


Abstract
Background/Aim: Lung cancer is the first cause of cancer related deaths in both males and females. Epithelial–mesenchymal transition (EMT) is a reversible process by which epithelial cells transform to mesenchymal stem cells by losing their cell polarity and cell-to-cell adhesion, gaining migratory and invasive properties. High levels of E-cadherin are expressed in epithelial cells, whereas mesenchymal cells express high levels of N-cadherin, fibronectin and vimentin. The aim of this study was to evaluate the correlation between E-cadherin and vimentin expression and their clinical significance in non-small cell lung cancer (NSCLC). Materials and Methods: The immunohistochemical expression of E-cadherin, vimentin and Ki-67 was performed on tissue microarrays from NSCLC specimens obtained from 112 newly- diagnosed cases and were studied using classical pathological evaluation. Associations between E-cadherin, vimentin and Ki-67 expression, clinicopathological variables and survival were analyzed. In all cases, a value of p≤0.05 was considered significant. Results: Low E-cadherin expression was significantly correlated with tumor necrosis (p=0.019). Moreover, there was a trend for correlation between high E-cadherin expression and better overall survival (hazard ratio=1.02, and 95% confidence interval=0.45-1.87, p=0.091). There was also a significant negative correlation between vimentin expression and overall survival (hazard ratio=1.13, and 95% confidence interval=0.78-1.65, p=0.026). Additionally, there was a significant negative correlation between vimentin expression and grade I tumors (p=0.031). Finally, a positive correlation trend between vimentin expression and Ki-67 was found (p=0.073). Conclusion: High E-cadherin and low vimentin expression correlate with better prognosis and overall survival.
- E-Cadherin
- vimentin
- epithelial mesenchymal transition (EMT)
- non-small-cell lung cancer (NSCLC)
- biomarker
- prognosis
Lung cancer is the first cause of cancer-related deaths in both males and females. It is a fatal disease and most patients with lung cancer will die of their disease (1). Two main types of lung cancer exist: non-small-cell lung cancer (NSCLC) accounting for 85-90% of lung cancer cases, and small-cell lung cancer (SCLC), whose incidence seems to have decreased over the past decades (2). The current therapeutic approach for lung cancer includes surgical tumor removal, platinum-based chemotherapy, targeted therapy, immunotherapy and radiation therapy. Improvements in clinical and molecular understanding of the disease have resulted in novel therapeutic approaches. Multiple genetic and epigenetic abnormalities results in both oncogene activation [epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK)] and inactivation of tumor-suppressor genes [transcription factor (p53) and retinoblastoma protein (RB)] (3). Moreover, angiogenesis seems to play an important role in the process of invasion and metastasis in lung cancer (4). Other molecular and cellular processes of lung cancer include genomic instability, escape from apoptosis, cell immortalization, abnormalities in immune response and epithelial-mesenchymal transition (EMT) (5-9).
EMT is a reversible process by which epithelial cells transform to mesenchymal stem cells by losing their cell polarity and cell-to-cell adhesion, gaining migratory and invasive properties. It is the step by which an early tumor stage converts to an invasive one (9-11). Subsequently, the opposite process occurs: mesenchymal-epithelial transition (MET). For EMT transformation, epithelial cancer cells express mesenchymal proteins such as vimentin, fibronectin, N-cadherin and matrix metalloproteases, and become mesenchymal cells, ready for migration (12-14). During MET, cancer cells repossess the epithelial phenotype and reduce their expression of mesenchymal proteins including vimentin (15).
Vimentin, an important marker for EMT, is an intermediate filament type III, expressed in various non epithelial cells, particularly in mesenchymal ones (16). It is found in the cytoplasm and its role is to stabilize the cytoskeleton with microfilaments and microtubules (17-19). Vimentin is overexpressed in epithelial cancer types such as prostate, breast and lung cancer, while high expression levels are associated with poor prognosis (20). On the other hand, high E-cadherin levels are expressed in epithelial cells. E-Cadherin is a transmembrane protein that plays an important role in cell adhesion. More precisely, the extracellular domain of E-cadherin is responsible for cell adhesion and the intracellular domain interacts with catenin and connects to the actin cytoskeleton (21-22). Low E-cadherin expression has been observed in cancer cells and is related to advanced disease (21-24).
The aim of this study was to evaluate the correlation between E-cadherin and vimentin expression levels and clinicopathological variables and their clinical significance in NSCLC.
