


Abstract
Background: CD98 expression is high in various human neoplasms. However, the relationship of CD98 expression with the clinicopathological factors of gastric cancer (GC) remains unclear. This study examined CD98 expression and its clinicopathological impact on GC. Patients and Methods: Three hundred and thirty-one patients with surgically resected GC were evaluated. Tumor sections were stained and analyzed using immunohistochemistry to assess CD98 expression. Results: CD98 was positively expressed in 19% (66/331) of our patient cohort. Increased CD98 expression was significantly associated with advanced GC stage, lymph node metastasis, non-signet histology, lymphatic permeation, and vascular invasion. Positive CD98 expression was also a significant prediction marker for unfavorable prognosis postoperatively. However, CD98 was not identified as GC's independent prognostic predictor. Conclusion: CD98 could be a novel prediction marker for worse prognosis in GC-affected patients. Our data suggests that increased CD98 expression plays an essential role in tumor aggressiveness and metastasis.
Gastric cancer (GC) is the most common malignancy of gastrointestinal neoplasms. Recent improvement in survival after treatment is observed; however, patients with advanced GC still have low survival despite standard chemotherapy. Moreover, no established biomarker can predict survival outcomes and responses after therapeutic modalities, such as surgery or systemic chemotherapy. Thus, finding a viable predictive biomarker in GC-affected patients is crucial. The CD98 family comprises of widely expressed cell surface heterodimer proteins composed of a glycosylated heavy and a non-glycosylated light chain. Particularly, CD98 is a disulfide-linked 125-kDa heterodimeric membrane glycoprotein; it has been described to be associated with cellular proliferation, transformation, adhesion and the L-type amino acid transporter (LAT) system (1, 2). CD98 (4F2hc) expression is elevated in various human neoplasms, such as lung, pancreatic, biliary tract, breast, prostate, and head and neck cancers; hepatocellular carcinoma; and myeloma (3-12). Moreover, it has been reported that increased CD98 expression is significantly associated with shorter survival outcomes, tumor cell proliferation, and metastases (8). CD98 assists in transporting many amino acids in a cooperative function with L-type amino acid transporter 1 (LAT1) and xCT on the membranous surface of cancer cells (9). The LAT1 expression is elevated in various human cancers (2). We have previously reported that enhanced LAT1 expression is a significant prognostic marker correlated with tumor cell proliferation, angiogenesis, and CD98 expression level (3, 4, 8, 9). Recently, Ichinoe et al. described that LAT1 overexpression is closely associated with worse survival and lymph node metastases. However, since only 87 patients with GC were examined by immunohistochemistry against LAT1, this observation could be biased because of the small sample size. In the same study, LAT1 was also found as an effective predictor for non-scirrhous gastric cancer (13). Inhibition of LAT1 suppresses cancer cell growth via the mTOR signaling pathway (14). As a novel mechanism, LAT1 inhibition causes cell-cycle arrest at G1 phase and several studies reported apoptosis in some cell lines upon LAT1 inhibition (15, 16). Although CD98 expression levels are closely correlated with LAT1 expression, the mechanism of CD98 inhibition and tumor suppression in various human neoplasms remain unclear. Recent reports demonstrated CD98 as an attractive target for cancer treatment (4, 8). However, it remains unknown whether CD98 is associated with survival outcomes and clinicopathological factors in GC-affected patients. To bridge this gap in knowledge, we investigated the impact of CD98 expression on the pathological dynamics of GC-affected patients.
Patients and Methods
Patients. Under the retrospective design of the study herein, 331 patients were selected who underwent surgery for GC at the Gunma University Hospital between January 2000 and December 2009. All clinicopathological data such as age, gender, histology, lymphatic permeation, vascular invasion, lymph node metastasis, and disease staging, were obtained from the institution database. Data were retrospectively analyzed. The Institutional Review Board of Gunma University Hospital (Gunma University Faculty of Medicine's Ethical Committee for Clinical Studies) approved this study. Patients' age ranged from 28 to 90 years, and the median age was 69 years. None of the patients had received neo-adjuvant chemotherapy. All surgical specimens were reviewed and classified according to the WHO classification by an experienced pathologist, blinded to clinical or imaging findings. Pathological tumor–node–metastasis stages were established using the International System for Staging adopted by the American Joint Committee on Cancer and the Union Internationale Contre le Cancer. In our analysis, the clinicopathological factors such as tumor differentiation, lymphatic permeation and vascular invasion were used. In terms of histology, all patients had adenocarcinoma (AC); 181, 66, 64, and 20 patients had stage I, II, III, and IV tumors, respectively. The day of surgery was considered the starting day for measuring postoperative survival. The follow-up duration ranged from 72 to 5,430 days (median, 2,047 days). As a comorbid disease in our study, 125 patients were treated with a medication for hypertension. The author's approach for the evaluation and resection of these tumors has been previously described (17).
