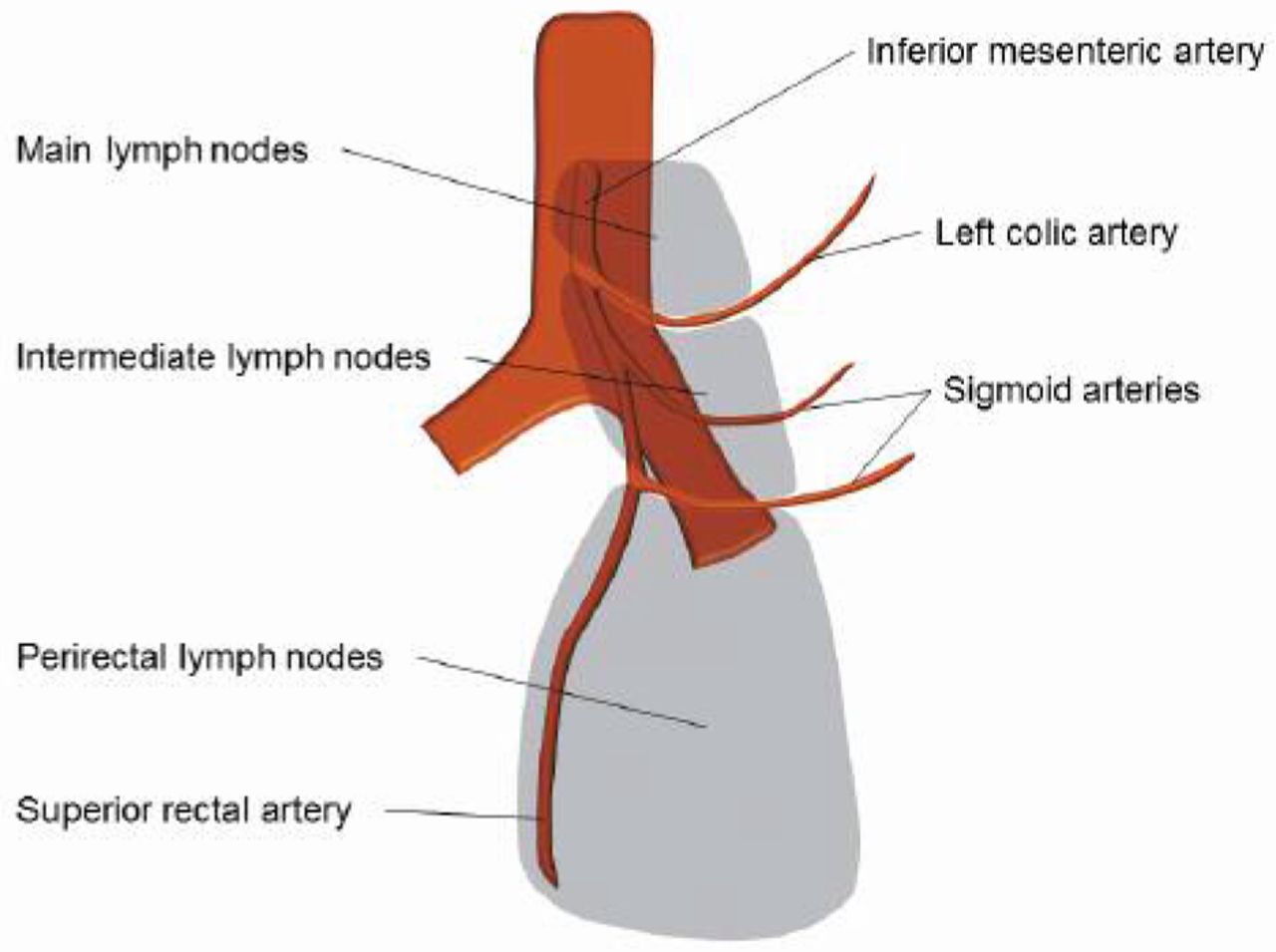
Definition of mesenteric LNs. The Japanese Classification of Colorectal Carcinoma categorizes mesenteric LNs of the rectum into 3 subgroups: perirectal LNs (PLNs), intermediate LNs (ILNs) and main LNs (MLNs) (Figure 2) (8). The MLNs are defined as the LNs at the root of the inferior mesenteric artery (IMA). The ILNs are defined as the LNs around the IMA between the left colic artery and the terminal branch of the sigmoid artery. The JSCCR Guidelines for the treatment of colorectal cancer (3) recommend mesenteric LN dissection that includes the PLNs, ILNs and MLNs for cT2-4 or cN+ rectal cancer.
