


Abstract
Aim: To evaluate the prognostic significance and potential therapeutic implication of genetic variability in prostaglandin E2 pathway genes in patients with locally advanced rectal cancer (LARC) treated with neoadjuvant chemoradiotherapy (nCRT) followed by surgery. Materials and Methods: This cohort study included 167 patients with LARC, treated with nCRT followed by surgery. A total of 61 single nucleotide polymorphisms (SNPs) were characterized using the Sequenom platform through multiplex amplification followed by mass-spectometric product separation. Surgical specimens were classified according to Mandard tumor regression grade (TRG). The patients were divided as ‘good responders’ (Mandard TGR1-2) and ‘poor responders’ (Mandard TRG3-5). We examined prognostic value of polymorphisms studied to determine if they are related to Mandard response. Results: Mandard tumor response and rs17268122 in ATP binding cassette subfamily C member (ABCC4) gene were the only two parameters with independent prognostic significance for disease-free survival. Conclusion: tagSNP ABCC4 rs17268122 appears to be a prognostic factor in LARC treated with nCRT and surgery, independently of response to nCRT. The screening of ABCC4 rs17268122 tagSNP and the Mandard tumor response in clinical practice may help to identify patients with different rectal cancer prognosis and contribute to an individualized therapeutic decision tree.
- Molecular marker
- prostaglandin E2 pathway genes
- neoadjuvant chemoradiation
- polymorphism
- survival
- rectal cancer
- Mandard response
Neoadjuvant chemoradiation followed by curative surgery remains the standard care for locally advanced rectal cancer. It improves local control and reduces toxicity compared to postoperative treatment (1). However, not all patients benefit from this type of protocol. About one-third of patients still develop distant metastases and eventually die of their disease (2). Tumor down-sizing and down-staging, with locoregional disease control and better survival, is achieved only if there is complete or near-complete tumor response (3, 4). In fact, various histopathological responses to the same chemoradiotherapy protocol are possible and are related more to tumor biology than tumor stage. Understanding tumor biological features and patient genetic variability are important; only this through can a more patient-tailored treatment capable of conferring better prognosis become possible. One of the aspects that can affect tumor biology and explain different behavior of rectal cancer is that of genetic biomarkers. These can be studied through immunohistochemical expression in tumor biopsies and tumor-resected specimens, or by genetic variability analysis using patients' blood or tumor tissue samples.
Over the past decade, the study of the genetic background, namely single nucleotide polymorphisms (SNPs), has raised growing interest. These are the simplest type of polymorphism and result from a single base mutation, which substitutes one nucleotide by another. In fact, since SNPs are inherited from one generation to the next, with high frequency in the genome and with potential functional repercussions in gene expression, they represent good biomarkers of tumor biology (5). The study of cyclooxygenase-2 (COX2)-derived prostaglandin E2 (PGE2) pathway genes in LARC treated with neoadjuvant chemoradiotherapy (nCRT) and surgery may help to understand the different tumor behavior and response heterogeneity in patients with the same clinical stage treated with similar schemes. In fact, COX2-derived PGE2 is the most abundant prostaglandin found in colorectal tumors (6, 7). In addition to its well-known role in inflammatory reactions, COX2 plays a role in tumor progression, stimulation of angiogenesis, promotion of metastasis, and decrease of the antitumor immune response (8, 9). Steady-state extracellular PGE2 levels are regulated by the balance between biosynthesis and degradation, promoted by 15-hydroxyprostaglandin dehydrogenase (HPGD) but also the specific influx and efflux PG membrane transporters [prostaglandin transporter (PGT) encoded by SLCO2A1 gene and multidrug resistance-associated protein 4 encoded by ABCC4 gene]. Hence genetic variability in COX2, HPGD, SLCO2A1 and ABCC4 PGE2 pathway genes can influence gene expression, leading to the extracellular accumulation of PGE2, development, progression of colorectal cancer, or even interfering with chemoradiation response and prognosis in locally advanced rectal cancer (LARC) (10-13).
