


Abstract
Background: Gastric cancer in pregnant women is rare. When physicians encounter a patient with pregnancy-associated gastric cancer, it is important to take a multidisciplinary approach and respect the will of the patient. We herein describe a case of gastric cancer during pregnancy. Case Report: A 36-year-old woman at 18 weeks of gestation was diagnosed with advanced gastric cancer. She underwent totally laparoscopic distal gastrectomy at 23 weeks of gestation and four cycles of FOLFOX6 without any severe toxicity. At 36 weeks of gestation, a healthy baby was born. After delivery, the patient was treated with additional chemotherapy. She has finished chemotherapy and has been followed-up without recurrence for 1 year after operation. Conclusion: Laparoscopic gastrectomy followed by chemotherapy for gastric cancer during pregnancy might be a safe option.
The occurrence of cancer during pregnancy is dilemmatic with respect to the patient's health and fetal integrity. The most common types of pregnancy-associated cancer include cervical cancer, breast cancer, malignant melanoma, and lymphoma (1). Among them, pregnancy-associated gastric cancer is quite rare. However, information on the exact incidence rate is limited (2). Although the definition of pregnancy-associated gastric cancer is unclear, it is generally accepted as gastric cancer diagnosed during gestation. The disease is characterized as follows: most patients have at an advanced disease stage at diagnosis, and operability and survival rate are relatively low (2). No standard treatment has been established because of its rarity, delay in diagnosis, and limited treatment options.
We herein report a case involving a 36-year-old woman diagnosed with gastric cancer at 18 weeks of gestation. The patient successfully underwent totally laparoscopic distal gastrectomy followed by chemotherapy.
Case Report
A 36-year-old woman, gravida 3, para 2, was admitted to the emergency room for evaluation of hematemesis and dizziness in April 2015 at 18 weeks of gestation. One week earlier, she had been admitted to the same hospital and underwent conservative care because of diarrhea and epigastric soreness. On her second admission, she was normotensive but tachycardic, with a pulse rate of 112 beats per minute. Laboratory testing revealed anemia (hemoglobin level of 8.2 g/dl and hematocrit of 24.6%). Esophagogastroduodenoscopy revealed a large distinct protruding mass with a central ulcer at the gastric angle to the lower body (Figure 1). Endoscopic ultrasound showed a 4-cm hypoechoic mass in the fourth layer (Figure 2). The endoscopic biopsy confirmed a poorly cohesive carcinoma, and the patient was referred to the Department of Gastrointestinal Surgery for surgical treatment of gastric cancer.
The patient underwent totally laparoscopic distal gastrectomy with D2 lymph node dissection and Billroth-II reconstruction with curative intent at 23 weeks of gestation. Macroscopically, the elevated lesion was located at the lesser curvature of the lower body and was approximately 6×5 cm in diameter (Figure 3). The surface of the mass was ulcero-infiltrative and penetrated the serosa but not the adjacent structures. Microscopically, multiple lymph nodes were involved and the surgical margin was negative for tumor cells. The tumor was a diffuse-type carcinoma according to the Lauren classification. During the operation, only one seeding nodule at the pancreatic capsule was removed. The lesion at the pancreatic capsule was pathologically confirmed as a peritoneal metastasis. The final diagnosis was gastric cancer with peritoneal metastasis, stage IV (pT4aN3bM1).
Following the operation, the patient's postoperative course was unremarkable and fetal ultrasonography revealed the well-being of the fetus (Figure 4). The patient underwent four cycles of FOLFOX6 [leucovorin, 5-fluorouracil (5-FU), and oxaliplatin] before delivery and subsequently delivered a healthy baby weighing 2,570 g at 36 weeks of gestation. The Apgar scores were 8 and 9 at 1 and 5 minutes, respectively. Pathological examination of the placenta revealed no metastasis. The patient resumed chemotherapy 13 days after delivery. After 21 chemotherapy cycles, abdominal computed tomography revealed no evidence of aggravation of metastasis. At the time of writing, the patient and baby were doing well and undergoing routine follow-up examinations.