Indications for LLD. LLD is indicated when the lower border of the tumor is located distal to the peritoneal reflection and has invaded beyond the muscularis propria (cT3-4) in accordance with the JSCCR Guidelines for the treatment of colorectal cancer (3). Patients without lateral LN metastasis on preoperative imaging who were aged over 76 years or at high-risk of postoperative complications due to comorbid conditions did not undergo LLD. In patients diagnosed with lateral LN metastasis on preoperative imaging who were aged over 76 years or at high-risk of preoperative complications due to comorbid conditions, unilateral (metastatic side) dissection or sampling of lateral LNs was performed. Patients aged 75 years or younger who were not at high-risk of postoperative complications underwent bilateral LLD.
Preoperative evaluation included digital rectal examination, colonoscopy, histological examination, CT, MRI and barium enema. Patients were staged using the tumor node metastasis (TNM) staging system in the seventh edition of the American Joint Committee on Cancer (AJCC) Cancer Staging Manual (10). Although the TNM staging system considers lateral LN metastasis as distant metastasis, the present study considers lateral LN metastasis as regional metastasis (4).
LLD operative procedure. Bilateral LLD, including bilateral complete dissection of CILNs, IILNs and OLNs, was performed after removal of the rectum (Figure 3). First, the ureter was identified and mobilized. To dissect the CILNs, the ventral and medial portions of the common iliac artery and vein were exteriorized from the aortic bifurcation. Dissection was performed along the blood vessel wall to the bifurcation of the internal and external iliac arteries. Next, IILNs, located between the internal iliac artery and the autonomic nerves (pelvic splanchnic nerves and pelvic plexus), were dissected. Finally, OLNs were dissected. The border between the internal iliac vessels and OLNs was separated. The lateral surface of the internal pudendal artery was exfoliated to Alcock's canal and the sacral nerves, as well as the coccygeal muscle were exposed. Obturator nerves were preserved and the obturator artery and vein were dissected. The lateral side of the obturator space was exposed to the pelvic wall along the obturator fascia, while the inside of the pelvic wall was dissected to the lateral side of the internal iliac artery. The proximal side was dissected en bloc to the bifurcation of the internal and external iliac arteries (11).
Up to December 2011, when robotic-assisted laparoscopic surgery began at our Institution, rectal cancer surgery with LLD was performed using the open method. Since January 2012, rectal cancer surgery with LLD has also been performed using robotic-assisted LLD (11, 12). Laparoscopic LLD was adopted for patients who prefer not to have robotic or open surgery. The lateral LN resection area was the same regardless of surgical approach.
Evaluation of the therapeutic value of LLD. We adopted the IEBLD to assess the efficacy of LN dissection for each LN region. This index was proposed by Sasako et al. (9) in 1995. It is calculated by multiplying the frequency of LN metastasis in each region by the 5-year survival rate of patients with positive LNs in each region. LN metastasis was recorded separately for each LN region. In this study, the IEBLD was calculated for all lateral LNs, CILNs, IILNs and OLNs. The IEBLD for all lateral LNs represents the benefit from bilateral complete dissection of CILNs, IILNs and OLNs, which was calculated by multiplying the frequency of any lateral LN metastasis by the 5-year survival rate of patients with any lateral LN metastasis. Then, the IEBLD for mesenteric LNs, including all mesenteric LNs, PLNs, ILNs and MLNs, was also calculated and compared to the IEBLD for lateral LNs. Because it is impossible to determine a cut-off level as a definite indication for LN dissection (13), the IEBLD of mesenteric LNs, which are routinely dissected in locally advanced rectal cancer, was used as reference. Previous articles dealing with IEBLD also used the IEBLD of routinely dissected LNs as a reference (14-18).

Consort diagram. LLD, Lateral lymph node dissection, CRT, chemoradiotherapy.
Patients' follow-up. Patients who were diagnosed with pStage III disease underwent adjuvant chemotherapy after the operation for 6 months. Tumor markers were measured every 3 months for 3 years and then every 6 months until 5 years. CT scans were performed every 6 months for 5 years. All study protocols were approved by our Institutional Review Board (No. 28-J58-28-1-3) and informed consent was obtained from all patients.