Therefore, with this study we aimed to evaluate 61 SNPs, the majority in PGE2 pathway genes, on survival of patients with LARC cancer treated with nCRT followed by surgery at a single tertiary center.
Patients and Methods
Ethics approval. This project was approved by the Research Ethics Health Committee (references188-CES) and Department of Education, Development and Research (reference 133-DEFI) of the Hospital Center of Porto. Informed consent from patients whose tissue was archived was not required as per Ethics Board guidelines. Patient informed consent for the use of blood and tissue for genetic polymorphism was obtained.
Patient population. A consecutive series of patients with, biopsy-proven LARC, who underwent nCRT followed by elective radical surgery with total mesorectal excision (TME) with curative intent between January and December 2013 were recruited after reviewing the clinical database at the Digestive Surgery Service, of University Hospital Center of Porto, which is a tertiary referral center for a population of 728,663 inhabitants. All patients with rectal cancer (T2N+M0 or cT3/4 N0/+M0) located at less than 12 cm of distance from the anal verge who received nCRT and were operated within 8 weeks after radiotherapy ended were included, if none of the following exclusion criteria were met: other diagnosed neoplasia, short course radiotherapy, post neoadjuvant stage IV, R1/R2 surgery, and postoperative death within 60 days.
Diagnosis and staging criteria. Staging included rigid proctoscopy, total colonoscopy, chest, abdominal and pelvic computed tomographic scan, endorectal ultrasound, pelvic magnetic resonance image (since 2008), and serum carcinoembryonic antigen (CEA) level.
nCRT protocol. This protocol included total irradiation of 50.4 Gy in 28 fractions and 5-fluorouracil (5-FU) by infusion pump (225 mg/m2/day, 7 days for week, from the first until the last day of radiotherapy) or capecitabine (2500 mg/m2/day, divided in two doses, from de first until the last day of radiotherapy). All patients receiving nCRT were operated on within 8 weeks after radiotherapy ended.
Surgical procedures. Radical surgery consisted mainly of sphincter_saving rectal resection or abdominoperineal resection both with total mesorectal excision. Regarding the selection of the operative procedure, we considered the distance of the lesion from the anus, the comorbidities of the patient, and the condition of the anal sphincter.
Adjuvant chemotherapy protocol. Post surgery, patients were administered adjuvant chemotherapy protocol for 6 months performed preferably with 5-FU or a combination of 5-FU and oxaliplatinum (one of the followed regimens: mFolFOX6 – 200 mg/m2 folinic acid (FA) day 1, 400 mg/m2 5-FU bolus day 1, continued infusion for 46 hours of 2,400 mg/m2 5-FU and 85 mg/m2 oxaliplatin, 14/14 day cycle; CapeOx: 1,000 mg/m2 capecitabine twice a day, days 1-14, 130 mg/m2 oxaliplatin day 1, 21/21 day cycle; 5-FU/FA: 200 mg/m2 FA day 1, 400 mg/m2 5-FU bolus day 1, continued infusion for 46 hours of 2,400 mg/m2 5-FU, 14/14 day cycle).
Systemic inflammatory markers. Blood samples from all patients were collected within 7 days before starting nCRT protocol. White blood cell, neutrophil, lymphocyte, and platelet counts were recorded. The neutrophil to lymphocyte ratio (NLR) was calculated as the neutrophil count divided by the lymphocyte count using preoperative blood test results. An NLR ≥3 was considered elevated (based on receiver operating characteristic curve analysis).
Pretreatment biopsy samples – hematoxylin and eosin (H&E) staining and immunohistochemistry (IHC). Diagnostic pretreatment paraffin-embedded biopsies were available and reviewed by a pathologist blinded to clinical data. Tumor biopsy sample classification, including grade, were obtained for the worst tumor areas whenever available material contained several areas with neoplasia. The mitotic index was the number of mitoses for 10 high-powered fields and the cut-off was chosen taking into account the best ratio of sensitivity to specificity. In the absence of neoplasia in 10 high-power fields, the number of mitoses was counted in the number of observed fields, estimating the value for 10 fields.
