


Abstract
Background: A recent clinical trial on the immune check-point inhibitor pembrolizumab demonstrated that microsatellite instability (MSI) is a good biomarker for response to this inhibitor. However, clinicopathological features of advanced colorectal cancer (CRC) with high-frequency MSI (MSI-H) are unclear. Patients and Methods: A total of 2,439 surgically resected CRC tissues were analyzed for MSI status, and mutational status of V-Ki-Ras2 Kirsten rat sarcoma 2 viral oncogene homolog (KRAS), neuroblastoma RAS viral oncogene homolog (NRAS) and v-Raf murine sarcoma viral oncogene homolog B (BRAF). Stage IV cases were selected, and clinical and molecular features were evaluated. Results: There was no significant survival difference observed between MSI-H CRC and microsatellite-stable (MSS) CRC in patients with stage IV disease (3.92 vs. 2.50 years; p=0.766). However, hematogenous and lymphogenous metastasis-dominant CRC with MSI-H demonstrated poor prognosis, whereas peritoneal metastasis-dominant CRC with MSI-H demonstrated good prognosis, (1.33 vs. 5.2 years; p=0.006). Conclusion: Prognosis of stage IV CRC with MSI-H depended on the metastatic pattern. These findings provide useful information for the adaptation of CRC immunotherapy.
Colorectal cancer (CRC) is the third most commonly diagnosed cancer and frequent cause of cancer-related death worldwide (1). Specifically, the 5-year survival rate of patients with advanced CRC is less than 30%, and further advances in chemotherapy and surgical techniques are required to improve the survival rate of patients with CRC. Recently, novel molecular-targeting drugs, such as antibody to epidermal growth factor receptor (EGFR), are based on the molecular mechanism of carcinogenesis and achieve good efficacy. However, biomarkers are often required for appropriate therapy and are predicted based on the molecular mechanism of carcinogenesis.
During carcinogenesis, genetic changes, including deletion, insertion and substitution of nucleotides, rearrangement and epigenetic changes are accumulated. At least two types of genetic changes are known: chromosomal instability (CIN) and microsatellite instability (MSI). CIN comprises of structural and numerical changes of chromosomes, whereas MSI comprises frequent mutations in the microsatellite area without obvious structural and numerical changes of chromosomes. It has been reported that in Western countries approximately 80% of CRCs exhibit CIN and 15% have MSI (2). MSI is caused by dysfunction of the mismatch repair system, which detects and repairs mismatches that occur during DNA replication (3, 4). CRCs with CIN and MSI demonstrate different clinicopathological features, probably because of different mechanisms of genetic changes (5).
Sporadic CRC with high-frequency MSI (MSI-H) is prone to develop in the proximal colon and in older females. Pathological characteristics are associated with the presence of tumour-infiltrating lymphocytes, a Crohn's-like lymphocytic reaction and mucinous/signet ring cell differentiation (6-9). Although CRC with MSI-H is indicative of good prognosis in stage II and III disease (10-12), several reports suggest that the prognosis of CRC with MSI-H is poorer than that of microsatellite-stable (MSS) CRC in stage IV (13, 14), and is still unclear whether this is correct or not.
In a recent study, the immune checkpoint inhibitor pembrolizumab significantly prolonged the disease-free and overall survival (OS) rates for CRC with MSI-H compared to those for CRC with MSS (15). Therefore, immune checkpoint inhibitors are highly expected to be an effective treatment for CRC with MSI-H. In this study, we evaluated the clinicopathological and molecular characteristics of stage IV CRC with MSI-H which may become potential targets of immune checkpoint inhibitor therapy.