Materials and Methods
Study patients. One hundred and twelve patients (93 men and 19 women) diagnosed with newly diagnosed primary NSCLC were enrolled in this study. Disease diagnosis was based on pathological examination. Their medical records were reviewed in order to collect the following parameters: age, gender, performance status, smoking habit, pathological data (histological type, grade, lymphovascular invasion, inflammation, necrosis and fibrosis), disease stage (TNM according to the seventh edition of AJCC) (25) and overall survival. Baseline characteristics of the patients enrolled are presented in Table I that was published in one of our previous studies (26). The mean age of patients analyzed was 63.6 years and the median age 64 years. The majority of cases were adenocarcinomas (52.7%). The mean and median monitoring duration were 27.5 and 17.5 months, respectively. All the participants gave their written informed consent to this study and this study conforms to the Declaration of Helsinki.
Tissue microarrays and immunohistochemistry. We collected tissues by sampling one representative tissue core, 1 mm in diameter chosen from each formalin-fixed, paraffin-embedded tumor specimen (27-30). The sections of tissue microarrays (TMAs) were dewaxed using xylene and rehydrated through graded alcohols. During the process, a blocking reagent (Snipper, Biocare Medical, Walnut Creek, CA, USA) was used to block non-specific antibody. Three binding targeted mouse monoclonal antibodies were then used to detect E-cadherin (Dako, Glostrup, Denmark), vimentin (Abcam, Cambridge, UK) and Ki-67 (Dako) expression. Antigen retrieval was performed by microwaving slides for 15 min at 720 W in 10 mM citrate buffer (pH 6.0) and then incubating them for 1 h at room temperature with the primary antibodies. The dilutions for E-cadherin, vimentin, and Ki-67 were 1:100, 1:200 and 1:100 in phosphate-buffered saline (PBS), respectively. The samples were washed with PBS (three times), incubated with biotinylated linking reagent (Biocare Medical, Walnut Creek, CA, USA) and then with peroxidase-conjugated streptavidin label (Biocare Medical, DAB; Sigma, Saint Louis, MO, USA). Furthermore, the primary antibody was omitted and substituted by an irrelevant anti-serum antibody in negative controls. As positive controls, tumor tissue sections with known high E-cadherin, vimentin and Ki-67 expression were used (normal human urothelium, normal human fibroblasts and normal human tonsil, respectively). The evaluation of immunohistochemistry was carried out by two independent pathologists using classical pathology methods (semi-quantitatively evaluation). Particularly, two parameters were evaluated, the intensity of staining (weak or diffuse while background staining considered negative) and the percentage (%) of tumor cells stained (both membranous and cytoplasmic for E-cadherin and vimentin while nuclear for Ki-67 positivity).
Demographic clinical and pathological features of patients (n=112) (26).
Statistical analysis. Correlations of E-cadherin, vimentin and Ki-67 expression levels in NSCLC tissue with patient characteristics (clinicopathological variables) were identified by using chi-square test. Kaplan–Meier method was used in order to create the survival curves and any differences detected were compared with the log-rank-test. Correlation between potential prognostic marker and overall survival was analyzed by a Cox proportional-hazard regression model. Cox regression analysis was conducted at both univariate and multivariate levels. In all cases, an alpha level of <0.05 was considered significant. SPSS program for Windows performed the statistical analysis (version 13.0; SPSS Inc., Chicago, IL, USA).
Association between the expression of E-cadherin and clinicopathological data of patients (n=112).