IHC for cyclin D1, p21, epidermal growth factor receptor (EGFR) and vascular endothelial growth factor (VEGF) were performed in tissue arrays constructed from core tissue specimens (preoperative endoscopic biopsy) taken before treatment. Representative core tissue specimens (2 mm in diameter) were taken from individual paraffin blocks and rearranged in new tissue array blocks using a trephine apparatus (Superbiochips Laboratories, Seoul, Korea). Array slides were labeled by IHC with four commercially available antibodies to: cyclin D1 (1:1,000; BD Biosciences, MA, USA), p21 (1:300; Spring Bioscience, CA, USA), EGFR (1:200; Abcam, MA, USA), and VEGF (1:30 dilution; BD Biosciences). Antigen retrieval was performed by immersing the slides in citrate buffer (pH 6.0) and microwaving them for 10 min. Non-reactive sites were blocked using 1% horse serum in Tris-buffered saline (pH 6.0) for 3 minutes. Primary antibodies were applied, and antibody binding was detected using the avidin-biotin peroxidase complex (Universal Elite ABC kit PK-6200; Vectastain, Burlingame, CA, USA) and diaminobenzidine tetrahydrochloride solution (Kit HK 153-5 K; Biogenex, San Ramon, CA, USA). We performed the IHC procedure without primary antibody for negative controls. Normal colorectal epithelial cells were used as internal negative controls.
The location of staining, nuclear, membranous, or cytoplasmic, was recorded.
The percentage of positively stained cells were assigned to one of four categories for protein expression: 0%, 0; 1-25%, 1; 26-50%, 2; >50%, 3. The staining intensity was scored as follows: none or weak, 0; moderate, 1; intense, 2. If the staining intensity was heterogeneous in a section, it was scored based on that which was predominantly observed. The two scores (if different from zero) were then multiplied to produce a weighted score for each tumor specimen. The final score was grouped as follow 0-3, weak; ≥4, strong (Figure 1).
Sample collection and biological processing for DNA analysis. DNA was extracted preferably from blood or alternatively from tumor tissue. Blood samples were collected with a standard venipuncture technique using EDTA-containing tubes before the beginning of neoadjuvant therapeutic. Genomic DNA was extracted from peripheral blood leukocytes, using the QIAamp DNA Blood Mini Kit (Qiagen, Madrid, Spain) following the manufacturer's instructions.
For patients unable to provide a blood sample, the DNA was extracted from formalin-fixed paraffin-embedded blocks from the Pathology Department at our Hospital. Two to four 10-mm thick section were used in each extraction depending on the size of tissue area (1.5-3 cm2). Briefly, the tumor tissue specimens from each glass slide were scraped, using a clean razor blade, into a 1.5-ml microcentrifuge tube followed by centrifugation at 14,000-16,000 × g for 3 minutes. The tissue pellets were then rehydrated with 1 ml of absolute ethanol, followed by centrifugation at 14,000-16,000 × g for 3 minutes and the supernatant was discarded. This step was repeated twice. The tube was left open for 15 min to allow any remaining ethanol to evaporate. Further steps of DNA isolation were performed using the GRS Genomic DNA Kit. Tissue, in accordance with the manufacturer's protocol (GRiSP, Porto, Portugal).
DNA was quantified using a NanoDrop 1000 Spectrophotometer (Thermo Fisher Scientific, Wilmington, DE, USA) and stored at −20°C until genotype examination. The DNA quality was determined by measuring the optical density (OD) 260/280 ratio.
Polymorphism selection. The strategy for polymorphism selection has been described elsewhere (10). Briefly, using a tagSNP approach, the genetic variants were retrieved from a set of common SNPs in the Caucasian population of HapMap project (CEU) (https://ncbi.nlm.nih.gov). The Genome Variation Server (version 7.00) was used to recover tagSNPs capturing variations (i) with a minor allelic frequency of 15% or more; (ii) within the coding region of the genes plus 2 kb upstream and downstream, (iii) with a r2 greater than 0.8, and (iv) which successfully converted to the Sequenom platform (Sequenom, San Diego, CA, USA). A total of 55 tagSNPs were analyzed in COX2, HPGD, SLCO2A1 and ABCC4 PGE2 pathway-related genes.