Immunohistochemical staining. CD98 expression was determined by immunohistochemical staining using an anti-CD98 antibody. The anti-CD98 antibody is an affinity purified rabbit polyclonal antibody (Santa Cruz Biotechnology, Inc, Dallas, TX, U.S.A. 1:100 dilution) raised against a peptide mapping at the C-terminus of human CD98 (3, 4, 10-12). Immunohistochemical staining was performed on paraffin sections using a polymer peroxidase method (Histofine Simple Stain MAX PO (MULTI) kit; Nichirei Corporation, Tokyo, Japan). Deparaffinized, rehydrated sections were briefly treated with 0.3% hydrogen peroxidase in methanol for 30 min to block endogenous peroxidase activity. After rinsing in phosphate-buffered saline, the sections were incubated with the anti-CD98 antibody (1:100) overnight. Thereafter, sections were incubated with the Histofine Simple Stain MAX PO (MULTI) kit (Nichirei Corporation). The peroxidase reaction was performed using 0.02% 3,3’-diaminobenzidine tetrahydrochloride and 0.01% hydrogen peroxidase in 0.05 M tris-HCl buffer, pH 7.6. Negative control tissue sections were prepared by omitting the primary antibody. CD98 expression was considered to be positive only if plasma membrane staining was presen and it was scored by assessing the extent of staining as follows: score=1, ≤10% of tumor area stained; score=2, 11%-25% stained; score=3, 26%-50% stained; and score=4, ≥51% stained. Tumors with scores ≥2 were defined as CD98 positive. The sections were assessed using light microscopy by at least two authors who were blinded to the results.
Statistical analysis. p-Values of <0.05 indicated statistically significant difference. The significance of difference was determined by Fisher's exact test. The Kaplan–Meier method was used to estimate survival as a function of time and survival differences were analyzed using the log-rank test. Overall survival (OS) was defined as the time from tumor resection to death from any cause. Progression-free survival (PFS) was defined as the time between tumor resection and the initial manifestation of disease progression or death. Multivariate analyses were performed using the stepwise Cox proportional hazards model to identify independent prognostic factors. Statistical analyses were performed using GraphPad Prism 4 (Graph Pad Software, San Diego, CA, USA) and JMP 8 (SAS, Institute Inc., Cary, NC, USA) for Windows.
Results
Patient demographics and immunohistochemical analyses. The immunohistochemical analyses were performed on 331 primary GC lesions. CD98 immunostaining was predominantly localized on the plasma membrane (Figure 1). In our patient cohort, the positive expression rate of CD98 was 19% (66/331). Figure 2 shows the CD98 scoring profiles, in which scores of 1, 2, 3, and 4 were observed in 80%, 12%, 7%, and 1% of GC lesions, respectively. Patient demographics according to CD98 expression status are listed in Table I. CD98 expression was significantly associated with disease stage, T factor, lymph node metastases, non-signet cells, lymphatic permeation, and vascular invasion.
Survival analysis based on CD98 expression. The 5-year OS and PFS rate of all patients was 75% and 74%, respectively. Out of 331 patients, 102 died after the initial surgery. Using univariate analysis, it was found that age, disease stage, T factor, N factor, lymphatic permeation, vascular invasion and CD98 expression had a significant relationship with OS. Meanwhile, disease stage, T factor, N factor, lymphatic permeation and vascular invasion were closely related to unfavorable PFS (Table II). Multivariable analysis confirmed that disease stage, age and T factor were independent prognostic factors for predicting poor OS and that disease stage, T factor and vascular invasion were significant predictive factors for PFS in GC-affected patients. Figures 3A and 3B illustrate the Kaplan–Meier survival curve in patients with high and low CD98 expression, respectively. The prognostic significance of CD98 expression was analyzed according to disease stage and tumor differentiation. No statistically significant difference in OS and PFS was observed between patients with either positive or negative CD98 expression in early (stage I or II) versus advanced stage disease (III or IV). However, the Kaplan–Meier analysis of OS demonstrated a significant difference between patients with either positive or negative CD98 expression and with well or moderate differentiation (Figure 3C), but no such significance was observed in patients with poor differentiation (Figure 3D).