Patients and Methods
Patients and tissue samples. The present study was conducted using 2,439 surgically resected primary CRC cases at the Saitama Cancer Center from October 1999 to March 2014. Patients who had a history of preoperative radiotherapy or chemotherapy, inflammatory bowel disease, or of familial adenomatous polyposis were excluded. Pathological staging was performed according to the tumour, node and metastasis (TNM) classification system (seventh edition) (16). Patients were followed-up until death or survival until June 2015. All tumour samples were analysed after obtaining informed consent from each patient. Tumour tissues were paired with normal colorectal tissues and stored at −80°C. The present study was approved by the Ethics Committee of the Saitama Cancer Center (no. 476). All procedures performed in this study were conducted in accordance with the ethical standards of the Institutional and National Research Committees and with the 1964 Helsinki Declaration and its later amendments.
Mutation analysis. Genomic DNA was extracted from the fresh frozen tissue samples using the standard phenol-chloroform extraction method and assayed for mutation in V-Ki-Ras2 Kirsten rat sarcoma 2 viral oncogene homolog (KRAS), neuroblastoma RAS viral oncogene homolog (NRAS) and v-Raf murine sarcoma viral oncogene homolog B (BRAF). KRAS mutations in exon 2, 3 and 4, and NRAS mutation in exon 2 and 3 were detected by denaturing gradient gel electrophoresis or high resolution melting (HRM) analysis using a Rotor-Gene Q (Qiagen, Hilden, Germany), as described previously (17,18).
BRAF mutations in exon 15 (codon 600) were detected by polymerase chain reaction (PCR)-restriction fragment length polymorphism or HRM, as previously described (19).
Analysis of microsatellite status. The MSI analysis was performed using fluorescence-based PCR, as described previously (8). The MSI status was determined using five Bethesda markers: BAT25, BAT26, D5S346, D2S123 and D17S250. The MSI status was graded as MSI-H with the presence of two or more unstable markers, as MSI-low (MSI-L) with only one unstable marker, and as MSS with no unstable marker. MSI-positive markers were re-examined at least twice to confirm the results. MSI-L was grouped with MSS in this study.
Analysis of mutL homolog 1 (MLH1) promoter hypermethylation. All CRCs with MSI-H were analyzed for MLH1 promoter hypermethylation. Methylation status was investigated by methylation-specific PCR, combined with bisulfite restriction analysis, as previously reported (19).
Statistical analysis. Possible associations between each mutation and the clinicopathological parameters of CRC were assessed using the Fisher's exact test for categorical variables and an independent t-test for the continuous variables. For this analysis, the OS time was calculated from either the date of surgery until the date of death from CRC, or the date of the last visit at follow-up (30 June 2015). The Kaplan–Meier method was used to estimate the distribution of OS, and the log-rank test to compare the distribution of survival time. All p-values were calculated using a paired test and p-values of less than 0.05 were considered statistically significant. All statistical analyses were performed with SPSS Statistics v.20 (SPSS, Inc., IBM Corp., Armonk, NY, USA).
Results
Patient characteristics of stage IV CRC. The frequency of MSI-H was 5.9% in all cases and 3.7% in stage IV, respectively (Table I). The frequency of MSI-H was 8.9% in stage II, the highest among all the stages (Table II). KRAS mutation was detected in 42.6%, NRAS mutation in 3.1% and BRAF mutation in 4.6% of all CRC specimens (Table I). Although frequency of KRAS and NRAS mutation remained unchanged in each stage, the frequency of BRAF mutation increased from 3.4% at stage 0-I to 6.3% at stage IV (p=0.037) (Table II).
Clinicopathological and molecular characteristics of stage IV CRC with MSI-H. Stage IV CRCs were categorized into two groups by MSI status. Stage IV CRCs with MSI-H were more frequently associated with proximal location (p<0.001), large tumour size (p<0.001), undifferentiated histological features (p<0.001) and mucinous components (p=0.038).
Furthermore, stage IV CRC with MSI-H exhibited a different metastatic pattern compared to that with MSS. CRCs with MSI-H were more frequently associated with the presence of peritoneal dissemination (p=0.017) and less frequently associated with the presence of liver metastases (p=0.001). The frequency of curative resection was significantly higher in patients with MSI-H than MSS CRC (p=0.030). In addition, BRAF mutation was observed significantly more frequently in MSI-H (p=0.011), whereas the frequency of the KRAS and NRAS mutations were not significantly different between CRC with MSI-H and that with MSS in stage IV (Table III).