Furthermore, rs2946834 insulin-like growth factor 1 (IGF1), rs1801280 N-acetyltransferase 2 (NAT2), rs1800629 tumor necrosis factor–alpha (TNFA), rs9344 cyclin D1 (CCND1), rs2227983 EGFR, and rs1800871 interleukin 10 (IL10) polymorphisms, previously found to be associated with colorectal tumor development, were also included.
Genotype characterization. TagSNP genotyping was performed using MassARRAY iPLEX Gold technology (Sequenom) based on multiplexed amplification followed by mass-spectrometric product separation. This technique was carried-out by the Genomic Unit, Genotyping Service, Gulbenkien Science Institute.
Resected specimen samples – H&E staining and IHC. Immunohistochemical staining for cyclin D1, p21, EGFR and VEGF were performed in tissue arrays constructed from core tissue specimens taken from the resected specimen using the methodology applied in pretreatment tumor biopsies.
Standard pathological tumor staging of the resected specimen was performed in accordance with the guidelines of the American Joint Committee on Cancer (http://www.cancerstaging.net). The circumferential resection margin was scored as positive when cancer cells were within 1 mm of the margin. Evidence of pathologic complete response after neoadjuvant treatment (ypCR) was defined as an absence of viable adenocarcinoma in the surgical specimen or the presence of lakes of mucus without tumor cells. The histology of all surgical specimens was reviewed and confirmed by a pathologist blinded to clinical data and were classified based on the Mandard tumor regression grading system (14).
The number of tumor samples taken from the resected specimens was variable, with a mean of six paraffin blocks per case. The methodology used was the following. Five samples were taken from the area with macroscopic lesion (assuming it existed), i.e. in the same manner as dealing with a specimen from a patient who had not received neoadjuvant therapy. These included the closest macroscopic approach of the macroscopic lesion to the peritoneal surface or the mesorectal excision plane, as appropriate. If no viable tumor was identified within the initial five blocks, the whole of the remainder of any macroscopic lesion in additional blocks was included. If no viable tumor was identified within these extra blocks, another three further levels from all of these blocks were taken. If no viable tumor was identified in these sections, then complete histological tumor regression was assumed.
All obtained slides were seen and reviewed by the same experienced pathologist blinded to clinicopathological data. Items observed and registered in the biopsies were subsequently analyzed in the resected specimen and the same criteria adopted.
Patients were then divided in two groups according to the Mandard TRG system, good responders were defined as Mandard TRG1 orTRG2; poor responders were defined as Mandard TRG3, TRG4 or TRG5 (Figure 2). Both groups (good vs. poor responders) were used to evaluate outcomes.
Survival and disease recurrence definitions. Disease recurrence was evaluated according to location: locoregional (LR), systemic (DR), or mixed. All surviving patients were followed-up and their current status was confirmed. None of the patients were lost from follow-up. Disease-free survival (DFS) was calculated from the first date of neoadjuvant treatment to the date of progression (local or distant).
Statistical analysis. The survival function was estimated using the Kaplan–Meier method. The difference in survival rates between groups was tested for significance using the log-rank test. A Cox proportional hazard regression model was performed to estimate which prognostic factors were associated with survival: age; gender clinical stage; anal-to-tumor distance; pre-treatment CEA; pre-treatment NLR; biopsy mitotic number; inflammatory infiltrate; pre-treatment IHC expression of cyclin D1, EGFR, VEGF and p21; CEA post-CRT; surgery procedure; tumor grade; tumor desmoplastic infiltration; tumor inflammatory reaction; tumor vascular venous invasion; tumor lymphatic invasion; tumor perineural invasion; pathologic stage; circumferential involvement; tumor mitosis number; tumor necrosis; post-treatment immunohistochemical expression of cyclin D1, EGFR, VEGF and p21; tumor downstaging and downgrading; Mandard TRG response; and status of 61 tagSNPs. Univariate analysis studied survival with respect to the parameter under investigation. Multivariate Cox stepwise likelihood ratio analysis selected prognostic factors after adjustment for the effect of the other variables and a Cox model using enter method was applied. The significance of differences in proportions was calculated with Chi-square test and the differences in means with Student's t-test. The statistical analysis was performed using SPSS statistical software (version 21.0 for Windows; IBM Corp., Armonk, NY, USA). All statistical tests were conducted at a two-sided level of significance of 0.05 and factors significant with p<0.15 were included in the multivariate analysis.
