


Abstract
Quadruple synchronous primary neoplasms are very rare with only three cases reported in the English-speaking literature to date. Collision tumors are also rare entities, especially of the appendix. We herein report a case of synchronous quadruple primary neoplasm in a 95-year-old female. She was diagnosed with colon adenocarcinoma, sessile serrated adenoma of the appendix and a collision tumor composed of a well-differentiated neuroendocrine tumor and Schwann cell hamartoma. Histological examination and immunohistochemistry supported these four lesions as separate entities. This case is unique because we report the diagnosis of quadruple synchronous primary, an extremely rare occurrence, in addition to a collision tumor of the appendix. We also provide a review of the literature for synchronous neoplasms and collision tumors.
- Synchronous
- multiple primary malignant neoplasms
- neuroendocrine tumor
- sessile serrated adenoma/polyp
- schwannoma
- collision tumor
- colon adenocarcinoma
Multiple primary neoplasms (MPNs) in a single patient are a relatively rare occurrence. MPNs are classified as either synchronous or metachronous depending on the time of diagnosis. Synchronous cancers are diagnosed either simultaneously or within 6 months of each other and metachronous cancers are diagnosed at least 6 months apart. The prevalence of MPNs varies significantly between 0.73% and 16% (1, 2) depending on the source and synchronous cancer is much rarer than metachronous cancer. The prevalence of MPNs has grown in recent years and is expected to increase due to improved cancer survivorship and more sensitive cancer diagnostic techniques (3).
In this report, we describe a case of a 95-year-old Caucasian woman with synchronous quadruple primary neoplasms with two of the tumors being collision tumors located in the appendix. She was diagnosed with adenocarcinoma of the colon, collision tumor of neuroendocrine tumor and Schwann cell hamartoma in the appendix and sessile serrated adenoma of the appendix. To the best of our knowledge, this particular combination of synchronous malignancies has never been previously reported.
Case Report
A 95-year-old Caucasian woman presented with an episode of nausea, vomiting and abdominal distention. Her past medical history was significant for previous episodes of small bowel obstruction, type II diabetes mellitus, iron deficiency anemia, peripheral neuropathy and hypertension. She had no history of melena, hematochezia or diarrhea. Laboratory findings and clinical examination at this time were unremarkable. Her family history was non-contributory. Computed tomography (CT) revealed a large cecal mass (Figure 1A) causing obstruction of the terminal ilium and a mildly enlarged tail of the appendix measuring 8 mm in diameter (Figure 1B).
A colonoscopy with a biopsy from the cecal mass was subsequently performed revealing a moderately differentiated adenocarcinoma. Given the patient's good performance status, surgery was offered to the patient. A right hemicolectomy was then performed. Grossly, the cecum contained a fungating purple-pink mass measuring 3.7 cm in the greatest dimension that did not appear to involve the appendiceal orifice. The appendix was 4.7 cm in length with mildly enlarged at the tail measuring 1 cm in diameter.

Radiographic findings. A) Axial computed tomography (CT) image without contrast showing a cecal mass (large open arrow) causing obstruction of the terminal ilium (white solid arrow) and a normal sized proximal appendix measuring 6 mm in diameter (thin white arrow). B) Coronal CT image without contrast showing a mildly enlarged tail of the appendix measuring 8 mm in diameter (thin white arrow) and a cecal mass (large open arrow).
Microscopic examination of the resected cecum revealed a moderately differentiated adenocarcinoma, intestinal type (Figure 2A), with invasion through the mascularis propria into the serosa. Eight of fifteen regional lymph nodes were positive for metastatic adenocarcinoma. The tumors' cells were diffusely positive for cytokeratin-20 (CK20) and CDX2 and negative for synaptophysin and chromogranin. The immunohistochemistry of four mismatch repair proteins (MLH1, MSH2, MSH6 and PMS2) showed intact expression, suggesting that the patient did not have Lynch syndrome.
Microscopic examination of the resected appendix revealed a collision tumor (Figure 3A-B) of a well-differentiated neuroendocrine tumor (NET) (Figure 2B) and a Schwann cell hamartoma (Figure 2C) at the tip of the appendix. The NET cells were diffusely positive for synaptophysin (Figure 3D, left), chromogranin, CDX2 (Figure 3D, right) and partially positive for pan-cytokeratin but negative for CK7, CK20 and carcinoembryonic antigen (CEA). The Schwann cell hamartoma cells were diffusely positive for S100 (Figure 3C) but negative for CD117 and desmin. In addition, a separate sessile serrated adenoma that was 0.7 cm in the greatest dimension was also seen in the middle of the appendix (Figure 2D). The final histologic diagnoses of this right hemicolectomy include four primary neoplastic lesions of moderately differentiated adenocarcinoma of the cecum, sessile serrated adenoma of the appendix and a collision tumor composed of a well-differentiated neuroendocrine tumor and Schwann cell hamartoma. Following surgery, the patient was referred to palliative care since she was not a good candidate for systemic therapy given her age.