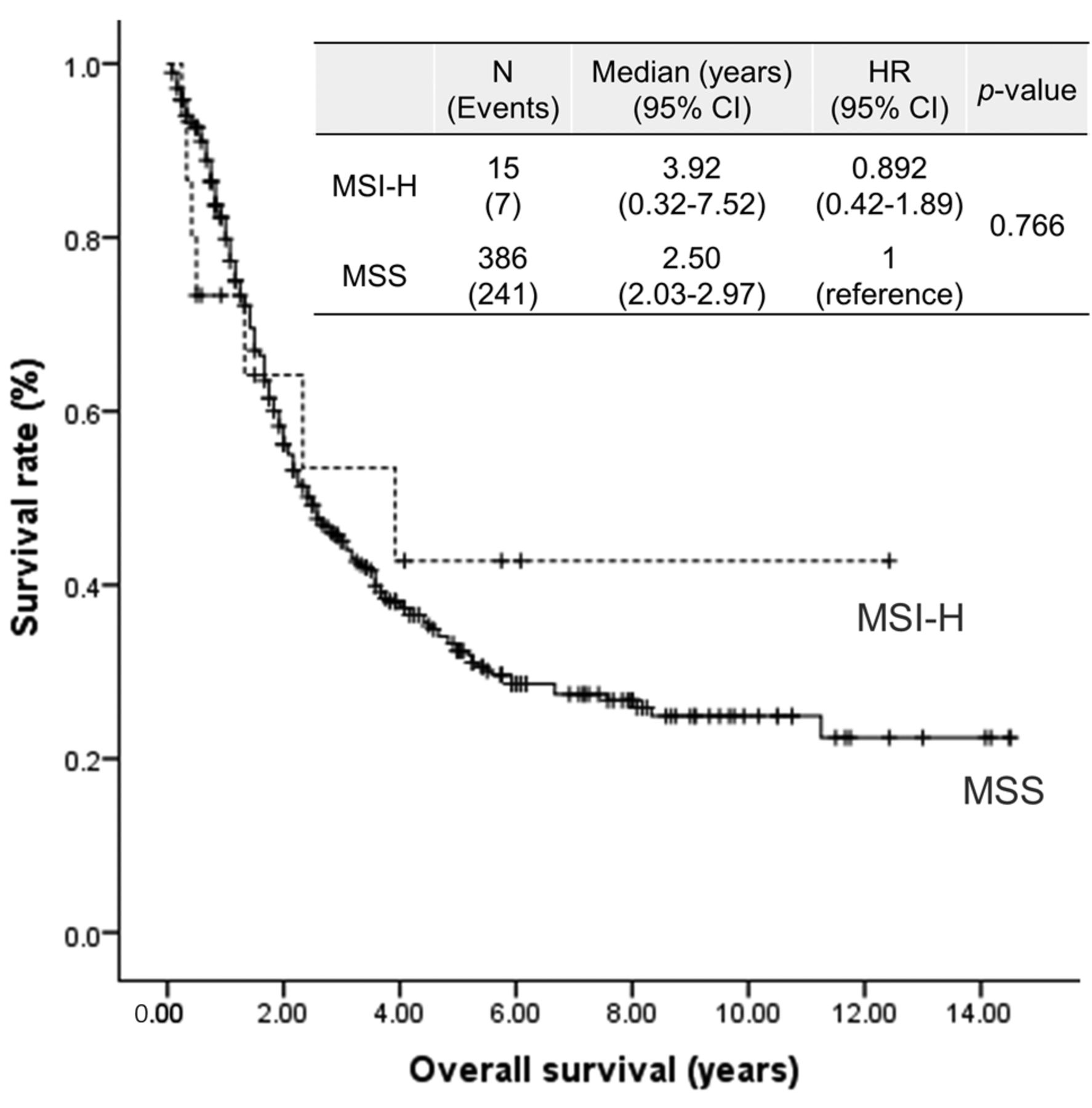
Survival analysis classified by MSI status in stage IV CRC. There was no significant survival difference observed between patients with CRC with MSI-H and those with MSS CRC in stage IV [3.92 vs. 2.50 years; hazard ratio (HR)=0.892, 95% confidence interval (CI)=0.42-1.89, p=0.766]. However, the survival curve for patients with CRC with MSI-H dropped sharply, intersected with that of CRC with MSS, and was stable after 4 years (Figure 1). This suggests that there are two groups in CRC with MSI-H: one with poor prognosis and another with good prognosis. Univariate and multivariate survival analyses for CRC with MSI-H demonstrated that there was no statistical significance, due to a small number of MSI-H cases. However, it did suggest that the metastatic pattern (liver metastasis- or peritoneal metastasis-dominant) was associated with survival in CRC with MSI-H (Table V).
