


Abstract
Background/Aim: The plasma glutathione peroxidase (GPX1) levels in gallstone patients operated with laparoscopic cholecystectomy (LC) or minicholecystectomy (MC) versus cancer patients is unknown. Patients and Methods: Initially, 114 patients with symptomatic gallstone disease were randomized into LC (n=53) or MC (n=61) groups. Plasma levels of C-reactive protein (hs-CRP) and the oxidative stress marker GPX1 were measured at three time points; before (PRE), immediately after (POP1) and 6 hours after operation (POP2). The end-point of our study was to determine a correlation between the plasma hs-CRP and GPX1 levels in the LC and MC patients versus cancer patients. Results: The plasma GPX1 levels preoperatively and following surgery in the LC and MC patients versus cancer patients were quite similar (p=0.509, p=0.578, p=0.882, respectively). The patients with inflammation of the gallbladder wall (IGW) versus no-IGW had significantly higher plasma GPX median (interquartile range) levels preoperatively (11.5; 6.2-17.4 vs. 8.0; 5.6-14.5, p=0.033) and the GPX values following surgery (POP1, 11.4; 7.8-14.7 versus 7.3; 4.4-11.0, p=0.019 and POP2, 11.5; 7.1-16.2 versus 9.4; 4.2-13.1, p=0.027). The IGW in patients with LC and MC groups combined, correlated significantly to the plasma CRP levels preoperatively (r=0.280, p=0.005) and the CRP values following surgery (POP1, r=0.295, p=0.003 and POP2, r=0.338, p=0.001) and the GPX1 values postoperatively (POP1, r=0.319, p=0.001 and POP2, r=0.243, p=0.026) and to the length of the skin incision (r=0.248, p=0.009). Conclusion: The plasma GPX1 levels preoperatively and following surgery in the LC and MC patients versus cancer patients were quite similar. However, the inflammation of the gallbladder wall (IGW) correlated significantly with plasma GPX1 and hs-CRP values suggesting that inflammation and oxidative stress are related.
Reactive oxygen species (ROS) are a heterogeneous group of highly reactive oxygen containing molecules and have common features closely related to reactive nitrogen species (RNS). The tissues ROS balance is maintained by oxidant producing and oxidant consuming systems. Excessive ROS production or failure in antioxidant defence system may lead to oxidative stress and result in DNA damage and protein and lipid peroxidation (1-3). ROS neutralizing mechanisms can be divided into enzymatic and non-enzymatic antioxidants. The most important enzymatic antioxidants are glutathione peroxidase (GPx), superoxidase, catalase and tioredoxin. The family of GPx consists of 8 isoforms in humans. The active site of all GPx molecules contains a selenocystein and mediates a reaction where glutathione is oxidized and hydrogen peroxidise is reduced.
We have earlier investigated the role of oxidative stress in gastrointestinal operations and concluded that midline laparotomy may cause a reduction in 8-OHdG (4, 5) and GPX1 (6) levels resulting in biochemical evidence of oxidative stress. However, the use of the rectus sheath block analgesia (RSB) in open abdominal procedures does not significantly affect the oxidative stress marker 8-OHdG (5) and GPX1 (6) levels indicating that this stress response is not simply due to surgical trauma. Interestingly, new finding with possible clinical relevance was that the patients with cancer appeared to have a trend for lower plasma GPX1 values than the patients with benign disease (6). To our knowledge, the assessment of plasma GPX1 response in gallstone patients versus cancer patients is unknown and our hypothesis was that there could be some difference in the GPX1 levels and oxidative stress. The primary end-point of the study was, whether the laparoscopic cholecystectomy (LC) or minicholecystectomy (MC) operated gallstone patients have reduced oxidative stress marker GPX1 levels compared to cancer patients.