Results
Description of study population and clinical parameters. This cohort study gathered 186 consecutive patients with LARC treated with nCRT follow by curative surgery with total mesorectal excision at one single University Hospital. After exclusion of 11 patients with positive radial margin (R1 surgery), for 4 patients with yp stage IV, and four deaths within 60 postoperative days, 167 patients were included in the present analysis, with a median age of 64.8 years (range=31-82 years). The male to female ratio was 1.69:1. The clinical parameters are summarized in Table I.
Polymorphism study. Three SNPs were excluded from the analysis due to genotyping failure, leaving a total of 58 to be included in the survival analysis: 29 in ABCC4, 15 in SLCO2A1, seven in HPGD, and one each in COX2, EGFR, CCND1, IL10, TNFA, IGF1 and NAT2 genes. Genotypic frequencies and DFS by selected SNPs in the 167 patients are given in Table S1 (http://chporto.pt/Table-S1a).
Biopsy characteristics. The biopsy characteristics including IHC expression of cyclin D1, p21, EGFR and VEGF are shown in Table II.
Clinical parameters of patients included in this study.
Surgery. Sphincter-saving rectal resection with anastomosis (with or without protective ileostomy) was performed on 107 patients (64.1%). Abdominoperineal resection was performed on 53 patients, and seven patients were subjected to proctectomy with definitive stoma. The perioperative morbidity of the series was 25.1%, with 16 abdominal or pelvic abscesses, three anastomostic leaks, that included six reoperations (due to three leakages and three abdominal abcesses), and three re-admissions (due to pelvic abscess).
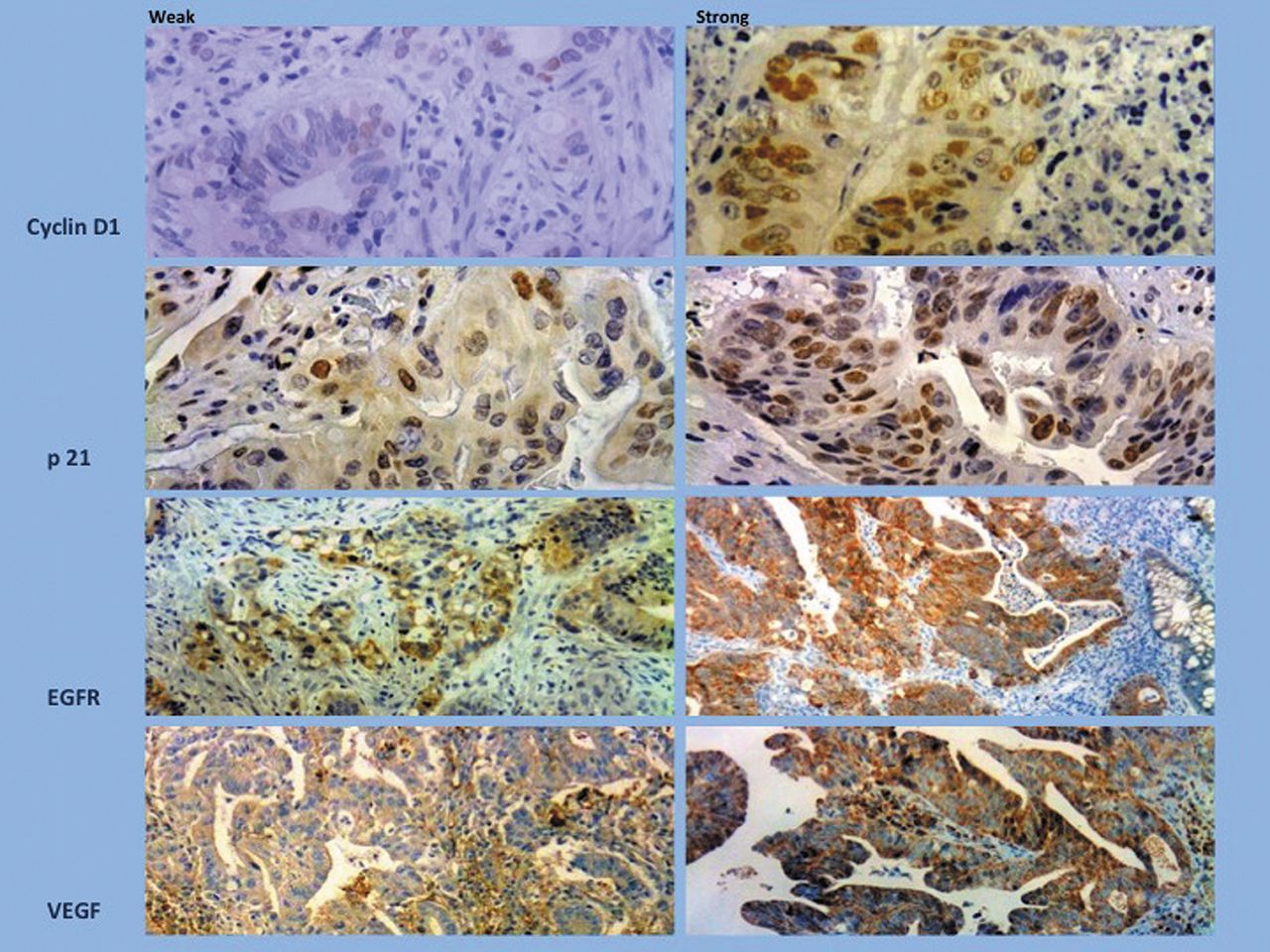
Immunohistochemical study of cyclin D1, p21, epidermal growth factor receptor (EGFR) and vascular endothelial growth factor (VEGF) showing representative examples of weak and strong staining (×200 and ×100).