Characteristics of patients with colorectal cancer (CRC).
Rates for mutation (mt) of v-Raf murine sarcoma viral oncogene homolog B (BRAF), V-Ki-Ras2 Kirsten rat sarcoma 2 viral oncogene homolog (KRAS) and neuroblastoma RAS viral oncogene homolog (NRAS), and for high-frequency microsatellite instability (MSI-H) by colorectal cancer stage.
Survival analysis of patients with stage IV CRC classified by metastatic pattern and MSI status. We divided patients with stage IV CRC with MSI-H and MSS into two groups: i) a CRC with peritoneal metastasis-dominant group (PM); and ii) a CRC with hematogenous and lymphogenous metastasis-dominant group (HL). CRC with PM was defined as cases with peritoneal metastasis with fewer than four lymph node metastases. CRC with HL which included CRC with liver metastasis, lung metastasis, or more than three lymph node metastases was defined. Finally, stage IV CRCs were classified into four groups: i) MSI-H CRC with HL (MSI-H-HL); ii) MSI-H CRC with PM (MSI-MSI-H-PM); iii) MSS CRC with HL (MSS-HL); and iv) MSS CRC with PM (MSS-PM).
Patients with MSI-H-HL had the poorest OS rate of the four groups (vs. MSI-H-PM, p=0.006; vs. MSS-PM, p=0.004; vs. MSS-HL, p=0.021). In the multivariate analysis, there was a significant decrease in the median OS rate for those with MSI-H-HL compared to those with MSS-HL (1.33 vs. 2.42 years; HR = 2.34, 95% CI=1.01-4.99; p=0.027) and MSS-PM (1.33 vs. 5 years; HR = 4.03, 95% CI=1.47-11.04; p=0.007). In contrast, all patients survived in the MSI-H-PM group, which demonstrated the best OS rate of the four groups (vs. MSI-H-HL, p=0.006; vs. MSS-PM, p=0.08; vs. MSS-HL, p=0.022) (Figure 2).
Pathological and molecular characteristics of MSI-H-PM and MSI-H-HL. The frequency of KRAS mutation between MSI-H-PM and MSI-H-HL groups was not different (p=1.000). In contrast, the frequency of BRAF mutation in MSI-H-HL cases (40%) tended to be higher than that in MSI-H-PM cases (0%) (p=0.231), no MSI-H-PM case had BRAF mutation.
BRAF-mutated CRC with MSI-H demonstrated a poorer prognosis than wild-type BRAF CRC with MSI-H in stage IV (HR=1.575, CI=0.286-8.673; p=0.601 vs. BRAF wild-type) (Figure 3). MLH1 promoter hypermethylation was observed in eight cases among 15 stage IV CRCs with MSI-H, consisting of two MSI-H-PM and six MSI-H-HL cases (Table IV). OS rates were not significantly different between hypermethylated MLH1 promoter CRC with MSI-H and unmethylated CRC with MSI-H in stage IV (Figure 4).