Patients and Methods
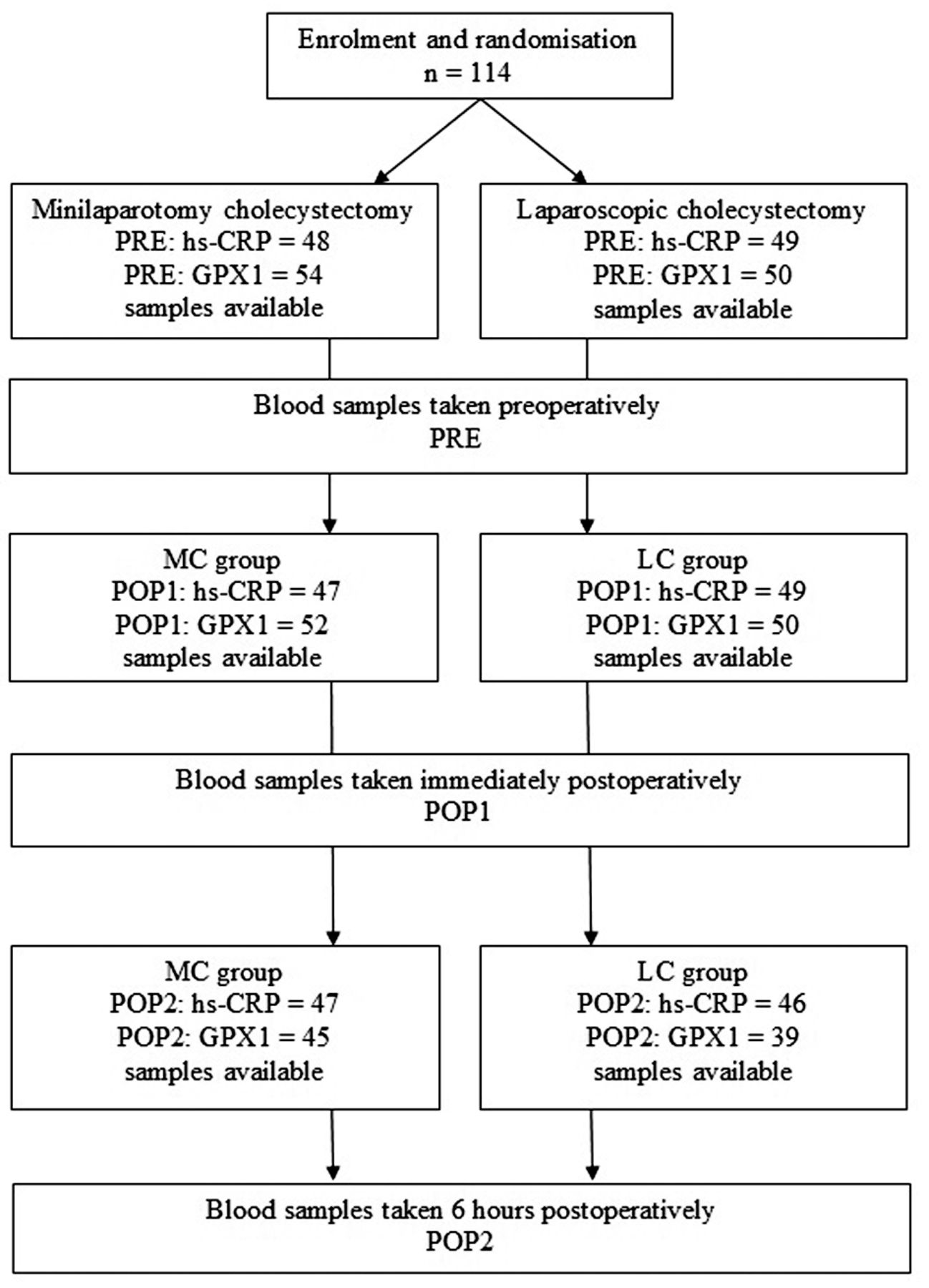
The study was approved by the Ethics Committee of Helsinki and Uusimaa University District, Helsinki, Finland (DNRO 120/13/02/02/2010, May 12, 2010), it was registered in the ClinicalTrials.gov database (ClinicalTrials.gov Identifier: NCT01723540, Consort diagram, Figure 1), and it was conducted in accordance with the Declaration of Helsinki. Design of the study was a prospective, randomized, multicentre clinical trial consisting of 114 patients with confirmed symptomatic cholelithiasis (Table I). Written consent was collected from participants, after they received verbal and written information about the study. Patients were randomized to undergo either laparoscopic cholecystectomy (n=53) or minicholecystectomy (n=61) in two separate hospitals in Finland: Kuopio University Hospital, Kuopio (n=86) and Helsinki University Central Hospital, Helsinki (n=28) between March 2013 and May 2015. Design of the study is presented in Figure 1. After patient enrolment, randomisation was done with a sealed envelope method either to LC or MC groups. The cancer patients, recruited from our previous prospective, randomized trial, included ten patients with gastrointestinal cancer and 19 patients with gynecological cancer (5-7).