Mandard tumor regression grade (TRG) system and representative examples of TRG for resected adenocarcinoma.
Pathology of resected specimens. Stage distribution is shown in Table III.
The average number of dissected lymph nodes in the surgical specimens was 8 (range=0-22). Circumferential resection margin >1 mm was confirmed in all 167 patients.
Response to neoadjuvant therapy is characterized in Table III. Tumor downstaging was observed in 67 patients (40.1%). Reduction in T-stage by one level was observed in 29 patients (17.4%) and by two or more levels in 38 patients (22.8%). Observations indicating pathological down-staging are given in Table III. Ninety-five (56.8%) patients presented one or lower pathological stage than their initial clinical tumor stage. ypCR or Mandard TRG1 was confirmed in 31 patients (18.5%). The use of Mandard system allowed us to define two groups as previously mentioned: good responders (Mandard TRG1-2) and poor responders (Mandard TRG3-5). Using the Mandard system, a good response to nCRT was found in 86 patients (51.4%) and a poor response in 81 (48.5%).
Clinical outcome. Table IV shows long-term clinical outcome, relapse of disease and survival. With a median follow-up of 64 months (range=6-148 months), 5-year DFS was 73.3% and pelvic control was 95.8%. Seven patients (4.2%) developed pelvic recurrence (five isolated and two with synchronous metastatic disease) and 22 (13.2%) distant metastases alone. Two out of seven pelvic recurrences occurred later in the outcome – after 18 months of follow-up (at 28 and 45 months, respectively). Twelve out of 167 patients had more than 24 but less than 42 months of follow-up. Local recurrence increased slightly to 4.5% (7/155) when considering only patients with more than 42 months of follow-up.