Survival analysis of patients with stage IV colorectal cancer classified by microsatellite instability (MSI) status. There was no significant survival difference for those with high-frequency MSI (MSI-H) CRC compared to those with microsatellite stable (MSS) CRC. HR: Hazard ratio, CI: confidence interval.
In comparison between MSI-H and MSS, the frequency of BRAF mutation in MSI-H-HL cases was significantly higher than that in MSS-HL cases (p=0.002). Moreover, the curability rate of MSI-H-HL tended to be higher than MSS-HL (p=0.120). The curability rate of MSS-PM was significantly higher than that of MSS-HL (p=0.003) (Table IV).
Discussion
In this study, we found that there were two main groups in stage IV CRC with MSI-H, one with extremely good prognosis (MSI-H-PM), and one with a poor prognosis (MSI-H-HL). In general, CRC with MSI-H is a better prognostic indicator than MSS in stage II and III CRC (10-12), whereas no difference was observed between corresponding groups in stage IV CRC in our study (Figure 1). However, the Kaplan–Meier curve in Figure 1 indicates that stage IV CRC with MSI-H may consist of two different groups: i) a group with poor prognosis, demonstrated by the curve dropping sharply during the early phase; and ii) a group with long-term survival. The univariate and multivariate analyses suggest that the metastatic patterns do indeed affect prognosis (Table V). Several reasons can be considered for why MSI-H-HL in stage IV CRC was found to be associated with a poor prognosis. Firstly, BRAF mutation would adversely affect prognosis. It has been reported that BRAF mutation was a poor prognostic factor in several retrospective studies (8, 20-22). Additionally, in CRC with MSI-H, BRAF-mutated CRC was also found to have poorer prognosis than CRC with wild-type BRAF (23). Similarly to these previous reports, our data show that BRAF-mutated stage IV CRC with MSI-H demonstrated a poorer prognosis than that wild-type BRAF. Whereas, BRAF mutation with MSI-H was not associated with poorer OS than BRAF mutation with MSS in stage I-III CRC (24). Poor prognosis associated with BRAF mutation may be dependent on tumour stage. Furthermore, the frequency of BRAF mutation was 40% in MSI-H-HL compared to none in MSI-H-PM cases. Since not all cases of MSI-H-HL had the BRAF mutation, there may be factors of poor prognosis at play other than the BRAF mutation. In the future, we plan to investigate the mechanism of this association by accumulating more cases and examining multiple cancer-related genes.
Characteristics of patients with stage IV colorectal cancer.
Molecular and pathological features of each type of metastasis according to microsatellite instability (MSI) status in colorectal cancer (CRC).
Univariate and multivariate overall-survival analysis in stage IV colorectal cancer with high-frequency microsatellite instability.