Statistical analysis. All statistical analyses were performed using EZR (Saimata Medical Center, Jichi Medical University, Saitama, Japan) (19). All p-values were 2-sided and p-values less than 0.05 were considered statistically significant.
Results
Patients' demographic characteristics and pathological findings. Table I summarizes the demographic characteristics and pathological findings of the 229 study patients. The open approach was used in 199 patients (86.9%), compared to robotic in 28 patients (12.2%) and laparoscopic in 2 patients (0.9%). Regarding pT stage, 188 patients (82.1%) had pT3 or pT4 disease. As for pN stage, 122 patients (53.3%) had pN+ disease. Lateral LN metastasis was observed in 32 patients (14.0%). As for pathological stage, 194 patients (84.8%) were diagnosed with Stage II or III disease, while 30 patients (13.1%) had Stage I disease and 5 patients (2.1%) had Stage IV disease. The median number of harvested LNs was 48. The median number of harvested total lateral LNs, CILNs, IILNs and OLNs was 21, 3, 5 and 13, respectively. R0 resection was achieved in all patients.

Schematic image showing the location of the mesenteric lymph nodes, including perirectal lymph nodes, intermediate lymph node (ILNs) and main lymph nodes (MLNs) around the inferior mesenteric artery.
Frequency of LN metastasis and IEBLD for each LN. Table II presents the frequency of metastasis, 5-year overall survival rate of patients with nodal involvement and IEBLD for each type of mesenteric and lateral LNs. The overall incidence of metastasis to mesenteric and lateral LNs was 50.7% and 14.0%, respectively. Among 113 patients without metastasis to mesenteric LNs, the metastasis to lateral LNs was observed in 6 patients (5.3%). The incidence of metastasis to lateral LNs (14.0%) was higher than that of ILNs (5.7%). The 5-year overall survival rate for patients with lateral LN metastasis was significantly worse than the rate for patients without lateral LN metastasis (75.7% vs. 95.2%, p=0.0002) (Figure 4). However, the 5-year overall survival rate was not significantly different between patients with ILN metastasis and lateral LN metastasis (84.6% vs. 75.7%, p=0.88) (Figure 5). The IEBLD for all lateral LNs (10.6) was higher than that for ILNs (4.8). Among the lateral subregions, OLNs and IILNs had nearly identical IEBLDs. CILNs had the same IEBLD (0.5) as MLNs (0.5). Median follow-up for all patients was 60.8 months.
Discussion
Middle and lower rectal cancer are considered to have 2 lymphatic pathways: superior and lateral. Regarding the superior pathway, LN metastasis arises from the perirectal area and spreads along the superior rectal artery to the IMA (20, 21). In Japan, during LN dissection for the superior pathway, ligation at the root of the IMA is usually performed for patients with locally advanced rectal cancer (3). Previous literature from a Western country also described central vascular ligation (CVL) with the mesenteric dissection up to MLNs as an important technique for improving oncologic outcomes (22). On the other hand, the strategy for lateral LN metastasis is different in Japan and Western countries. In Western countries, TME with neoadjuvant CRT has become the standard treatment for locally advanced rectal cancer. On the other hand, mesorectal excision with LLD is the standard treatment for locally advanced middle and lower rectal cancer in Japan. However, the efficacy of LLD has not been fully evaluated in a prospective study. The recommendation for LLD in the JSCCR Guidelines for the treatment of colorectal cancer is based on a nation-wide observational study. Sugihara et al. found that the incidence of lateral LN metastasis was 20.1% among patients who underwent LLD. They found that the risk of local recurrence decreased by 50.3% and the 5-year survival rate improved by 8% when LLD was performed for T3-4 middle and lower rectal cancer (2). In addition, Akiyoshi et al. reported that patients with lateral LN metastasis localized to IILNs and N2a patients have a similar prognosis, while patients with metastasis to lateral LNs other than IILNs have a poorer prognosis. However, their prognosis is similar to that of N2b patients and better than that of Stage IV patients who underwent curative resection (4). These 2 studies are retrospective in nature and have the limitations inherent to this type of study design. Recently, a multi-center randomized controlled trial comparing mesorectal excision with and without LLD for clinical Stage II or III middle and lower rectal cancer was carried out in Japan. In the analysis of short-term outcomes, Fujita et al. and Saito et al. reported that the morbidity and urogenital dysfunction were not significantly different between mesorectal excision alone and mesorectal excision with LLD, which demonstrated the safety and feasibility of LLD (23, 24). The results of the primary analysis have not yet been published. However, the efficacy of LLD for all cT3-4 cancers will not be clarified by this trial because patients with clinical lateral LN metastasis detected with preoperative imaging were excluded. Thus, the present study attempted to evaluate the therapeutic value of LLD relative to the value of dissecting mesenteric LNs in patients with cT3-4 middle and lower rectal cancer, including those with clinical lateral LN metastasis.