Prognostic value of data variables. More than 90 variables were included in the univariate analysis for prognostic significance (including morbidity). Thirteen were associated with an adverse prognosis and subsequently included in the multivariate model (p<0.15), as shown in Table V.
Patients with a poor Mandard response, ypN stage 1-2, with no pathological TNM downstaging, with moderately differentiated or undifferentiated tumors, presenting overexpression of VEGF or p21 in pretreatment biopsies, or who were carriers of rs17268122TT and rs8002180TT/TC in ABCC4, rs1800871AA in IL10 or rs2227983GG in EGFR genotypes presented a significantly worse 5-year DFS.
In a univariate analysis, four tag SNPs were identified as biomarkers associated with DFS: rs17268122 and rs8002180 in ABCC4, rs2227983 in EGFR, and rs1800871 in IL10. One of them, rs17268122 in ABCC4 gene.
Biopsy characteristics.
In a Cox stepwise forward likelihood model, the Mandard TRG response and ABCC4 rs17268122 tagSNP were identified has independent prognostic factors after adjustment considering all other variables (Table VI). Patients with ABCC4 rs17268122GG and a poor Mandard response had a nearly three-fold increased likelihood of death (p=0.002) compared with those with this genotype with a good response. Furthermore, patients homozygous for the rs17268122TT ABCC4 genotype exhibited a worse DFS (p=0.001).
Characteristics of resected specimens.
We also calculated the HR by Mandard response for the three genotypes of rs172268122 ABCC4 (GG, GT and TT). Patients with a poor response to nCRT with GG genotype of the rs17268122 ABCC4 had a HR=2.916 (95% CI=1.370-5.426); patients with a poor response to nCRT and GT genotype of rs17268122 ABCC4 had an increased likelihood of death with HR=4.627 (HR=e1.070+0.406; 95% CI=1.174-18.653) and those with a poor response with TT genotype had a very dismal HR of 13.653 (HR=e1.070+1.544; 95% CI=1.582-68.191).
Figures 3 and 4 show Kaplan–Meier survival curves for DFS according to Mandard response and rs17286122 ABCC4 genotype.
Discussion
The use of nCRT in LARC modified the prognostic value of traditional clinical parameters. In fact, when nCRT is employed, the magnitude of tumor response has greater impact on survival than the majority of pre-treatment tumor features, including clinical stage (15, 16). The prognostic factors are commonly parameters resulting from nCRT action on tumor tissues that lead to changes in tumor size and also in characteristics of tumor cells and surrounding tissue. These alterations are reflected in histological features, such as tumor differentiation, mitotic number, amount of necrosis, mucin deposits, fibrotic grade, desmoplastic reaction, type and amount of inflammatory cells, and in IHC results. The assessment of tumor response can be performed on single or a set of histopathological tumor characteristics using ypTNM classification and TRG scales. These are aspects of tumor response assessment widely being studied by us (17) and by many other groups, with different prognostic impact (3, 4, 15, 16, 18-26). These heterogeneous results can be explained by several aspects instudy design such as: adoption of different tumor regression grade scales, lack of method standardization, semiquantitative methods and the utilization of different antibodies and reagents in IHC studies. With SNP characterization, part of this problem is overcome. The results of genetic analysis remain immutable not depending on whether DNA extraction was performed from tissue or blood, before or after nCRT. The greatest drawback concerns SNP selection, procedural costs and difficulty of application in clinical practice.
Long-term clinical outcome, relapse of disease and disease-free survival (DFS).
Despite these technical difficulties, our project included analysis at three main levels: IHC, histological and genetic.