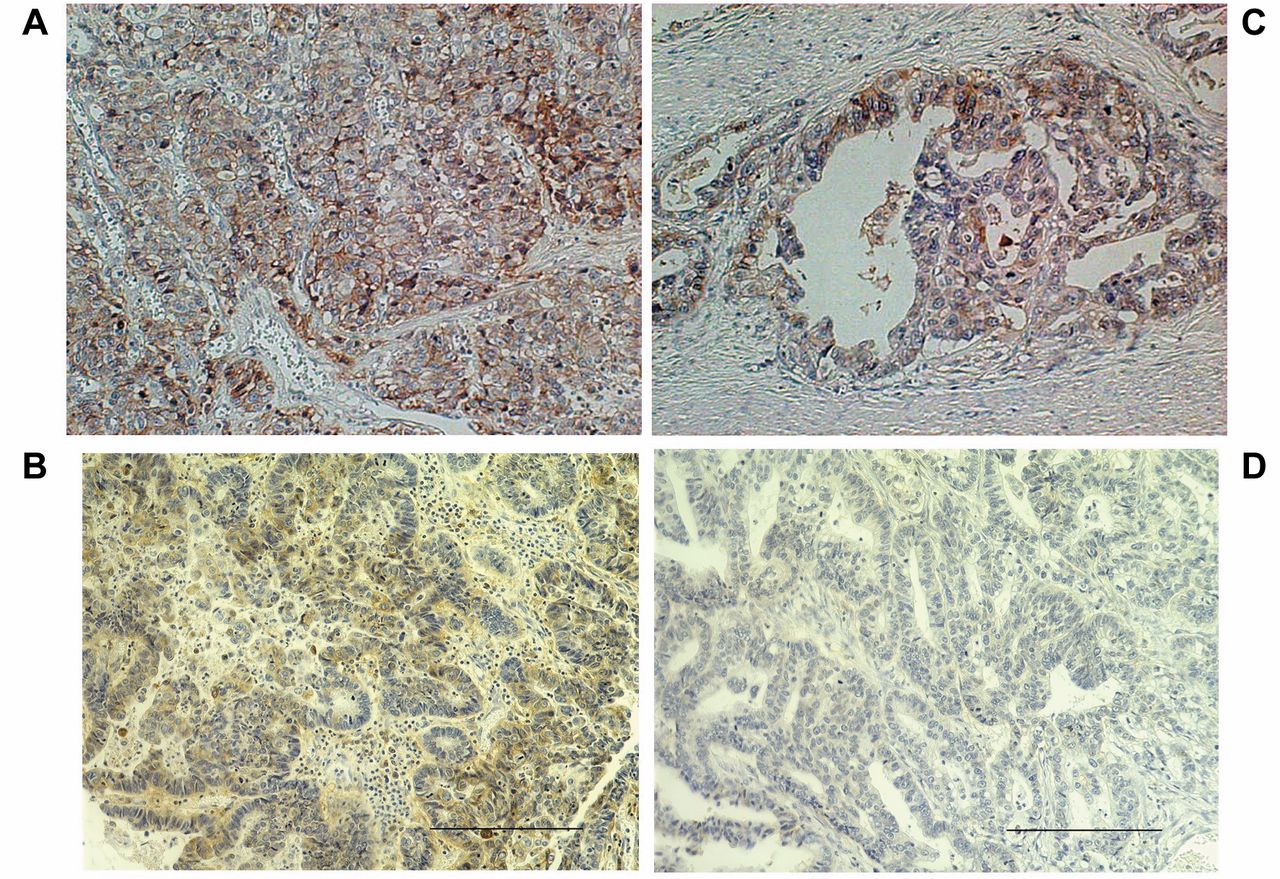
Immunohistochemical staining of CD98 in gastric adenocarcinoma. Positive CD98 staining is localized to the membrane of a malignant melanoma. In the representative images, CD98 immunostaining was scored as grade 4 (A), 3 (B), 2 (C) and grade 1 (D).