Discussion
The most commonly accepted criteria for the diagnosis of multiple primary neoplasms (MPNs) was proposed by Warren and Gates in 1932 (4): each tumor must be anatomically distinct from the others, they must have distinctively different histology and metastasis must be excluded. MPNs are known to occur in many different organ systems (3, 5) but are more commonly seen in the gynecologic (6, 7, 8) and gastrointestinal tracts (9, 10). This is most likely because they are derived from the same embryonic layer or tissue and, in the case of gynecologic malignancies, responsive to the same hormones.
The etiology of MPNs is still unclear at this time but, for some patients, could be explained by the presence of carcinogenetic risk factors. For instance, a heavy cigarette smoker will have an increased risk of developing lung, stomach, liver, kidney, uterine cervix and urinary bladder cancer (11). Other risk factors include previous cancer treatment, such as radiotherapy or chemotherapy, immunosuppression and hereditary predisposition (12). For patients without known risk factors, such as ours, MPNs may simply be due to advanced age as the risk of cancer increases with age.
The exact prevalence of patients diagnosed with at least two, non-metastatic, primary cancers varies significantly in the literature. This wide variation may be due to several factors, including different criteria to define MPNs depending on author. Furthermore, some reports are autopsy series which report higher frequency of MPNs compared to retrospective clinical case series. Demandante et al. (1) performed a literature review of over one million cancer patients diagnosed from 1966 to 2000 and found the overall occurrence rate of MPNs to be between 0.73% and 11.7%. In addition, a Surveillance, Epidemiology, and End Results (SEER) analysis revealed that second- or higher-order malignancies made up 16% of new cancer diagnoses (2). The incidence of MPNs will likely increase in the future given better access to care, an aging population and improved diagnostic techniques and treatment protocols that will lead patients living long enough to develop additional cancers (2).

Histological examination. A) The cecal tumor showed moderately differentiated adenocarcinoma. B) Histologic sections of the resected appendix demonstrated a collision tumor composed of well-differentiated neuroendocrine tumor (NET) cells with monotonous nuclei and characteristic “salt and pepper” chromatin along with a Schwann cell hamartoma (C) composed of benign-appearing spindle cells with elongated, tapering nuclei. D) Histologic sections from the distal 1/3 of the appendix also demonstrated a sessile serrated adenoma with characteristic ‘boot-shaped’, horizontally branching basal crypt architecture (Hematoxylin and eosin (H&E) staining; A, 200×; B and C, 400×; and D, 100×).
Depending on the time interval of diagnosis, MPNs can be synchronous or metachronous. Synchronous tumors are diagnosed simultaneously or within 6 months of one another, while metachronous tumors are diagnosed at least 6 months apart (4). Synchronous tumors are much rarer than metachronous tumors. A retrospective analysis at a Turkish oncology center revealed that, out of 130 MPNs cases, only 18.4% were synchronous (13). In addition, a Minneapolis Veterans Affair tumor registry from 2005 to 2009 revealed that, out of 506 patients with MPNs, 24.3% had synchronous tumors (14).
Triple synchronous MPNs are an extremely rare occurrence with only a few cases reported in the literature (6, 7, 8, 15, 16). To our knowledge, there have only been four cases (including the present case) of synchronous MPNs (3, 5, 17). In our case, three of the four neoplasms were located in the appendix. Of these, two were a collision tumor of neuroendocrine tumor and Schwann cell hamartoma.
Tumors located in the same organ with composite features of different histologic characteristics are divided into two distinct morphologic groups (18). Two histologically distinct tumors with a clear boundary between the two components is a collision tumor. In contrast, if there is intermingling between the components it is a composite (mixed) tumor. For our patient, there was no evidence of transition between the neuroendocrine and Schwann cell hamartoma components making it more consistent with a collision tumor than a composite tumor.
