


Abstract
Background: Soft-tissue sarcomas (STS) of the distal extremities are a rare disease entity, hence proper treatment strategy is not well established. We evaluated the local control, survival and complications of treating sarcomas in the wrist, hand, ankle and foot with limb-sparing surgery (LSS) and postoperative radiotherapy (PORT). Patients and Methods: Seventeen patients with STS in wrist, hand, ankle and foot who received PORT after LSS from August 2008 to November 2015 were retrospectively reviewed. Primary outcome was 5-year local recurrence-free survival (LRFS). Secondary outcomes were 5-year distant metastasis-free survival (DMFS) and toxicities. Results: The median age was 32 (range=12-78) years. The most frequent STS location was the foot in 11 patients (64%) followed by two patients each in the wrist, hand and ankle, respectively. Fourteen patients (82%) underwent wide resection with flap grafts and the same number of patients achieved clear resection margins. The median postoperative radiation dose was 54 (range=46-60) Gy. Five patients also received chemotherapy. At a median follow-up of 39 (range=6-87) months, 5-year LRFS and DMFS were both 100%. Only one patient experienced grade 3 radiation dermatitis and there was no major wound complication. Radiation-induced bone fracture occurred in two patients. Conclusion: PORT after LSS showed excellent local control for STS in the wrist, hand, ankle and foot. Considering the good local control and saving of limb function without any significant toxicity, the combination of LSS followed by PORT could be an appropriate and safe modality for STS of the distal extremities.
Limb-sparing surgery (LSS) combined with postoperative radiotherapy (PORT) is the recommended treatment for soft-tissue sarcoma (STS) of the extremities based on three sentinel randomized trials (1-3). However, the application of the approach is controversial for lesions located in distal extremities such as the wrist, hand, ankle and foot. For surgeons, it is difficult to achieve both wide resection margins and preservation of function because of the proximity of complex neurovascular bundles. From a radiation oncologist's point of view, the distal extremities have been considered poorly tolerant of radiation due to the difficulty in sparing a strip of the limb circumference in order to prevent subsequent lymphedema and pain. For this reason, some physicians still advocate radical amputation as the primary treatment of STS of the distal extremities.
STS account for fewer than 1% of malignant tumors. Most of these arise in the trunk, or proximal extremities, and seldom involve the distal extremities. Because of the rarity of this disease, the management of STS in the wrist, hand, ankle and foot is not well established.
At our center, we have treated such patients with PORT after LSS not only for tumor control but also for preservation of function. PORT has the advantage that the complete pathological review is available for histology and margin status. In addition, it has a lower risk of major wound complications (4, 5).
We tried to reduce the risk of late toxicities, such as subcutaneous fibrosis, joint stiffness and edema, through minimizing the target volume. This was possible through the precise review of magnetic resonance imaging (MRI) and the close cooperation between surgeon and radiation oncologist.
The purpose of this study was to report the rates of local control, survival and toxicities of patients treated at a single large tertiary referral center with LSS combined with PORT for STS of the distal extremities.
Patients and Methods
Patient and tumor characteristics. Seventeen patients with STS involving the wrist, hand, ankle and foot were treated with PORT after LSS between August 2008 and November 2015. Patients with metastatic disease were excluded. All clinical data were obtained through retrospective review of the patient's records.
Patient and tumor characteristics are summarized in Tables I and II. The median age was 32 (range=12-78) years. There were 10 female and seven male patients. The most frequent STS location was the foot in 11 patients (64%). Right-sided tumor was more prevalent (64%). The median tumor size was 3 cm (range=0.7-6.5 cm), and 14 patients had a tumor size of 5 cm or less (82%). Eight patients presented with high-grade tumors (47%), and there were various histopathologies of STS in the present cohort (Table II).
Treatment. Before referral to the Sarcoma Department at our center, 14 patients (82%) had already had their tumors excised. Except for one patient who showed clear resection margins, 13 patients needed re-excision due to gross residual tumor (n=2), or positive (n=4) or unknown (n=7) resection margin status. Excision or re-excision was performed with the goal of obtaining a tumor-free margin of 2 cm, if possible. If needed, tendons, periosteum and parts of bone were resected locally. A patient with 5.1 cm-sized mass in right second finger and another patient with 2 cm tumor in left fourth toe underwent amputation of the involved digits. However, further resection of neighboring extremities was not carried out, hence we also included these patients in the analyses. Thirteen patients underwent excision with free-flap reconstructions using superficial circumflex iliac perforator or anterolateral thigh perforator. One patient was treated with excision and local flap reconstruction. Two patients underwent curettage and filling, and the last patient underwent excision alone. After the completion of all surgical resections, negative resection margins were achieved in the majority of patients (82%, n=14). Two patients showed positive resection margins and one patient had an unknown margin status. An unknown margin status was considered to be at as high a risk for local recurrence as a positive margin, thus we put positive and uncertain margin status together for the analyses.