The surgical techniques used were standardized in both groups. The LC procedure was performed using the four-trocar technique (two 10-mm and two 5-mm trocars) and intra-abdominal pressure was set at 12 mmHg. The ultrasonic scissors (Harmonic ACE®, Ethicon Endo-Surgery, Cincinnati, OH, USA) were used both in the MC and LC procedure. The gallbladder was dissected from the liver with ultrasonic scissors. The cystic artery was sealed with ultrasonic scissor and two metal clips were inserted to the cystic duct.
The MC technique is a mini-invasive open technique with very short wound; mean (SD) length of skin incision, 4.8 (1.6) cm, and the rectus muscle was not cut, but split. Skin incision length more than 8,0 cm or cutting of rectus muscle resulted in conversion to conventional open operation. Skin incisions were infiltrated with local anesthetic (20 ml ropivacaine 7.5 mg/ml) at the end of the operation. Both study groups were standadized regarding endotracheal anesthesia and postoperative care.
Histopathological analysis was performed to gallbladder specimen; inflammation criteria in this study were visible macroscopic inflammation or thick wall of gallbladder based on surgeon's evaluation and signs of gallbladder inflammation in histopathological analysis. After the final histopathological analysis, the gallbladder specimens were graded to the inflammation of the gallbladder wall (IGW+, n=38) patients or to the IGW- (no inflammation, n=66) patients.
The primary outcome measures were the plasma levels of hs-CRP and GPX1 measured at three time points with high-sensitivity assays: before operation (PRE), immediately after operation (POP1) and 6 hours after operation (POP2). For laboratory measurements EDTA-blood samples were taken at the prespecified time-points and centrifuged at 1000 g for 15 min. Plasma was separated and stored frozen at -70oC until analyzed. Plasma Hs-CRP was analyzed with a Cobas 6000-analyzer (Hitachi, Tokyo, Japan) using the method by Roche Diagnostics (Mannheim, Germany). The plasma GPX1 assays were performed using sandwich-type ELISA methods from BioVendor GPX1 ELISA Kit (62100 Brno, Czech Republic). The limit of detection was 45 ng/l. The intra-assay CV% was 2.7-4.5% and the inter-assay CV% was 4.9-9.0%. The GPX1 assay-protocol is described in our previous paper (6).

Design of the study as flowchart.
The data were entered and analysed with a statistical software program (IBM SPSS Statistics 21.0, IBM, Somers, IL, USA). The biomarker results are presented as median values with interquartile range. The t-test and Mann-Whitney U-test was used for the comparison between the study groups. Group differences in three time points were tested by t-test. The Fisher exact test was used to analyze the frequency data. A two-sided p-value of less than 0.05 was considered statistically significant.
Results
The demographic variables and surgical data were similar in the study groups (Table I). The plasma oxidative stress marker GPX1 levels preoperatively and following surgery in the LC and MC patients versus cancer patients were quite similar (Table II, p=ns). In the LC and MC groups combined, the patients with the IGW+ versus IGW-patients had significantly higher plasma GPX levels preoperatively (Table III, p=0.033) and the GPX levels following surgery (POP1, p=0.019 and POP2, p=0.027, Table III) (Figure 2A). The IGW+ versus IGW-patients had significantly higher plasma hs-CRP levels preoperatively (Table III, p=0.014) and the hs-CRP levels following surgery (POP1, p=0.012 and POP2, p=0.003, Table III) (Figure 2B). There was a significant correlation between IGW+ and plasma hs-CRP levels preoperatively (r=0.280, p=0.005) and the hs-CRP levels following surgery (POP1, r=0.295, p=0.003 and POP2, r=0.338, p=0.001). In addition, there was also a significant correlation between IGW+ and plasma GPX1 values postoperatively (POP1, r=0.319, p=0.001 and POP2, r=0.243, p=0.026). Interestingly, the length of the skin incision in the LC patients correlated significantly with plasma GPX1 levels following surgery (POP1, r=0.483, p=0.001) and with plasma CRP values preoperatively (r=0.524, p<0.001) and following surgery (POP1, r=0.548, p<0.001 and POP2, r=0.553, p<0.001). The length of the skin incision in the LC patients correlated also with BMI over 27.5 (r=0.683, p<0.001). In the LC patients the IGW+ correlated significantly with the length of the skin incision (>56mm) (r=0.350, p=0.013) and with plasma CRP values following surgery (POP1, r=0.290, p=0.043 and POP2, r=0.297, p=0.045). The BMI in the LC patients correlated significantly with the length of the skin incision (r=0.683, p<0.001) and with plasma CRP values preoperatively (r=0.476, p<0.001) and following surgery (POP1, r=0.498, p<0.001 and POP2, r=0.540, p<0.001).