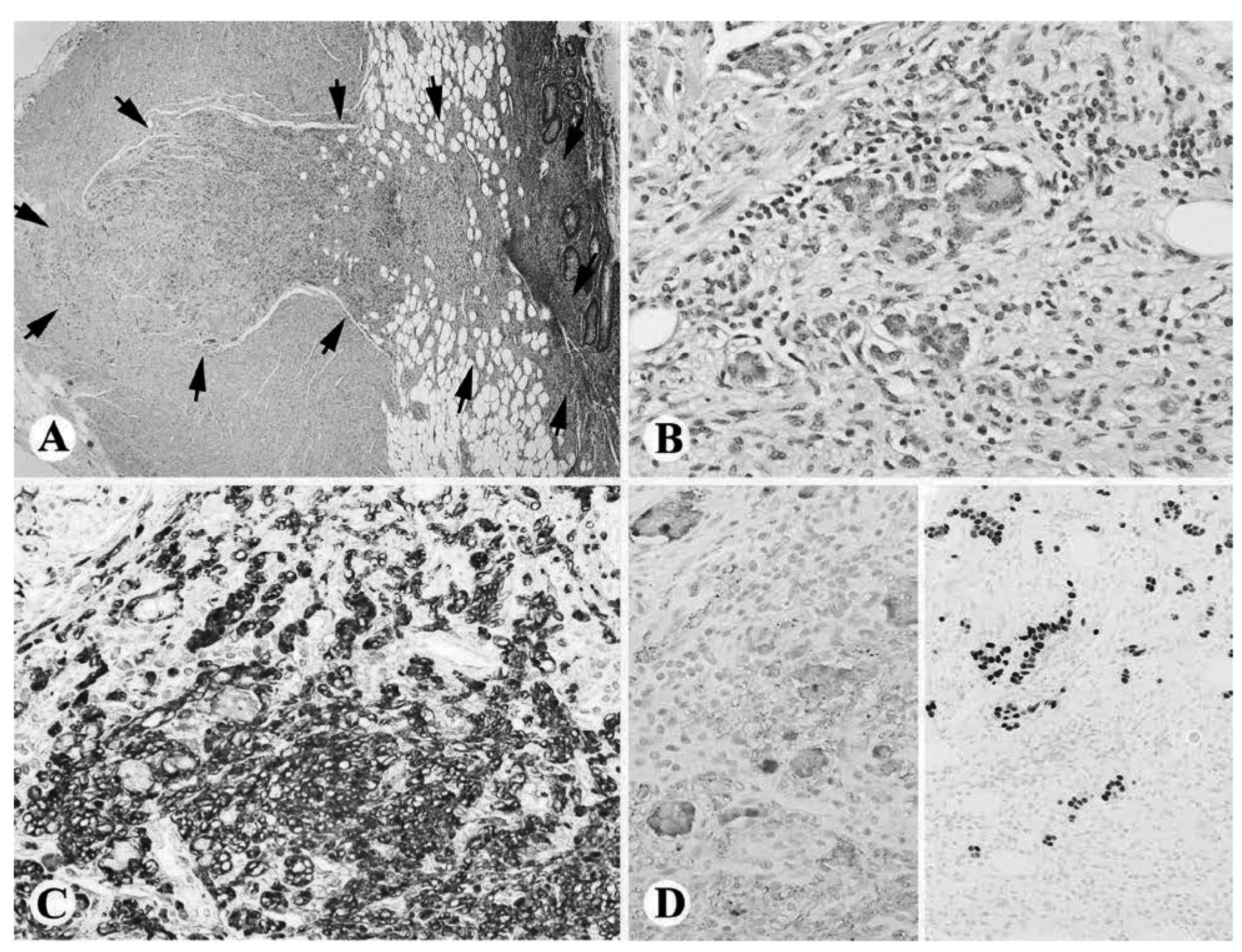
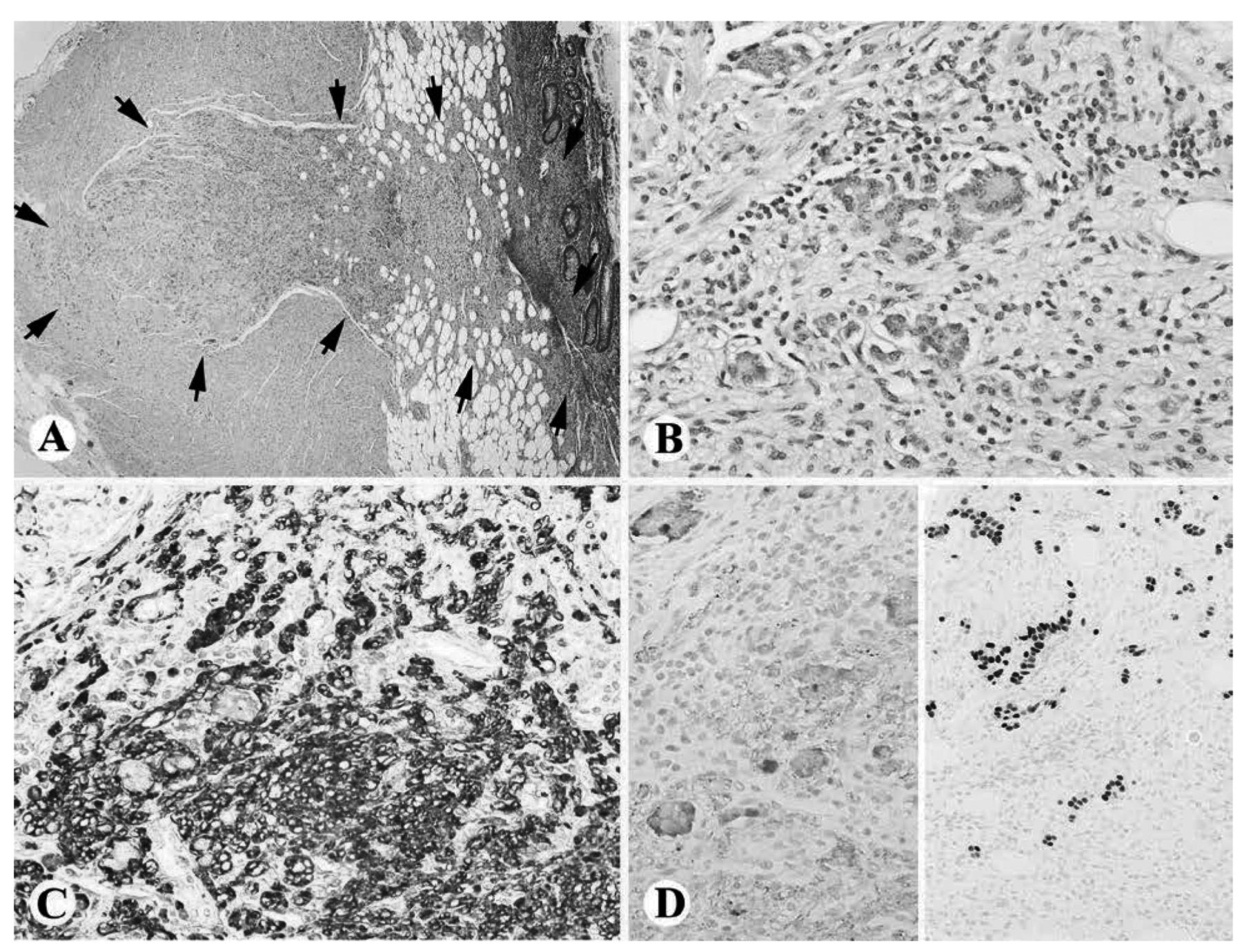
Collision tumor of the appendix. A) Low power view of the appendiceal collision tumor (outlined by black arrows, Hematoxylin and Eosin (H&E) staining, 40×). B) High power view of the collision tumor demonstrated distinctly different cell populations of spindle cell Schwann cell hamartoma cells and acinar arrangement of the round neuroendocrine tumor (NET) cells (H&E, 400×). C) The Schwann cell hamartoma cells were diffusely positive for S100 (400×). D) The NET cells were positive for synaptophysin (left) and CDX2 (right) (400×).
The etiology of collision and composite tumors is currently not fully understood. Most likely, collision tumors arise from cells of a different clonal origin (19), whereas composite tumors arise from a multipotent stem cell that is capable of bi-directional differentiation (20). While composite tumors of the gastrointestinal tract are rare, they appear to be most common in the appendix (19). Collison tumors of the appendix are even rarer with only four cases previously reported (19, 21, 22, 23). The histologic finding of collision tumors are relevant for the prognosis and treatment of the patient because usually the most aggressive component will determine disease progression (23).
Footnotes
Conflicts of Interests
The Authors declare that they have no financial conflicts.
- Received June 4, 2016.
- Revision received June 24, 2016.
- Accepted July 4, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Collision Tumors of the Gastrointestinal Tract: A Systematic Review of the Literature
- Synchronous Pancreatic Ductal Adenocarcinoma and Hepatocellular Carcinoma: Report of a Case and Review of the Literature
- Neuroendocrine Neoplasms of the Appendix: A Review of the Literature
- Triple synchronous primary malignancies: a rare occurrence
- Synchronous Type 1 Papillary Renal Cell Carcinoma in a Patient with Rectal Adenocarcinoma