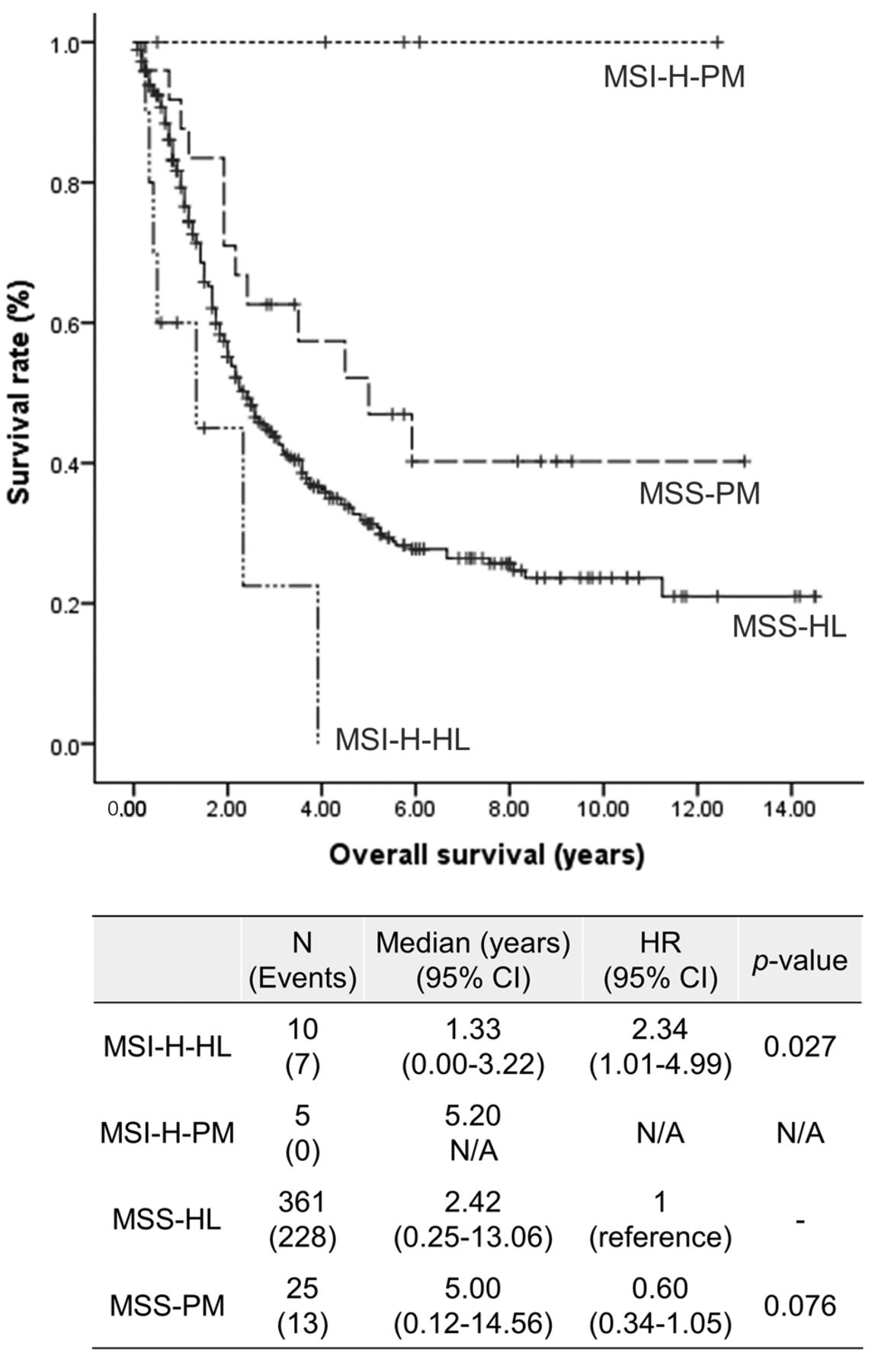
Survival analysis of patients with stage IV colorectal cancer CRC classified by metastatic pattern and microsatellite instability (MSI) status. Those with hematogenous/lymphogenous metastasis-dominant MSI-high (MSI-H-HL) CRC had the poorest overall survival out of the four groups [vs. peritoneal metastasis-dominant (MSI-H-PM): p=0.006; vs. microsatellite stable (MSS): p=0.004; vs. MSS-HL: p=0.021]. All cases in the MSI-H-PM group survived and MSI-H-PM had the best overall survival rate out of the four groups (vs. MSI-H-HL: p=0.006; vs. MSS-PM: p=0.08; vs. MSS-HL: p=0.022). HR: Hazard ratio, CI: confidence interval.

Survival analysis of patients with stage IV colorectal cancer classified by v-Raf murine sarcoma viral oncogene homolog B (BRAF) mutation. Patients with BRAF mutation (mt) had a poorer prognosis compared to those with wild-type (WT) BRAF. HR: Hazard ratio, CI: confidence interval.