The planning computed tomography (CT) was obtained by CT scanner in the most suitable position for each patient using customized immobilization devices considering planning fields. CT slice thickness was 2.5 mm. RT was administered using external beam techniques. Six megavoltage photon beam was employed using single to four fields such as anterior, posterior, lateral, or oblique fields.
Irradiation of the whole circumference of the extremity was avoided. The joint, sole, heel, and Achilles tendon were spared if it did not compromise the coverage of the suspected tumor spread. Although there are standard radiation field margins for STS (6), it is hard to uniformly apply to the distal extremities while meeting the previously mentioned conditions. The tumor bed was delineated based on initial enhanced MRI. For clinical target volume (CTV) delineation, we modulated the margins case by case. We set standard margins of CTV, 1.5 cm radially and 4 cm longitudinally, in only one case. The other cases, in order to prevent long-term toxicity, smaller margins (radial 0.5-1 cm, longitudinal 1-3 cm) were applied. The planning target volume (PTV) margins were 0.5-0.7 cm. In 14 patients, the radiation field was reduced for the latter 10-20 Gy irradiation. Reduced PTV volume was expansion of 0.5-1 cm from the tumor bed. The development of MRI and wide excision with flap graft in the majority of cases (n=14, 82%) justified our protocol for smaller target volumes. Because all surgical management was carefully performed in order to avoid tumor contamination, the inclusion of scars in the CTV was not mandatory.
The median postoperative radiation dose was 54 Gy (range=46-60 Gy). The fraction size was 2 Gy, except for one patient with a fraction size of 1.8 Gy. One patient was also treated with neoadjuvant and adjuvant chemotherapy with doxorubicin/ifosfamide regimen on Children's Oncology Group (COG) protocol ARST0332 for non-rhabdomyosarcoma STS. Four patients received adjuvant cyclophosphamide, vincristine, adriamycin, and dacarbazine combination chemotherapy. The rest of the patients did not receive any chemotherapy (Table I).
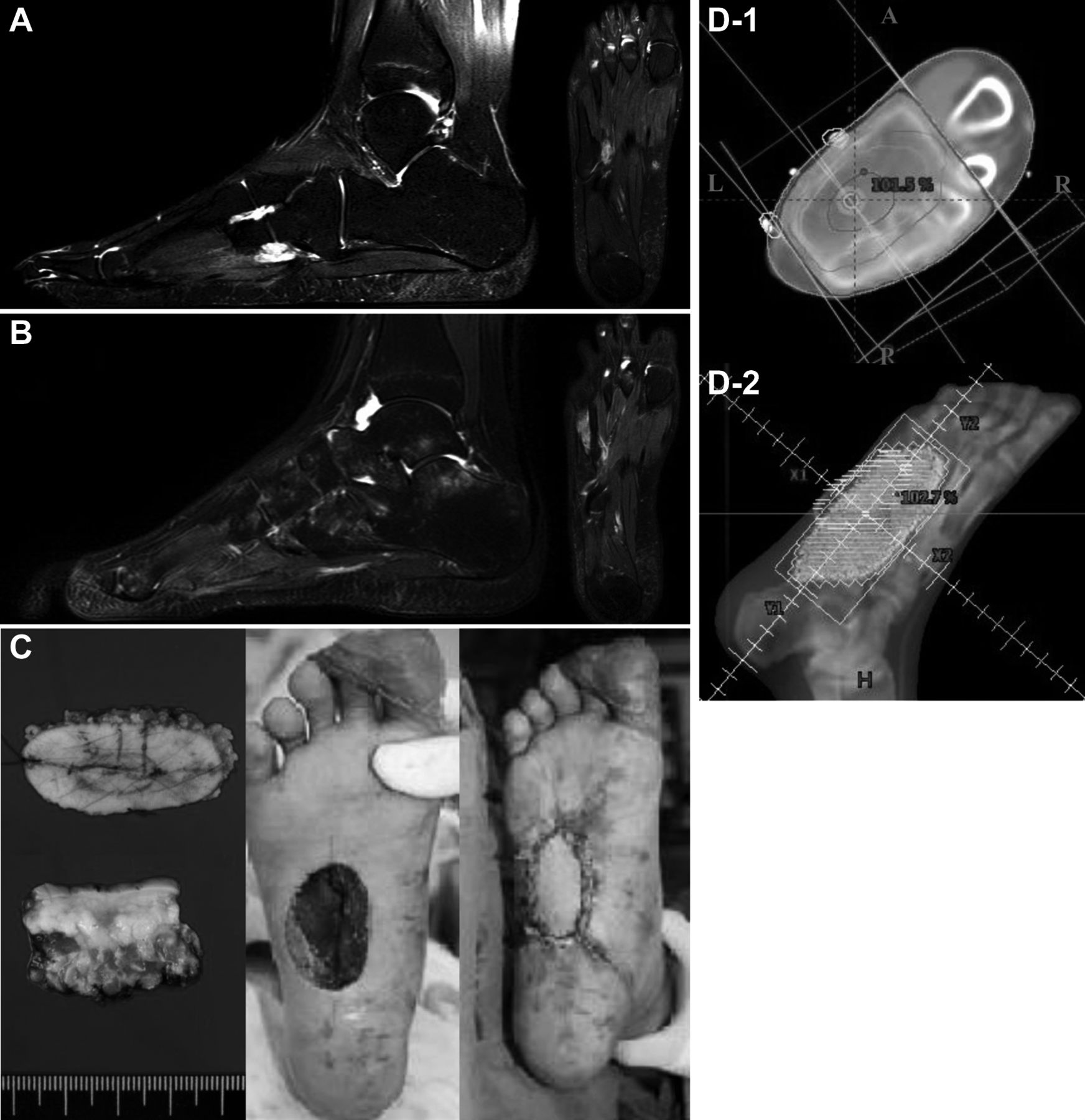
Figure 1 shows an example of the treatment process: A 12-year-old girl was diagnosed with synovial sarcoma in her right sole, and treated with neoadjuvant chemotherapy, LSS with free flap and PORT.