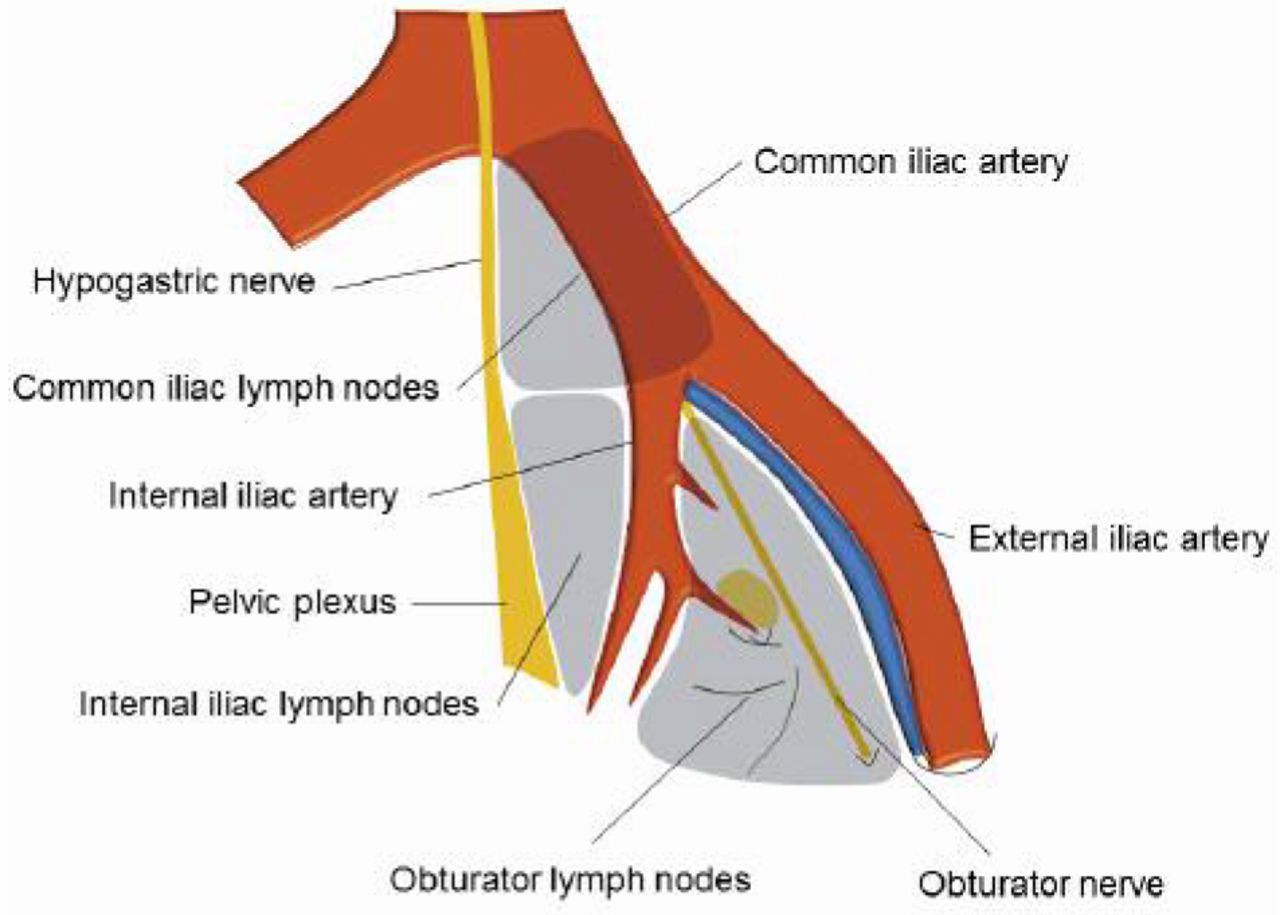
Schematic image showing the location of the left lateral lymph nodes, including the common iliac lymph nodes (CILNs), internal iliac lymph nodes (IILNs) and obturator lymph nodes (OLNs).
Demographic characteristics and pathological findings of our patient cohort (n=229).