Discussion
The incidence of cancer during pregnancy is approximately 1 per 1,000 pregnant women (1). In particular, pregnancy-associated gastric cancer is an extremely rare clinical situation. It has also been reported to have an unfavorable prognosis, with maternal 1- and 2-year survival rates of 18.0% and 15.1%, respectively (2). There are several possible reasons for such a poor prognosis. Firstly, delayed diagnosis is the main reason, because it is difficult to distinguish between the early symptoms of gastric cancer and pregnancy-induced symptoms such as nausea and vomiting. In addition, the physician and patient often avoid performing diagnostic examinations such as esophagogastroduodenoscopy during pregnancy in order to avoid harming the fetus. As a result, most cancers are detected after reaching an advanced stage or inoperable state. SecondIy, the therapeutic approach is usually limited due to two conflicting factors: the safety of the fetus and treatment of the mother. Thirdly, pregnancy is characterized by specific biological and hormonal changes that can adversely affect gastric cancer. For example, immunosuppression, elevated estrogen, and increased circulatory blood flow during pregnancy render the mother susceptible to the rapid growth of cancer (3). Maeta et al. reported distinct characteristics of gastric cancer caused by the specific conditions of pregnancy, namely the predominance of poorly differentiated adenocarcinoma with a scirrhous growth pattern, advanced cancer, and peritoneal metastasis (4). In addition, Furukawa et al. reported that the diffuse microscopic type of gastric cancer represented 75% of pregnancy-induced gastric cancer cases (5). Most of these exhibited the same characteristics of gastric cancer as in young patients and were consistent with the pathological findings in our case.
Generally, the management of pregnancy-associated gastric cancer is dependent on the gestational age as well as the stage of the gastric cancer. Moreover, the patient's desire for a child is also an important factor in choosing the optimal treatment. If the gastric cancer is diagnosed prior to 22 weeks of gestation and is operable, surgery is recommended after termination of the pregnancy by induced abortion; at weeks 22 to 27 of gestation, induced premature delivery or careful monitoring is instead recommended, followed by surgery; at week 28 of gestation and beyond, surgery can be performed after delivery (2). In cases of inoperable gastric cancer, the use of chemotherapy during pregnancy needs to be established. Adjuvant or palliative chemotherapy without termination of the fetus is known to be possible in the second and third trimesters because the most chemotherapy agents are felt to be generally safe in pregnancy (6). Thus, the determination of the therapeutic plan in pregnant patients is complicated and individualized within these general guidelines.
The decision to use chemotherapy during pregnancy is difficult because of the possible risk of teratogenicity and the lack of clinical evidence of the long-term effects. The evidence for the selection and use of a chemotherapeutic regimen during pregnancy is limited due to the low incidence of this treatment. Only a few case reports have described the use of a paclitaxel and S-1 regimen during pregnancy, and the baby was reported to be within the normal limits for height, weight and neurological development, although mild intrauterine growth retardation was initially observed (7). The US Food and Drug Administration safety rating for the use of oxaliplatin and 5-FU during pregnancy is class D. Congenital fetal abnormalities have been reported in a number of pregnancies in which 5-FU was administered during the first trimester, with a reported rate of 14% to 19% (8). However, this rate is significantly reduced to 1.3% when administration occurs in the second and third trimesters (8). This is evident in previous case reports, as well as in our patient, when chemotherapy was administered from the second trimester onward and no fetal malformations were reported.
The strength of the present report lies in it being the first reported case of laparoscopic gastrectomy for pregnancy-associated gastric cancer; all previously described patients underwent open gastrectomy as far as we are aware. However, there are possible disadvantages of laparoscopic surgery during pregnancy, including trauma to the pregnant uterus, technical difficulty due to the enlarged uterus, the potential risk of reduced uterine blood flow due to increased intra-abdominal pressure, and carbon dioxide absorption. On the other hand, the laparoscopic approach provides some advantages for pregnant patients. Above all, it induces less fetal stress due to reduced postoperative narcotic use and minimal manipulation of the uterus during surgery. Although short-term follow-up has suggested equal or superior safety with the laparoscopic approach compared to the open method, large series of data on its long-term safety are unavailable.

Esophagogastroduodenoscopy showed a 4-cm mass with ulceration in the lesser curvature of the lower body.

Endoscopic ultrasound showed a 4-cm hypoechoic mass in the fourth layer.
In conclusion, the possibility of gastric cancer should not be overlooked in the treatment of intractable or unusual gastrointestinal symptoms in pregnancy and should be endoscopically investigated. A multidisciplinary team consisting of a surgeon, oncologist, obstetrician, and neonatologist, as well as taking into consideration maternal desires regarding the pregnancy, are important in deciding the treatment plan. In addition, management of the cancer is determined according to gestational age and the stage of the gastric cancer. Laparoscopic gastrectomy followed by FOLFOX chemotherapy for gastric cancer during pregnancy might be a safe option, although the long-term effect of this regimen remains unknown.