Follow-up and statistics. The median follow-up for all patients was 39 (range=6-87) months from the last resection date. Acute and late toxicities were evaluated using Common Terminology Criteria for Adverse Events (CTCAE) v.4.03.(7) For scoring major wound complications, we used the criteria of O'Sullivan et al. (5) because the CTCAE criteria for wound complication did not fit for evaluating cases of distal extremities. Acute toxicities were defined as adverse events within 3 months after completion of RT. Patients were followed-up every 3 months for the first 2 years with ultrasonography (US) or MRI of the primary site and chest CT. After that time, follow-up was every 6 months until 5 years, and annual check-up thereafter was recommended with US/MRI and chest CT. The Kaplan–Meier method was used to estimate local recurrence-free survival (LRFS) and distant metastasis-free survival (DMFS).
Results
We did not intend to exclude patients with recurrent disease, but there was no such case anyway. With 17 patients who received PORT, the 5-year LRFS and DMFS were both 100%. No death was reported. Ten patients experienced radiation dermatitis and only one of them had grade 3 dermatitis. Grade 1 lymphedema was reported in six patients. There was no major wound complication.
Regarding late toxicities, fibrosis occurred in one patient with grade 1. Hyperpigmentation and decreased joint range of motion were reported in two and three patients, respectively. All of the cases were grade 1. Two patients experienced radiation-induced bone fractures. A 13-year-old boy was diagnosed with right fifth metatarsal fracture post-RT at 8 months of follow-up. The metatarsal bone was involved in the RT field and irradiated with 56 Gy. The patient complained of pain on walking and underwent cast immobilization for a month. The other patient was a 26-year-old man who did not have any symptoms. On regular follow-up x-ray, there was a fracture of his left first metatarsal bone which was covered by the initial PTV and prescribed 50 Gy. However, this patient did not need any treatment.
Patient and tumor characteristics.
Discussion
Our data report favorable oncological outcomes of STS of the distal extremities using PORT after LSS. Moreover, few toxicities were observed. Although there are several studies reporting the result of LSS combined with PORT (8-10), as far as we know, this is the latest cohort of patients treated from 2008 to 2015 with homogenous treatment strategy, and the first report in Asia.
We summarized the former trials published since 1990 in Table III. Except for Jyothirmayi et al. (11), the studies reported 10-year LRFS of 74-91% and DMFS of 74-87% (8-10, 12). Due to high incidence of intracapsular excision, half of the patients in the study by Jyothirmayi et al. showed positive resection margin or gross residual tumors. This may be the reason for the poor oncological outcome of the study. Although the current study had disadvantages of having a small cohort and short median follow-up of 3.3 years, we report excellent results of 5-year LRFS and 100% DMFS. This is comparable to the other studies where 5-year LRFS was 80-90% (8-10).