Baseline demographic characteristics and surgical data for the minicholecystectomy (MC) versus laparoscopic cholecystectomy (LC) study groups. Values are mean (standard deviation) or *number of cases.
Changes in plasma levels of hs-CRP and GPX1 measured at three time points; before operation (PRE), immediately after operation (POP1) and 6 hours after operation (POP2) in minicholecystectomy (MC,) and laparoscopic cholecystectomy (LC) patients versus cancer patients. Values are median (interquartile range).
Changes in plasma levels of hs-CRP and GPX1 measured at three time points; before operation (PRE), immediately after operation (POP1) and 6 hours after operation (POP2) in benign cholecystectomy patients with no-inflammation and with inflammation of the gallbladder wall. The marker values are median (interquartile range).

The line charts of the individual preoperative (PRE)- and postoperative (POP1, POP2) glutathione peroxidase (GPX1) (A) and high-sensitivity C-reactive protein (hs-CRP) (B) plasma values for the inflammation (red-colour) and no-inflammation (blue-colour) groups including group medians with bolded lines.
In the MC patients the IGW+ correlated significantly with the plasma CRP levels following surgery (POP2, r=0.373, p=0.008) and to plasma GPX1 values postoperatively (POP1, r=0.315, p=0.023 and POP2, r=0.347, p=0.02).
In patients with the LC and MC groups combined the high BMI correlated significantly with the plasma hs-CRP levels preoperatively (r=0.324, p=0.001) and following surgery (POP1, r=0.354, p<0.001 and POP2, r=0.334, p=0.001) and the plasma GPX1 levels postoperatively (POP1, r=0.202, p=0.04).
Discussion
The main aim of our study was to investigate the plasma GPX1 levels in relation to cholecystectomy technique with special reference to cancer patients and our hypothesis was that there could be some difference in the GPX1 levels and oxidative stress. However, the plasma GPX1 levels preoperatively and following surgery in the LC and MC patients versus cancer patients were quite similar. Interestingly, the inflammation of the gallbladder wall (IGW+) correlated significantly with plasma GPX1 and hs-CRP values suggesting that inflammation and oxidative stress are related.
Several issues should be taken in consideration in oxidative stress research. Baysall et al. (8) recognized DNA damage in operating room personnel and they concluded that DNA damage is depended on oxidative stress response to anesthetics gases. Therefore, to avoid study bias in our trial we have not used anesthetic gasses in our study patients.
Also, several methods and markers have been used in early detection of systemic oxidative stress. Glantzounis et al. (9) assessed the effect of intra-abdominal carbon dioxide pressure on oxidative stress after laparoscopy. The pneumoperitoneum was maintained at 14 mmHg in all patients and plasma levels of thiobarbituric-acid reactive substances (TBARS), TAS and serum uric acid levels were measured preoperatively, 5 minutes after deflation and 24 hours postoperatively. They concluded that increased intra-abdominal carbon dioxide pressure can have a clinically relevant effect on splanchnic circulation. Aran et al. (10) detected in 33 patients with laparoscopy a significant increase in the level of ischemia modified albumin (IMA), which they suggested as possible marker of systemic oxidative stress. However, no statistically significant association between systemic oxidative stress and malondialdehyde (MDA), total oxidant status (TOS), total antioxidant status (TAS) and oxidative stress index (OSI) was found.
Yannikopoulos et al. (11) have reviewed the studies on the effect of laparoscopic surgery on oxidative stress markers. They found four randomized clinical trials (12-15) and four non-randomized studies on elective cholecystectomy (16-19) comparing the plasma levels of lipid peroxidation markers and this systematic review aimed first to investigate the impact of oxidative stress and second the oxidative stress in laparoscopic surgery versus open surgery. There was a great heterogeneity on measured oxidative stress markers, methods and time periods of measurements.