For IHC analysis of pretreatment biopsies and resected specimens, we categorized samples by weak and strong expression to reduce interobserver variability. Four molecular markers were selected: cyclin D1, which plays a vital role in cancer cell-cycle progression and for which overexpression might be associated with poor clinical outcome (27); EGFR, a transmembrane tyrosine kinase receptor that can activate a cascade of multiple signaling pathways that facilitate tumor growth and when overexpressed can be related to more aggressive disease (24); VEGF, associated with angiogenesis stimulation and when overexpressed is associated with tumor growth and aggressiveness (28); and p21, a cell-cycle inhibitor, which when overexpressed may be associated with chemotherapy resistance (29). In this study, only weak expression of VEGF and p21 in pre-treatment biopsies was found to confer better prognosis than strong expression, although without statistical significance in the multivariate analysis. This result is concordant with those of Bertolini et al. (29). Nevertheless, the role of p21 expression as a prognostic factor in survival in rectal cancer remains controversial (30-32).
Association of factors with 5-year disease-free survival (DFS).
Concerning assessment of histological tumor response to CRT, we decided to adopt a two-point classification system based on Mandard TRG to split the patients into subgroups with significantly different prognosis, according to previous studies (33, 34). This methodology allows us to find prognosis factors with significance in multivariate analysis. In our study, these parameters had a stronger impact on outcome than other pathological features also related to tumor response to CRT such as CMR distance, ypT stage, ypN stage, yp tumor differentiation grade, tumor downstaging and pathological TNM downstaging. Once again, our results concur with these of some centers (4, 18, 35) but for others complete pathological response or yp nodal stage, for example, have a leading role in survival (16, 19, 22, 36).

Disease-free survival according to Mandard response. Good response: Tumor regression grade (TRG)1-2, poor response: TRG3-5.

Disease-free survival according to rs12268122 ATP binding cassette subfamily C member (ABCC4) genotype.
Cox model for disease-free survival.
The SNP selection was based on preliminary results of the study published by Pereira et al. (10) and also on the concept of inflammation and oxidative stress as a key role in development and progression of colorectal cancer (37, 38). The methodology used allowed us to identify some parameters with potential survival influence. In a univariate analysis, four tag SNPs were identified as biomarkers associated with DFS: rs17268122 and rs8002180 in ABCC4, rs2227983 in EGFR, and rs1800871 in IL10. One of them, rs17268122 in ABCC4 gene, maintained prognostic significance in multivariate analysis. Poor responders with ABCC4 rs17268122GG, -GT or -TT genotype had almost 3-, 5- and 14-fold increased hazard of death, respectively, compared with patients with a good response and GG genotype.
To our knowledge, this is the first study published about the potential influence of SNP variability in PGE2 pathway genes on survival of patients with LARC treated with nCRT followed by surgery and adjuvant chemotherapy. Although our findings must be confirmed in a large multicenter study with identical design, it seems the application of a standard TRG scale and the assessment of ABCC4 rs17286122 gene variability in patients with LARC will be of benefit in clinical practice.
Conclusion
In our study, the two main factors with independent prognostic significance in DFS in patients with LARC treated with nCRT followed by surgery were Mandard tumor response and the rs17268122 variability in ABCC4 gene.
The characterization of genetic variability in PGE2 pathway-related genes seems to be important in patients with LARC. Application of Mandard tumor response appraisal and ABCC4 rs17268122 genotype in a DFS model in clinical practice may help to identify patients with rectal cancer with different prognosis and contribute to an individualized therapeutic decision tree.
Acknowledgements
The Authors are thankful to Santo António Hospital Surgery Department Support Association and Department of Education, Development and Research of Hospital Center of Porto for funding. The Authors would like to acknowledge technical assistance from Arnaud Cruz Paula, Paulo Brochado, Hildeberto Moreira and Berta Silva Martins in tissue microarray construction, slides immunohistochemistry staining and blood/tissue DNA extraction.
Footnotes
Availability of Data and Materials
This was an observational cohort research study with a prospective registration. The data and materials are available from the Surgery Department of Hospital Center of Portos, Portugal.
Funding
This study was supported by a research grant from the Santo António Hospital Surgery Department Support Association and from Department of Education, Development and Research of Oporto Hospital Center. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.
Disclosure
All Authors state that they have no conflicts of interest in regard to this study
- Received October 25, 2016.
- Revision received November 27, 2016.
- Accepted December 1, 2016.
- Copyright© 2017 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.