The Japanese Classification of Colorectal Carcinoma (8) distinguishes ILNs from PLNs, partly because metastasis to ILNs is associated with poorer prognosis than metastasis to PLNs (25). Japanese surgeons generally consider ILN dissection to be essential because the JSCCR Guidelines for the treatment of colorectal cancer recommend LN dissection up to ILNs even for T1 rectal cancer. Recently, accompanied by the widespread acceptance of the CVL technique (22), the importance of ILN dissection has become globally accepted.
The present study showed that the overall incidence of lateral LN metastasis was 14.0%, which was in accordance with previous reports (14.6-20.1%) (1-4). The IEBLD for all lateral LNs reached 10.6, which was higher than the IEBLD for ILNs (4.8%). This result was due to the fact that (i) survival was achieved after LLD in patients with lateral LN metastasis, and (ii) the rate of lateral LN metastasis was higher than that of ILN metastasis. This result is consistent with a previous report by Ueno et al. (13). They reviewed 244 patients with middle or lower rectal cancer who underwent LLD using IEBLD with the objective of identifying parameters related to prognostic benefit. They found that the IEBLD for lateral LNs (9.9%) was higher than the IEBLD for LNs around the superior rectal artery (4.2%).
Information about the distribution of lateral LN metastasis is another important result of the present study. The evaluation of metastasis to each subregion using data from a single center has the advantage of avoiding region-to-region migration because the borders around each lateral LN group may differ by institution, which is affected by surgical technique or anatomical understanding. The present study revealed that the rates of IILN (7.4%) and OLN (8.3%) metastasis were similar. Among 32 patients with lateral LN metastasis, 31 (96.9%) patients had metastasis to either IILNs or OLNs. There have been very few studies demonstrating the distribution of lateral LN metastasis. Ueno et al. (13), who divided the IILNs into proximal and distal IILNs based on the superior vesicular artery as a landmark, reported that the incidence of metastasis to any lateral LNs, proximal IILNs, distal IILNs and OLNs was 16.8%, 6.1%, 9.4% and 4.1%, respectively. They also described the IILNs and OLNs as a ‘vulnerable field’ because 87.8% of patients with lateral LN metastasis had metastasis in this field. Yokoyama et al. analyzed 131 consecutive patients with locally advanced middle or lower rectal cancer who underwent LLD. The incidence of metastasis to any lateral LNs, IILNs and OLNs was 19.1%, 12.2% and 9.9%, respectively. They also found that 96.1% of patients with lateral LN metastasis had metastasis to either IILNs or OLNs (26). The present work and the aforementioned previous studies found that most lateral LN metastases occur in the IILNs or OLNs. Both prior studies have demonstrated a higher incidence of IILN metastasis than OLN metastasis, which is not consistent with our results. This may be explained by region-to-region migration, as previously mentioned.