Survival analysis of patients with stage IV colorectal cancer classified by the methylation status of the mutL homolog 1 (MLH1) promoter. Survival of patients with hypermethylation of the MLH1 promoter (+) was not significantly different from that of those without MLH1 promoter hypermethylation (−). HR: Hazard ratio, CI: confidence interval.
In general, CRC with MSI-H exhibits a large tumour size and has high growth ability but less metastasis (18, 25, 26). Therefore, once these tumours acquire metastatic potential, the prognosis might worsen. From a recent large-scale genome analysis, Guinney et al. showed there to be four consensus molecular subtypes (CMS) of CRC (27). From this study, the CMS1 population, which tended to have hypermutated type (high number of somatic mutation events in the genome) and BRAF mutation, had a very poor survival rate after relapse, but good OS and relapse-free survival. A part of the CMS3 population tended to have hypermutated type and KRAS mutation. MSI-H-HL and MSI-H-PM in our study may correspond to the CMS1 and CMS3 populations, respectively.
In contrast with the poor prognosis of MSI-H-HL CRC, patients with MSI-H-PM CRC had a prolonged OS rate, and there were no deaths during the observation period. Vatandoust et al. reported that patients with PM CRC who underwent curative surgery could expect long-term survival (28). Similarly to Vatandoust et al.'s report, MSI-H-PM also conferred a better prognosis in patients with curatively resected stage IV CRC in our study.
The following are considered to be the reasons for why MSI-H-PM in stage IV CRC has a good prognosis. Firstly, MSI-H-PM cases did not have BRAF mutation, which is a poor prognostic factor. Even though BRAF-mutated CRC is likely to develop PM (29), no MSI-H-PM cases were BRAF-mutant. Moreover, the report that BRAF-mutated CRCs with MSI-H are less likely to exhibit peritoneal metastasis supports our results (30). Thus, our detailed analysis suggests that the frequency of BRAF mutations in PM is dependent on the MSI status. Additionally, curatively resected MSI-H-PM cases could be considered as having the same oncological status as during the early stage. Therefore, MSI-H-PM cases may maintain a better prognosis.
In this study, a multivariate analysis could not be performed sufficiently due to the small number of CRC cases with MSI-H. Frequency of CRC with MSI-H is approximately 10-15% in Western countries, whereas that in Asia was reported to be 5.5-7.3% (18, 31, 32), lower than in Western countries. However, despite the small number of cases, there was a significant prognostic difference between MSI-H-HL and MSI-H-PM cases. In a recent clinical trial, the immune checkpoint inhibitor, pembrolizumab prolonged disease-free and OS rates for metastatic CRC with MSI-H (15). Thus, MSI-H is an attractive biomarker for immunotherapy and these findings provide useful information for the adaptation of CRC immunotherapy. In conclusion, we found that the difference in metastatic pattern in stage IV CRC with MSI-H affects prognosis.
Acknowledgements
The Authors would like to thank the staff of the Divisions of Gastroenterological Surgery and Molecular Diagnosis and Cancer Prevention, Saitama Cancer Center.
Footnotes
This article is freely accessible online.
Compliance with Ethical Standards
This study was approved by the Ethics Committee of the Saitama Cancer Center.
Conflicts of Interest
The Authors declare that they have no competing of interest in regard to this study.
- Received October 28, 2016.
- Revision received November 14, 2016.
- Accepted November 15, 2016.
- Copyright© 2017 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Effect of Trimetazidine on Diathermy-related Thermic Injury of the Rat Liver
- Clinical Impact of Primary Tumor Site in Stage IV Colorectal Cancer: A Statewide Cohort Study
- Reovirus sensitizes microsatellite stable colorectal cancer to anti-PD-1 treatment via cross-talk in innate and adaptive immune systems
- Short- and Long-term Histological Changes in Liver Parenchyma After Different Resection Methods and Their Potential Role in Treatment of Colorectal Liver Metastasis
- The Clinical Impact of the Genomic Landscape of Mismatch Repair-Deficient Cancers
- A Blueprint to Advance Colorectal Cancer Immunotherapies