Histopathology of tumor.
We routinely treated patients with PORT after LSS, rather than preoperative RT. According to a Canadian randomized trial, there is no difference in DFS and overall survival associated with preoperative RT and PORT (5, 13). The study also showed greater acute wound complications with preoperative RT and greater late fibrosis and limb edema with postoperative setting (5). Both preoperative RT and PORT have advantages and disadvantages, and we put much value on the strengths (complete pathologies, lower wound problems) of the postoperative setting.
Usually, the prescribed dose of radiation for PORT is higher (median=60-64.8 Gy) than the dose for preoperative settings (median=50-50.4 Gy). However, the dose we irradiated for PORT was rather lower than in the other studies (median=54 Gy) (Table III) and we did not increase the RT dose for the patients with positive (n=2) or unknown (n=1) margin status in order to avoid late complications; they received 54, 56 and 60 Gy, respectively, and with 10-29 months of follow-up, they have not experienced recurrence.
One of the reasons for the good local control in the present study is that most patients underwent complete excision and flap graft surgery. Consequently, 82% of the patients had negative resection margins. It is well known that a positive resection margin status significantly increases local recurrence, and local recurrence itself has a strong association with the development of subsequent metastasis and poor survival (14, 15). Secondly, the majority of patients presented with small-sized tumor (≤5 cm) which facilitated the achievement of clear resection margins. In addition, small size itself is good prognostic factor for distant metastasis so that this surely attributes to excellent 5-year DMFS (2). Lastly, 15 patients (88%) were aged under 50 years, which is a favorable prognostic factor for local recurrence (2).
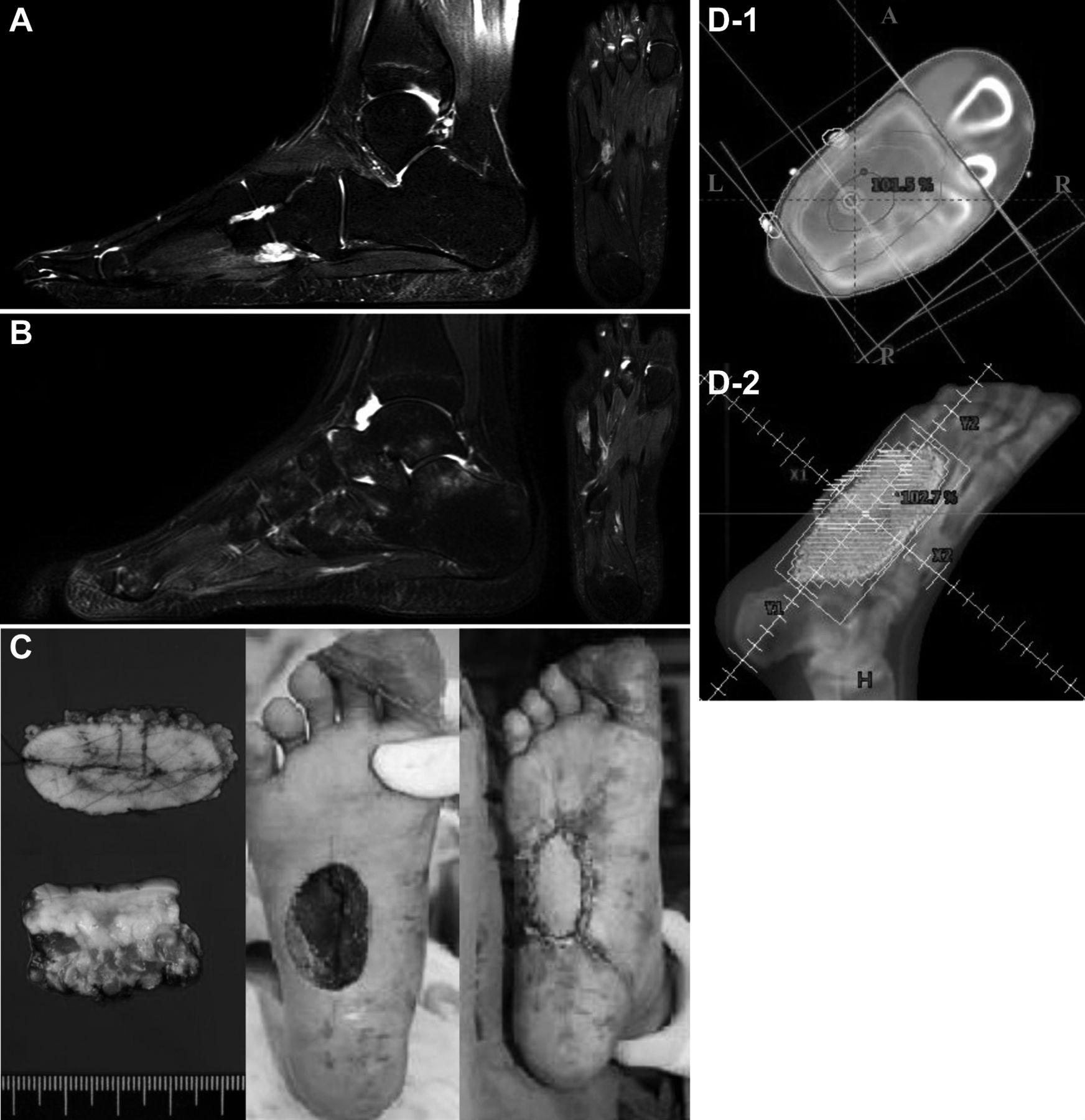
Synovial sarcoma of the right sole in a 12-year-old girl. A: Initial T2-weighted imaging of the foot shows a 17 mm-sized high signal mass with lobulated contour at the right fourth and fifth metatarsal base (white arrows) B: After two cycles of neoadjuvant doxorubicin and ifosfamide, this mass become indistinct in T2-weighted imaging. C: Postoperative gross specimen showed no definitively visualized tumor, and superficial circumflex iliac artery perforator flap reconstruction was performed for the excision site. D-1: With inversion of the right foot, left-anterior-oblique and right-posterior-oblique beams were used for planning. Tumor bed, clinical and planning target volumes were delineated in red, orange, and pink lines, respectively. D-2: Digitally reconstructed radiograph was created from the left-anterior-oblique view.
Summary of previous reports on treatment results of limb-sparing surgery combined with radiotherapy for soft tissue sarcoma of the distal extremities.
Previous studies irradiated over 60 Gy in the postoperative setting reported few severe toxicities (Table III). However, they all have the limitation of a retrospective nature and none of them reported on radiation-induced bone fractures.