A 6×5 cm tumor was located at the lesser curvature of the lower body.
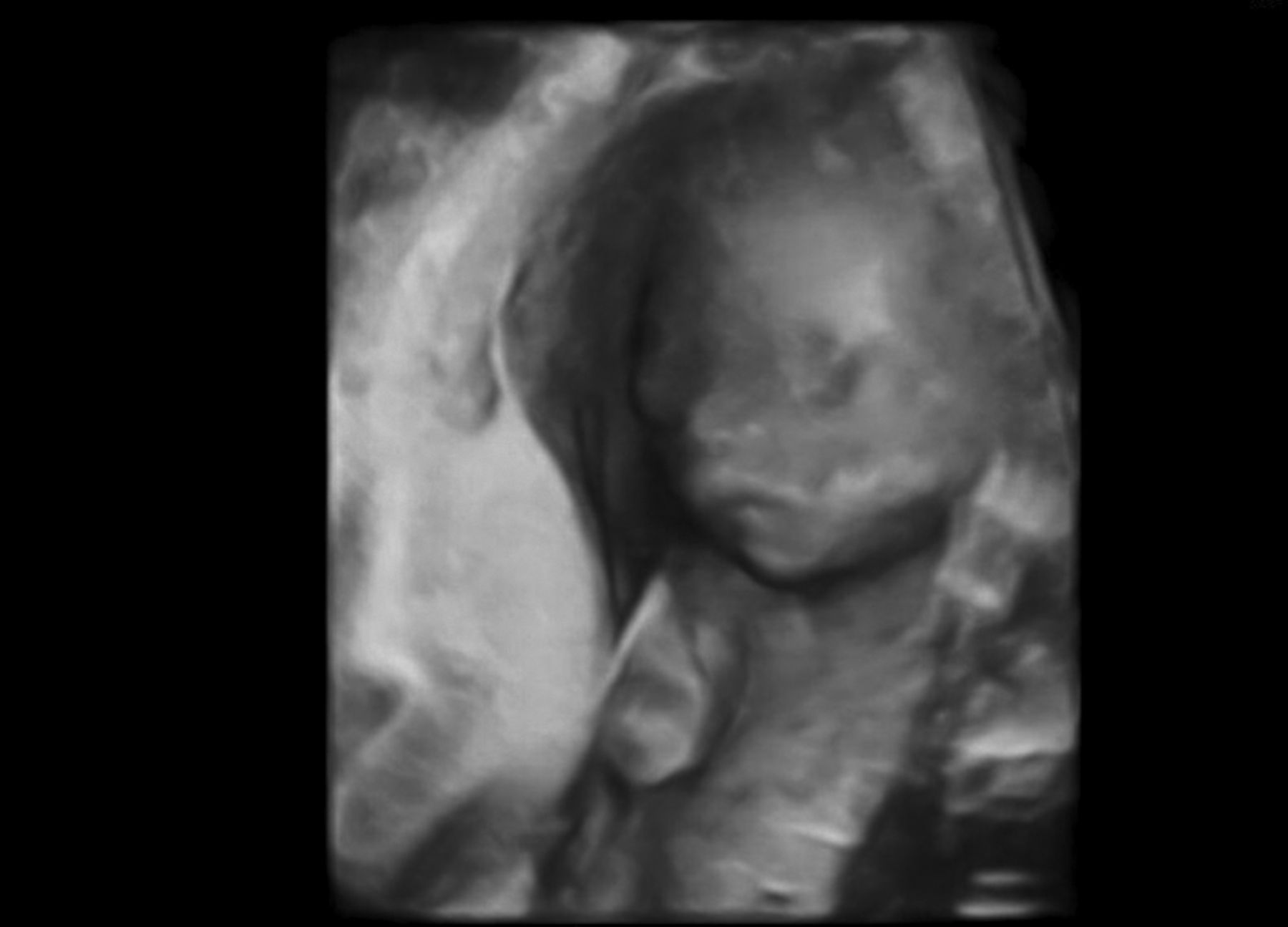
Following surgery, fetal ultrasonography confirmed the well-being of the fetus.
- Received July 8, 2016.
- Revision received July 31, 2016.
- Accepted August 1, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.