Five-year overall survival in patients with and without lateral lymph node metastasis. 5Y OS, Five-year overall survival.
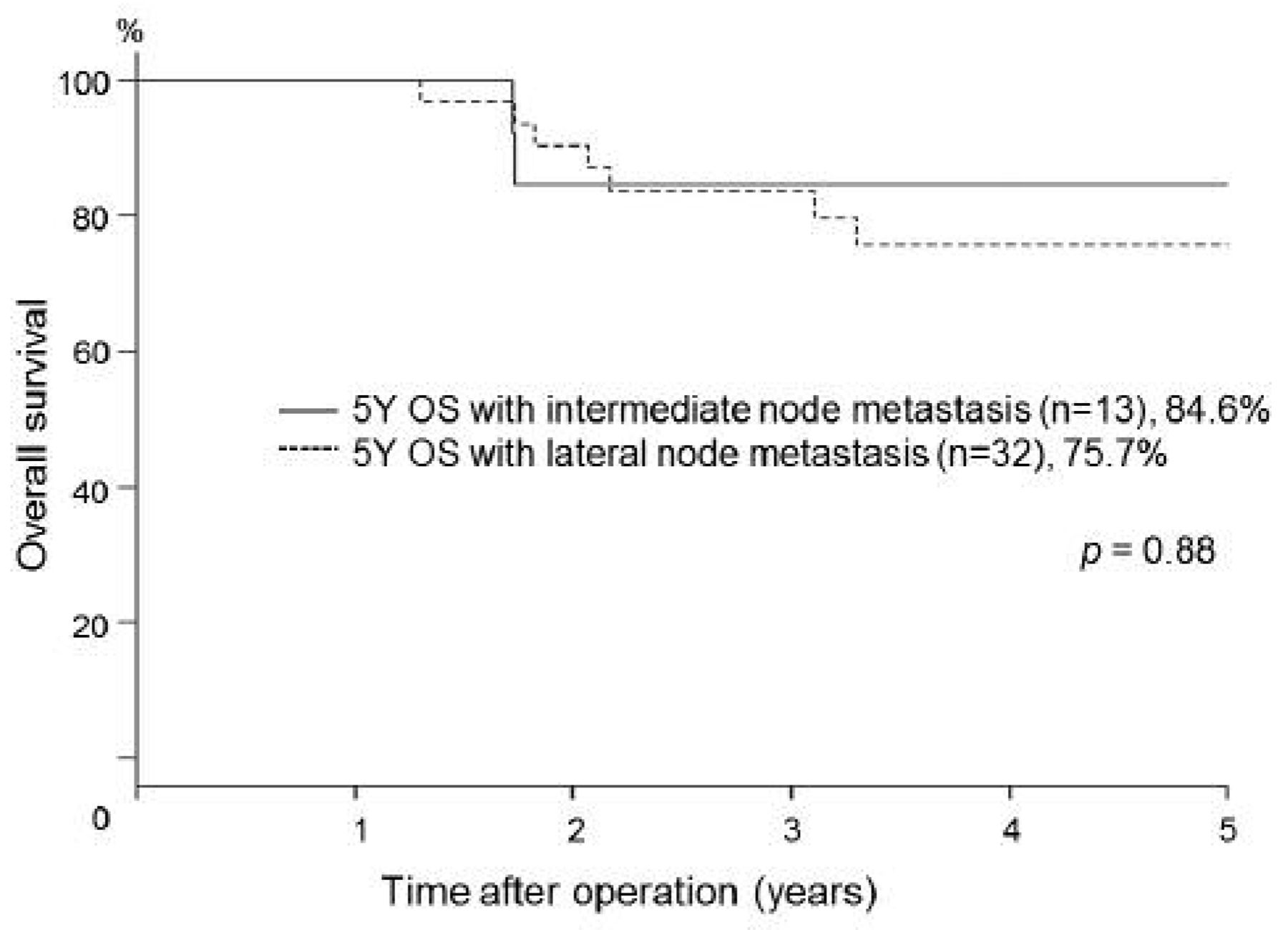
Five-year overall survival in patients with intermediate or lateral lymph node metastasis. 5Y OS, Five-year overall survival.
Frequency of metastasis, 5-year survival and IEBLD for each type of lymph node (n=229).
Another noteworthy finding of the present study was that the IEBLD for OLNs was not inferior to the IEBLD for IILNs. In the present work, the 5-year overall survival rate and IEBLD of patients with metastasis to OLNs were comparable to those with IILN metastasis. This result supports the fact that Japanese surgeons consider OLN metastasis to be regional LN metastasis, whereas the seventh edition of the AJCC Cancer Staging Manual considers OLN metastasis to be distant disease. The IEBLD for CILNs and MLNs were identical (0.5%). However, there were only a few patients with metastasis to these subregions (0.9% and 0.9%), which made it difficult to specify the therapeutic value of dissecting these subregions.
There are several potential limitations in the present study. First, there might be a selection bias in which patients received LLD. Patients without lateral LN metastasis on preoperative imaging over 76 years of age or at high-risk of postoperative complications due to comorbid conditions did not undergo LLD. This selection bias may affect the incidence of lateral LN metastasis and overall survival. The second limitation is that the present data excluded 21 rectal cancer patients with neoadjuvant CRT as this approach has been reported to significantly decrease the number of harvested LNs (27), which might affect the number of harvested LNs and incidence of metastasis. The third limitation is sample size. The patient cohort of the present study included 229 patients with 32 patients having metastasis to lateral LNs. This number may not be enough to present the 5-year overall survival rate of patients with metastasis to lateral LNs. With these limitations, this retrospective study has to be considered as complementary research for revealing the clinical benefit of LLD.
In conclusion, the present study suggests that patients with locally advanced middle and lower rectal cancer can receive similar therapeutic benefit from LLD and ILN dissection. A prospective study is needed to confirm the efficacy of LLD for middle and lower rectal cancer.
- Received February 1, 2017.
- Revision received April 5, 2017.
- Accepted April 6, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}