Discussion
This study represents the first evaluation of the clinical and pathological significance of CD98 expression in patients with surgically resected GC. We found that increased CD98 expression was significantly associated with tumor aggressiveness and metastasis. CD98 is a potential biomarker that can be used to predict GC patient outcomes after surgical resection. Our study highlighted the prognostic significance of CD98 expression regarding GC-affected patients with well-to-moderate differentiation. These results suggested that CD98 plays a crucial role in tumor progression and GC invasion. Because the mechanism governing such dynamics is unknown, further studies investigating a GC population without poor differentiation is warranted to verify CD98's clinical role in GC. While numerous studies have shown that increased CD98 expression is associated with clinical and pathological features in different cancers, the magnitude of positive CD98 expression (19%) in our GC patient cohort seems to be markedly lower in comparison. The positive rates of CD98 expression in lung, pancreatic, biliary tract, breast, and hypopharyngeal cancers are 47%, 56.7%, 36.7%, 31.8%, and 82.3%, respectively (3-5, 8-10). As mentioned above, CD98 expression levels correlate with LAT1 expression levels (3-5). Our group, has previously noticed that LAT1 expression is higher in patients with squamous cell carcinoma (SQC) than in those with AC (7). Moreover, in patients with lung cancer, LAT1 expression in SQC (with a positive rate of 91%) was significantly higher than in AC (with a positive rate of 29%). The prognostic significance of LAT1 expression has also been shown to be markedly different between patients with SQC and AC. Particularly, LAT1 expression in patients with AC has a direct relationship with worse prognosis, whereas there is a weak association between LAT1 expression and survival in SQC-affected patients. In patients with early stage cancer, LAT1 expression associated more with shorter survival compared to CD98 expression. However, CD98's prognostic role may be more important than that of LAT1 in advanced-stage cancer progression. Additionally, it is uncertain whether the prognostic roles of LAT1 and CD98 are different between patients with early and advanced stages and this warrants rigorous investigation.

Scoring of CD98 expression in GC tumor sections. CD98 scores of 1, 2, 3, and 4 were observed in 80%, 12%, 7%, and 1% of GC tumor sections, respectively.

Survival outcomes after surgical resection. Kaplan–Meier analysis was conducted to assess the impact of CD98 expression on overall survival (OS) and progression-free survival (PFS) in GC-affected patients. A statistically significant difference in OS (A) and PFS (B) was observed between patients with positive or negative CD98 expression. Additionally, Kaplan–Meier analysis of OS resulted in a significant difference between patients with positive or negative CD98 expression and with either well or moderate differentiation (C), but there was no observed significant difference in patients with poor differentiation (D).
Patient's demographics according to CD98 expression.
Univariate and multivariate survival analysis in all patients.
Recently, Toyoda et al. investigated the prognostic significance of LAT1 and CD98 in patients with advanced hypopharyngeal SQC and concluded that CD98 and not LAT1, could serve as a prognostic marker to predict survival outcomes postoperatively, although LAT1 and CD98 were positively expressed at 85.7% and 82.8% of the samples studied, respectively. Additionally, this study exhibited a statistically significant correlation between the expression of LAT1 and CD98. Although CD98's role as a potentially promising and predictive biomarker in advanced human neoplasms (4, 8) is important, there was no significant difference between patients with GC either positive or negative for CD98 expression in terms of advanced stage. Interestingly, our data demonstrated that a significantly worse prognosis was confirmed in GC-affected patients with positive CD98 expression. As stated earlier, Ichinoe et al. noted that LAT1 could be an independent prognostic factor in GC-affected patients without scirrhous carcinoma (13). As scirrhous carcinoma is associated with poor differentiation, LAT1 may be a significant prognostic predictor for GC-affected patients without poor differentiation. Such dynamics are somewhat reflective in our data.
Our study has several limitations. First, we did not investigate the relationship between CD98 expression and the integrin signaling pathway and teasing out this relationship merits future studies. Second, a heterogeneous patient population was evaluated, and such an analysis may bias the results of survival outcomes postoperatively. Next, steps will involve studying survivorship in a homogenous GC patient population. In conclusion, CD98 was positively expressed in 19% of GC-affected patients who underwent surgery and CD98 expression was significantly associated with GC tumor aggression and metastases. CD98 predicted worse prognosis in GC-affected patients, particularly in patients without poor differentiation. However, this result was not confirmed using multivariable analysis. CD98 could be an attractive target for GC therapeutic treatments.
Acknowledgements
The Authors would like to thank Ms. Yuka Matsui for her technical assistance and deeply appreciate Prof. Masahiko Nishiyama of the Department of Molecular Pharmacology and Oncology, Gunma University Graduate School of Medicine for critical reviewing this manuscript. The Authors declare that they have no conflict of interest.
- Received November 10, 2016.
- Revision received January 24, 2017.
- Accepted January 25, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}