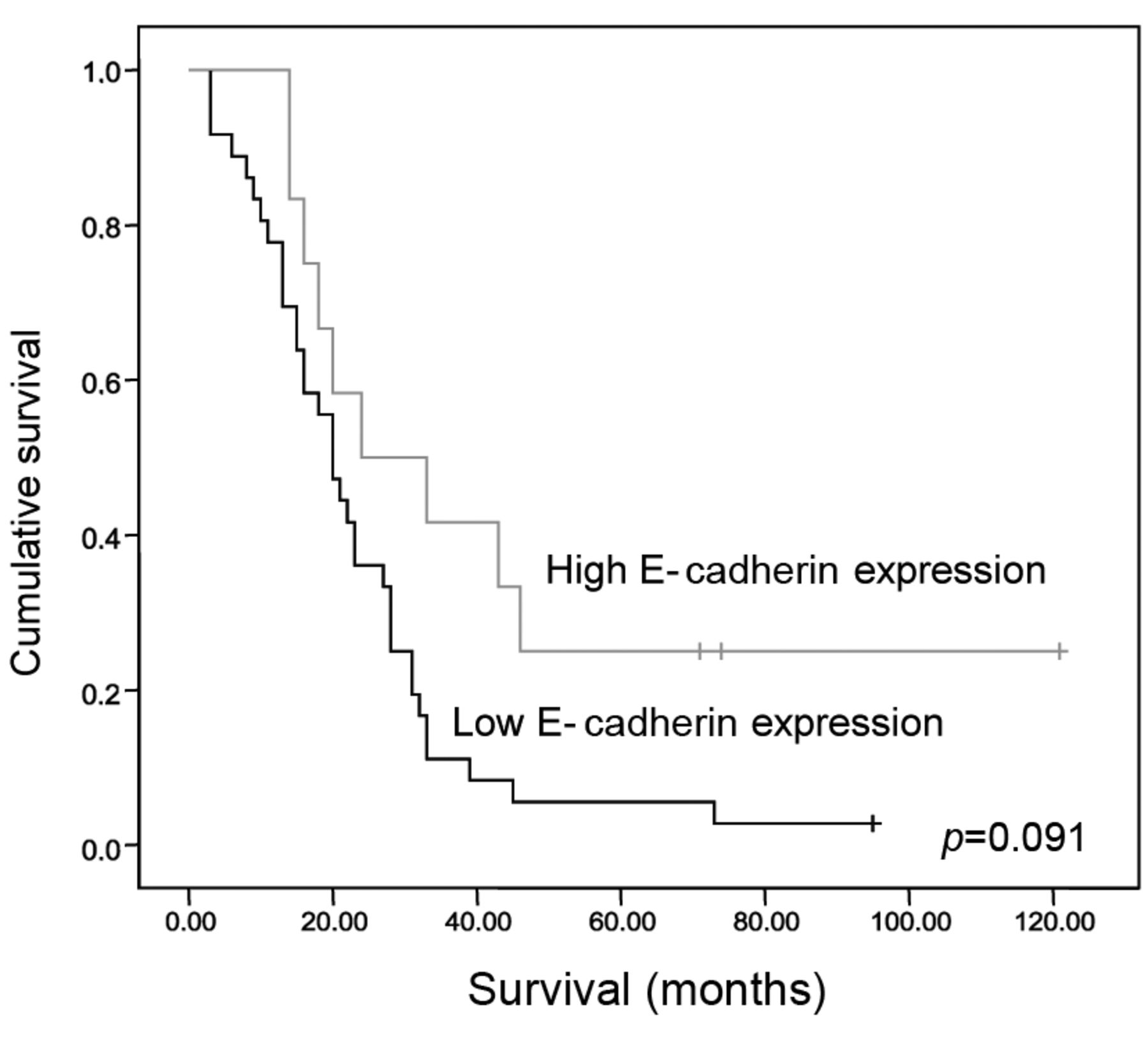
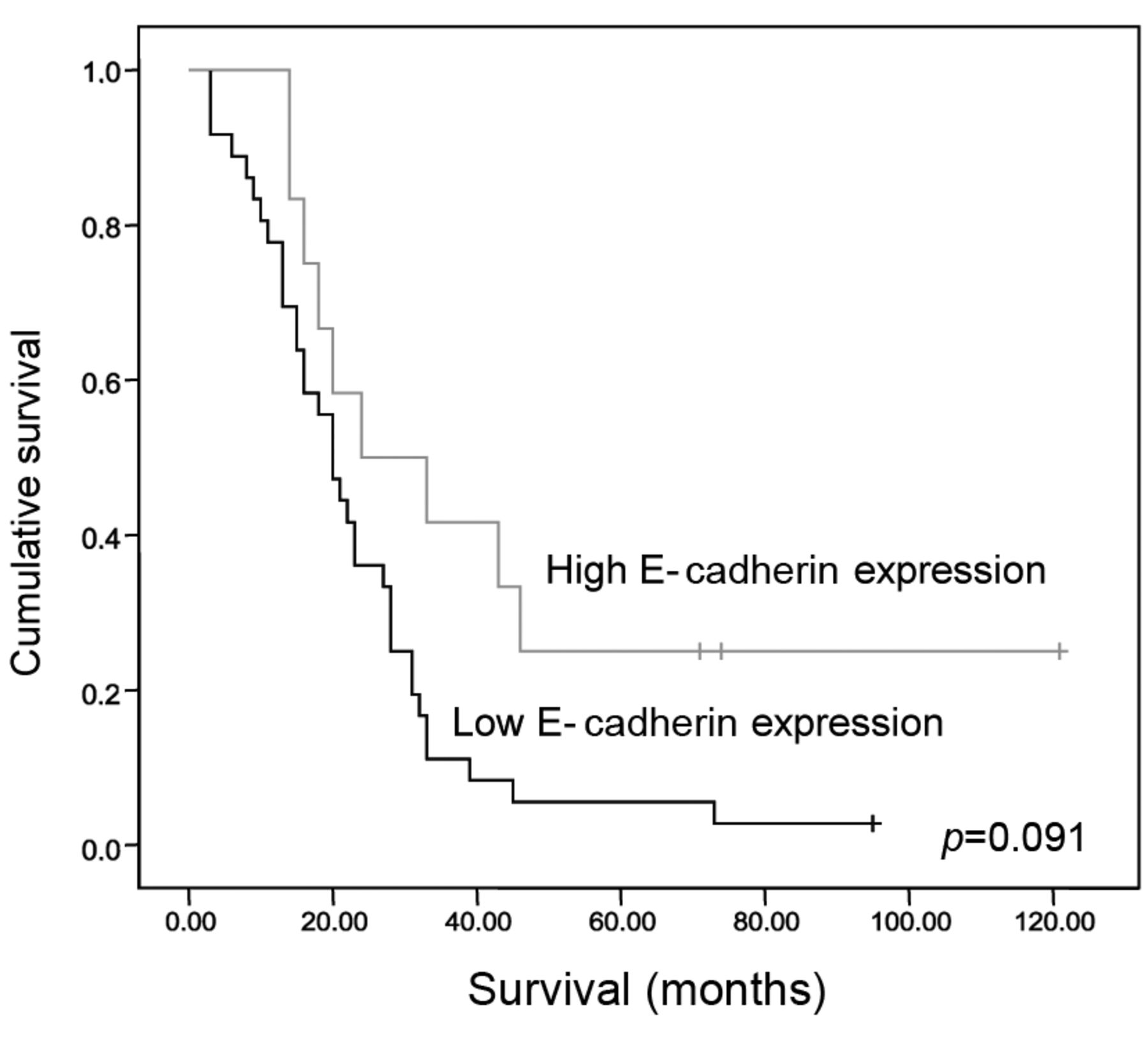
Kaplan-Meier survival analysis according to E-cadherin expression.
Results
The median expression value was used to separate patients into two groups according to whether immunohistochemical E-cadherin expression was above (high expression) or below (low expression) the median value. E-Cadherin expression was high in 57 patients (57/112, 51%) and low in 55 patients (55/112, 49%) (Table II). Notably, low E-cadherin expression was significantly correlated with tumor necrosis (p=0.019). On the contrary, E-cadherin expression was not significantly associated with age, gender, smoking status, alcohol use, performance status (PS), histological type, grade, stage of disease, primary tumor (T), lymph nodes (N), metastasis (M), lymphovascular invasion, inflammation or fibrosis (Table II). There was no correlation between E-cadherin and Ki-67. We found a trend for positive correlation between high E-cadherin expression and overall survival (HR=1.02, 95% CI=0.45-1.87, p=0.091) (Figure 1).
Similarly, the median expression value was used to separate patients into two groups according to immunohistochemical vimentin expression (Table III). There was a significant negative correlation between vimentin expression and grade I tumors (p=0.031). Vimentin expression was not significantly associated with age, gender, smoking status, alcohol use, performance status (PS), histological type, stage of disease, primary tumor (T), lymph nodes (N), metastasis (M), lymphovascular invasion, inflammation, necrosis or fibrosis (Table III). Also, there was a trend for positive correlation between vimentin expression and Ki-67 (p=0.073). Finally, there was a significant negative correlation between vimentin expression and survival (hazard ratio=1.13, 95% confidence interval=0.78-1.65, p=0.026) (Figure 2).
Association between the expression of vimentin and clinicopathological data of patients (n=112).

Kaplan-Meier survival analysis according to vimentin expression.