With a median dose of 54 Gy, we reported two cases (12%) of bone fracture which occurred in a metatarsal bone. These fracture sites were included in the RT field and irradiated with 56 and 50 Gy, respectively. Dickie et al. evaluated the incidence of bone fractures in 691 patients with lower extremity STS (16). After a median follow-up of 7 years, 31 fractures were reported (4.5%). The average interval between RT and fracture was 3 years. Patients presenting bone fractures were treated with a maximum dose to bone of 64 Gy and a mean dose of 45 Gy. In contrast, for the no fracture group, the maximum irradiated dose was 59 Gy and the mean dose was 37 Gy. This study showed that the risk of bone fracture is related to RT dose. With no toxicities over grade 3 or recurrences, we carefully suggest that a dose under 60 Gy is sufficient for the elimination of microscopic disease. Moreover, it can lower the risk of late toxicities including bone fractures. Of course, efforts for achieving clear resection margin must be made before dose reduction.
The necessity for PORT in patients with negative resection margins can be doubted because of the findings of Lin et al. (17). They retrospectively reviewed 83 patients with STS of the hand or foot who underwent LSS. They reported that RT improved local control in patients who did not undergo re-excision (considered as positive resection margin) (n=17, p=0.02). However, in patients who did undergo re-excision (considered as negative resection margin), RT failed to improve local control (n=13, p=0.51). Could we therefore omit PORT in patients with clear resection margins? Lin et al. 's study also had limitations of small sample size and retrospective nature. Even with wide excision, there is a limitation of safety margins attributed to the anatomy of the hand and foot unlike the other extremities. There is no prospective trial on omitting PORT in patients with clear resection margin status, and PORT has shown acceptable toxicities in patients with sarcoma of distal extremities. Therefore, for now, the standard of care should be a multimodality strategy.
The sample size of the current study is small. The present study was also retrospective and had a relatively short follow-up period. However, due to the rarity of STS of the distal extremities, we decided the outcomes of 17 patients were worth reporting. To our knowledge, this is a first report in an Asian population. Due to the short accrual period, we were able to treat patients homogeneously.
As a conclusion, PORT after LSS showed excellent local control for STS in the wrist, hand, ankle and foot. Considering the good local control and sparing of limb function, the combination of LSS and PORT could be an appropriate and safe modality for STS of the distal extremities.
Acknowledgements
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2013R1A1A2011346) and by a grant of the Korea Health Technology R&D Project health & Welfare, Republic of Korea (grant number: HI15C0972).
- Received July 13, 2016.
- Revision received July 30, 2016.
- Accepted August 1, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}