Gal et al. (12) studied the effect of surgical technique on the MDA, myeloperoxidase activity (MPO) and oxidized glutathione (GSH) in 42 consecutive patients with cholelithiasis who received either LC (n=21) or OS (n=21). They found, that the postoperative levels of oxidative stress biomarkers were lower in the LC group compared to the OS group. Ozmen et al. (13) had no significant differences between OS or LC groups regarding nitric oxide NO, MDA or gastric intramucosal pH (pHi). In another randomized study, Zulfikaroglu et al. (14) collected 50 patients with cholelithiasis either to OS (n=25) or LC (n=25) groups. The oxidative stress markers in this study were MDA, NO and the total antioxidant capacity (TAC) using a Trolox equivalent antioxidant capacity method (TEAC). LC patients had a lower TAC score at 24 hours postoperatively than patients in the OS. Bukan et al. (15) found that plasma levels of the NO and MDA were significantly lower in LC (n=21) group compared to OS group in this randomized study.
Olakowski et al. (16) and Seven et al. (17) studied plasma MDA and GPx and found more oxidative stress in OS group. Glantzounis et al. (18) compared plasma MDA and TAC in LC and OS groups and found elevated levels post-operatively in LC group. Stipancic et al. (19) found no significant differences comparing LC and OS groups regarding TAS score in their non-randomized study.
Laparoscopic cholecystectomy (LC) is the gold standard for the treatment of symptomatic gallstone disease, although minicholecystectomy (MC) has shown to have a similar early recovery after surgery (2, 20-29). Our study group (30) has previously reported that the inflammatory response in the LC versus MC patients was quite similar post-surgery, although the LC patients reported significantly lower pain score 24 hours postoperatively and a shorter convalescence than the MC patients in a randomised trial (29, 31). A new finding in our earlier study was a statistically significant correlation between the individual plasma values of the oxidative stress biomarker 8-OHdG versus interleukins IL-10 and IL-1β in the LC and MC patients suggesting that oxidative stress and inflammation are related, which is also supported by recent studies (1, 3). Therefore, we wanted to analyze the plasma levels of hs-CRP, and GPX1 in the LC and MC patients. These results indicated that the oxidative stress response measured by GPX1 plasma levels in the LC versus MC patients was quite similar. Interestingly, a statistically significant correlation between the individual plasma values of the hs-CRP versus GPX1 in the LC and MC patients suggest that inflammation and oxidative stress are associated.
In conclusion, the plasma GPX1 levels preoperatively and following surgery in the LC and MC patients versus cancer patients were quite similar. Interestingly, the inflammation of the gallbladder wall (IGW) correlated significantly with plasma GPX1 and hs-CRP values suggesting that inflammation and oxidative stress are related.
Acknowledgements
The study was funded by the Heikki, Aino and Aarne Korhonen foundation and the EVO-funding of the Helsinki and Kuopio University Hospital, Finland.
Footnotes
Conflicts of Interest
The Authors report no conflicts of interest or financial ties to disclose. The authors alone are responsible for the content and writing of this article.
- Received September 12, 2017.
- Revision received October 3, 2017.
- Accepted October 5, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Plasma Concentration of the Lipid Peroxidation (LP) Biomarker 4-Hydroxynonenal (4-HNE) in Benign and Cancer Patients
- The Induction of Antioxidant Catalase Enzyme With Decrease of Plasma Malonidialdehyde: An Important Reactive Oxidative Species Inhibiting Mechanism
- Nitrotyrosine (NT), a Nitrosative Stress Biomarker, Plasma Concentrations in Gallstone Disease and Cancer Patients
- Cholecystectomy Patients with High Plasma Level of Catalase Have Significantly Lower Analgesia Requirement: A Prospective Study of Two Different Cholecystectomy Techniques with Special Reference to Patients with Cancer
- Gallstone Patients with Enhanced Oxidative Stress Biomarker Superoxide Dismutase (SOD1) Plasma Levels Have Significantly Lower Number of Postoperative Analgesic Oxycodone Doses: A Prospective Study with Special Reference to Cancer Patients
- Patients with Increased Levels of the Oxidative Stress Biomarker SOD1 Appear to Have Diminished Postoperative Pain After Midline Laparotomy: A Randomised Trial with Special Reference to Postoperative Pain Score (NRS)