Discussion
A crucial step in cancer progression is the migration of cancer cells through close lying tissues and vessels to distant tissues. EMT is a mechanism mediating this process (2). As epithelial cancer cells decrease their expression of epithelial proteins, lose cell–cell adhesion and express mesenchymal proteins, the cytoskeleton is remodeled (9-11). Many studies have investigated EMT in different cancer types (5-14). In the present study, we analyzed the expression of the mesenchymal marker vimentin and of the epithelial cell marker E-cadherin in tumor cells of patients with NSCLC in order to correlate these proteins with clinicopathological parameters as well as overall survival.
The most important conclusions of this study was to point out are the significant negative correlation between vimentin expression and overall survival (hazard ratio=1.13, 95% confidence interval=0.78-1.65, p=0.026) and the trend for correlation between higher E-cadherin expression and better overall survival (hazard ratio=1.02, 95% confidence interval=0.45-1.87, p=0.091). Higher expression of vimentin in tumor samples implies a more aggressive type of tumor and a worse overall survival. These data confirm the role of EMT process in the evaluation of lung cancer and are similar to other studies in several cancer types including NSCLC cell lines, colorectal, thyroid, head and neck and bladder cancer (31-36).
Moreover, low E-cadherin expression was significantly correlated with tumor necrosis (p=0.019). It is known that necrosis is an independent risk factor in survival and tumor recurrence in patients with NSCLC (37), implying that E-cadherin expression is associated with favorable prognosis. Also according to our results, there was a significant negative correlation between vimentin expression and grade I tumors (p=0.031). These findings suggest that low expression of vimentin is related to well-differentiated tumors. These data are similar to those of the literature as vimentin expression is associated with an aggressive tumor phenotype (38-40). E-Cadherin and vimentin expression were not significantly associated with other clinicopathological parameters in this study.
A variety of markers has been studied or is under investigation in NSCLC in order to thoroughly understand disease progression (26, 41-43). EMT is one of the pathways for NSCLC progression. In particular, there are data suggesting the involvement of EMT not only in the prognosis of patients with NSCLC but also in the response to specific treatments such as anti-EGFR therapies that are used nowadays for this tumor type (44). Additionally, there are data regarding the possibly implication of EMT in response to treatment with ALK inhibitors among patients with EML4–ALK NSCLC (45). Finally, there are some data referring to possible ways for reversion of the EMT in NSCLC, such as blocking muscarinic receptor signaling in vitro and in vivo, indicating that probably non-neuronal acetylcholine promotes EMT partially through activation of muscarinic receptor M2R (46).
Inevitably, we recognize that there are some limitations to our study. This was a small study with 112 tissue samples with NSCLC. Another limitation is the fact that the evaluation of vimentin and E-cadherin expression were done using only immunohistochemistry. Besides that, apart from E-cadherin and vimentin, there are other markers of EMT phenomenon such as N-cadherin and fibronectin which could be studied. Therefore, more and larger studies are required to reinforce these data and the role of EMT in NSCLC.
In conclusion, there are data suggesting that EMT plays an important role in carcinogenesis and metastasis. In the past decades, an increased number of studies have shown that EMT is associated with poor prognosis in different tumor types including NSCLC. Our data strengthen these data. Further investigation of EMT in NSCLC is needed in order to elucidate its role in the process of cancer development and metastasis. Possibly, in the future detection of EMT could be used not only for a better stratification of patients with NSCLC concerning their prognosis but also for the development of new therapeutic approaches.
Footnotes
↵* These Authors contributed equally to this study.
This article is freely accessible online.
Conflicts of Interest
No potential conflicts of interest exist. No financial support was granted.
- Received February 16, 2017.
- Revision received March 20, 2017.
- Accepted March 21, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Breast cancer progression and metastasis to lymph nodes reveals cancer cell plasticity and MHC class II-mediated immune regulation
- Magnolol Induces Apoptosis Through Extrinsic/intrinsic Pathways and Attenuates NF-{kappa}B/STAT3 Signaling in Non-small-cell Lung Cancer Cells
- Vimentin overexpression as a novel poor prognostic biomarker in eyelid sebaceous gland carcinoma
- Clinical and Prognostic Significance of Neoplastic Spindle Cells in Gallbladder Cancer
- The Mesenchymal-Epithelial and Epithelial-Mesenchymal Cellular Plasticity of Liver Metastases with Digestive Origin
- NHERF1 Suppresses Lung Cancer Cell Migration by Regulation of Epithelial-Mesenchymal Transition